Full Text
Introduction
Post operative pain is mostly managed with epidural local anaesthetics. Besides providing adequate post operative analgesia epidural techniques increases functional ability, early mobilization and earlier restoration of bowel function [1]. Pulmonary and cardiac morbidity are found to be less, and stress response to surgery is lower in postoperative epidural analgesia. It confers good analgesic quality with minimal side effects.
Orthopaedic procedures are associated with severe intraoperative and postoperative pain. It is important to achieve optimal pain control since this will facilitate more rapid achievement of functional outcome.
Chemical structure of bupivacaine and ropivacaine are almost identical except that a propyl group is attached with the pipechol ring in ropivacaine instead of butyl group in bupivacaine. Thus, ropivacaine is a smaller molecule than bupivacaine. Since the potential for toxicity of ropivacaine is less, it is widely used in situations where there is high chance of systemic toxicity due to overdosing or accidental intravascular injections as in epidural and peripheral nerve blocks [2]. The analgesic potency of ropivacaine is around 60% of that of bupivacaine [3].
Continuous infusion of epidural analgesics helps to maintain the level of analgesia and thereby reduces the adverse effects of bolus doses of local anaesthetics and opioids [4].
In initial studies using dilute concentrations of epidural ropivacaine and bupivacaine in volunteers, similar sensory blocking potency and decreased motor blockade was noticed for ropivacaine. This showed a superiority of ropivacaine for rapid patient mobilization than bupivacaine. However, studies in postoperative patients and patients receiving epidural infusion for labor analgesia have shown conflicting results.
Relative potencies of epidural ropivacaine vs bupivacaine for postoperative analgesia are still unclear and most of the comparisons were masked by the addition of epidural opioids and other adjuvants. Hence a comparison study is conducted for postoperative pain in lower limb orthopaedic procedures with plain ropivacaine and bupivacaine administered epidurally.
Materials and methods
After obtaining institutional ethical committee approval a prospective randomized controlled study was conducted in Meenakshi Mission Hospital and Research Centre, Madurai over a period of 3 years. The study was conducted five years ago and informed consent was obtained from all patients.
Inclusion criteria: Sixty patients in the age group of 20 to 60 years of either sex coming under ASA class I and II with weight between 40 to 75 kgs and height between 150 centimeters to 180 centimeters posted for elective unilateral lower limb surgeries were included in this study.
Exclusion criteria: Patients not willing to participate in the study, having infection at the site of injection, those having coagulation disorders, renal or hepatic diseases, those allergic to local anaesthetics and those undergoing emergency surgeries were excluded from the study.
All sixty patients were assigned randomly on the basis of computerized randomization chart into two Groups - A and B. Each group had thirty patients. Pre- anaesthetic check up with routine haemogram, chest x-ray and electrocardiogram along with any additional investigations were done depending upon the individual requirements. Patients were educated to interpret the visual analogue scale (VAS) preoperatively. After confirming adequate starvation and written informed consent patients were shifted to the operating room. Routine monitoring with electrocardiogram, pulse oximetry and noninvasive blood pressure was done and baseline parameters recorded. Patients were preloaded with 750ml of Ringer’s Lactate solution. Under proper aseptic precautions, in sitting position a 16-gauge Tuohy’s epidural needle is inserted in lumbar area using loss of resistance technique. Once position is confirmed an18 gauge epidural catheter is inserted and fixed such that 6cm of the catheter remains inside the epidural space. Test dose of 3 ml of 2% lignocaine with 15 micrograms of adrenaline was given. Lumbar subarachnoid block was used for the surgical procedures using 0.5% bupivacaine heavy and epidural boluses were given after two hrs of subarachnoid block.
Post operatively patients were shifted to High Dependency Unit with echocardiogram, pulse oximetry and non-invasive blood pressure monitoring. Epidural infusion of allotted drug was started at the rate of 6 ml/hour when the patients were able to do flexion of the opposite limb. Heart rate, blood pressure, visual analogue score, top up analgesia and side effects were recorded post-operatively for 48 hrs after the commencement of epidural infusion. VAS score > 3 was taken as trigger to give additional analgesia which was prefixed as 100mg of tramadol intravenous boluses along with 0.15mg/kg of intravenous ondansetron in our study.
Statistical tools
Software used for statistical analysis was Epidemiological Information Package; (EPI info. 2010) developed by CDC, Atlanta. Mean with standard deviation or range were used for continuous variables. Frequencies and percentage were used for categorical variables. Chi Square and ‘p’ values were calculated. Significant difference in quantitative values were tested with Kruskal- Wallis’s chi-square test. For qualitative variables- Yate’s chi-square test was used. ‘p’ value of <0.05 was taken as statistically significant difference.
Results
Demographic characters like age (Table 1), sex, height and weight were similar in both groups. The mean age of patients in ropivacaine group was 40.2 ± 13.1 years and bupivacaine group were 39.3 ± 12.6 years. Mean height of patients in Group A was 165.9 ± 6.4 centimeters and for Group B was 164.9 ±7.2 centimeters. ASA class of I and II were included in our study and they showed no statistically significant difference between the two groups (Table 2).
Table 1: Age distribution.
|
Age
|
Group A
|
Group B
|
p value
|
|
Number of patients
|
%
|
Number of patients
|
%
|
|
20 – 29 years
|
8
|
26.7
|
7
|
23.3
|
0.7335
|
|
30 – 39 years
|
8
|
26.37
|
9
|
30
|
|
40 – 49 years
|
6
|
20
|
5
|
16.7
|
|
50 years & above
|
8
|
26.7
|
9
|
30
|
|
Total
|
30
|
100
|
30
|
100
|
|
Range in years
|
21 – 60
|
21 -60
|
|
Mean in years
|
39.3
|
40.2
|
|
Standard deviation
|
±12.6
|
±13.1
|
Note: Age group of patients included in the study were similar in the two groups with no statistically significant difference.
Table 2: American society of Anaesthesiologists physical status of the patients.
|
ASA
|
Group A
|
Group B
|
p value
|
|
No.
|
%
|
No.
|
%
|
|
Ⅰ
|
19
|
63.3
|
20
|
66.7
|
1
|
|
Ⅱ
|
11
|
36.7
|
10
|
33.3
|
|
Total
|
30
|
100
|
30
|
100
|
The type of procedures included in the two groups were comparable statistically (Table 3). Duration of procedure for Group A was 153.7 ± 34.9 min and for Group B was 160.5 ± 40.7 min (Table 4). This difference was not statistically significant (p value= 0.4771). Mean heart rate did not have any statistically significant difference at various time intervals among the two groups (Figure 1).
Table 3: Procedures underwent by the patients in the study.
|
Procedure
|
Group A
|
Group B
|
|
No
|
%
|
No
|
%
|
|
Arthroscopy
|
2
|
6.7
|
2
|
6.7
|
|
Core decompression and bone grafting
|
-
|
-
|
1
|
3.3
|
|
External fixation
|
3
|
10
|
2
|
6.7
|
|
Flap cover
|
-
|
-
|
1
|
3.3
|
|
Hemiarthroplasty
|
-
|
-
|
1
|
3.3
|
|
Illizarov fixation
|
3
|
10
|
6
|
20.0
|
|
Intramedullary nailing
|
11
|
36.7
|
6
|
20.0
|
|
Open reduction with internal fixation femur
|
3
|
10
|
5
|
16.7
|
|
Open reduction with internal fixation tibia
|
3
|
10
|
3
|
10.0
|
|
Osteoarthritis knee
|
1
|
3.3
|
-
|
-
|
|
Percutaneous femoral nailing
|
1
|
3.3
|
-
|
-
|
|
Plasmacytoma femur
|
1
|
3.3
|
-
|
-
|
|
Tension band wiring patella
|
-
|
-
|
1
|
3.3
|
|
Total hip replacement
|
2
|
6.7
|
-
|
-
|
|
TKR
|
-
|
-
|
2
|
6.7
|
|
Total
|
30
|
100
|
30
|
100
|
Note: The types of procedures included in the study for the two groups were statistically similar.
Table 4: Duration of procedures.
|
Group
|
Duration of procedure (min)
|
p value
|
|
Range
|
Mean
|
S.D.
|
|
A
|
100 - 240
|
153.7
|
±34.9
|
0.4771
|
|
B
|
90 - 285
|
160.5
|
±40.7
|
Note: Mean duration of the procedures underwent by patients in each group were comparable statistically.
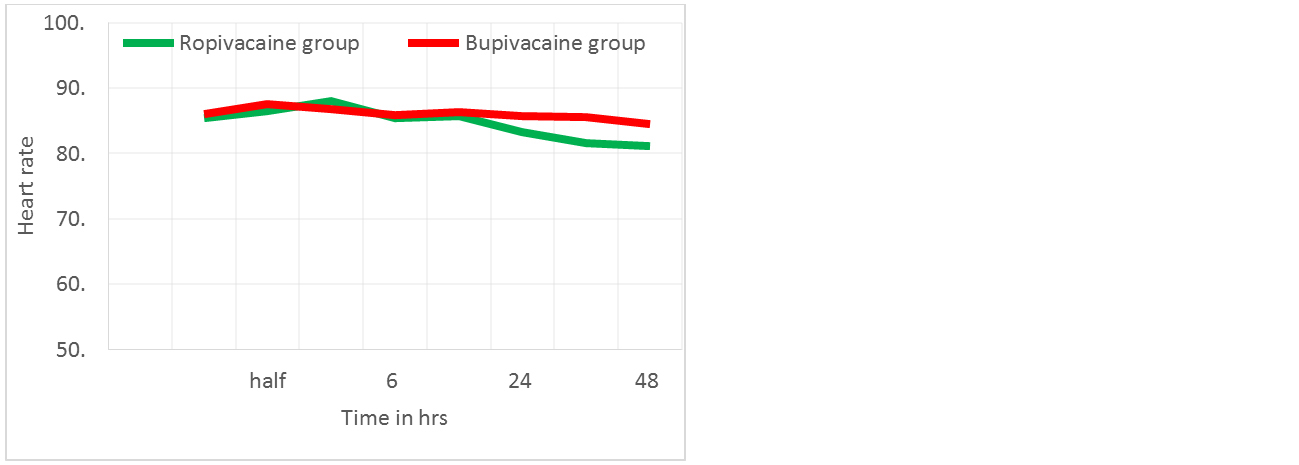
Figure 1: Variations in heart rate. No statistical significance noted at different time intervals in mean heart rate of both groups.
Systolic and diastolic blood pressure were recorded at various time interval for patients belonging to both groups and no statistically significant difference was noted (Tables 5 and 6). Pain was assessed using VAS score (Table 7). Throughout the observations VAS was found to higher in Group B but statistically significant difference was found at one hour, 12 hrs and 24 hrs. At one hour mean VAS for Group B was 2.7 ± 1.78 and for Group A was 1.77± 0.86 (p value = 0.0126) which was statistically significant (Figure 2). At 12 hrs mean VAS was 2.67 ± 2.27 for Group B and 1.47 ± 1.36 for Group A and at 24 hrs mean VAS was 1.73 ± 1.93 and 0.83 ± 1.39 respectively for Groups B and A. The p value was 0.031 at 12 hrs and 0.042 at 24 hrs and both showed significant difference statistically. Additional analgesic requirement was also assessed postoperatively. A statistically significant difference was noted at 12 hrs with a p value of 0.0153 and was found to be more for Group B patients (Table 8, Figure 3).
Table 5: Variations in systolic blood pressure (SBP).
|
SBP
|
Group A
|
Group B
|
p value
|
|
Mean
|
S.D.
|
Mean
|
S. D
|
|
Baseline
|
120
|
±10.8
|
118.3
|
±10.2
|
0.4821
|
|
30 min
|
121.3
|
±10.1
|
118.5
|
±10.0
|
0. 2994
|
|
1 h
|
121.4
|
±8.4
|
118.8
|
±8.7
|
0. 1942
|
|
6 hrs
|
120.7
|
±10.2
|
118.6
|
±7.4
|
0.435
|
|
12 hrs
|
118.6
|
±8.9
|
121.7
|
±7.1
|
0. 0658
|
|
24 hrs
|
117.9
|
±7.8
|
120.9
|
±8.2
|
0. 1844
|
|
36 hrs
|
121.1
|
±7.3
|
121.3
|
±8.3
|
0. 5574
|
|
48 hrs
|
121.2
|
±8.3
|
121.1
|
±7.7
|
0. 9807
|
Note: Systolic blood pressure recorded in the two groups had no significant difference statistically.
Table 6: Variations in diastolic blood pressure.
|
Diastolic blood pressure
|
Group A
|
Group B
|
p value
|
|
Mean
|
S.D.
|
Mean
|
S. D
|
|
Baseline
|
76.5
|
±9.2
|
75.0
|
±6.8
|
0.4977
|
|
30 min
|
77.9
|
±8.5
|
75.7
|
±6.1
|
0.4551
|
|
1 h
|
75.9
|
±8.2
|
76.2
|
±6.7
|
0.6826
|
|
6 hrs
|
75.9
|
±7.2
|
76.1
|
±6.8
|
0.8711
|
|
12 hrs
|
75.7
|
±7.5
|
77.4
|
±7.4
|
0.3664
|
|
24 hrs
|
75.7
|
±7.3
|
75.2
|
±6.2
|
0.7103
|
|
36 hrs
|
75.1
|
±7.2
|
75.2
|
±6.6
|
0.8897
|
|
48 hrs
|
75.9
|
±6.7
|
75.3
|
±6.3
|
0.8048
|
Note: Diastolic blood pressure recorded among the two groups showed no significant difference.
Table 7: Changes in visual analogue score.
|
VAS
|
Group A
|
Group B
|
p value
|
|
Mean
|
S.D
|
Mean
|
S.D
|
|
Baseline
|
0.93
|
±1.36
|
1.53
|
±1.25
|
0.1018
|
|
30 min
|
1.73
|
±1.39
|
2.43
|
±1.94
|
0.1786
|
|
1 h
|
1.77
|
±0.86
|
2.7
|
±1.78
|
0.0126
|
|
6 hrs
|
2.03
|
±1.03
|
2.37
|
±1.5
|
0.1081
|
|
12 hrs
|
1.47
|
±1.36
|
2.67
|
±2.27
|
0.0311
|
|
24 hrs
|
0.83
|
±1.39
|
1.73
|
±1.93
|
0.042
|
|
36 hrs
|
0.73
|
±1.08
|
1.23
|
±1.41
|
0.1422
|
|
48 hrs
|
0.6
|
±1.04
|
1.27
|
±1.46
|
0.058
|
Note: Mean pain perception was higher for ropivacaine group with significant difference at one hour, twelve hrs, and twenty-four hrs of the study.
Table 8: Requirement of top-up analgesic.
|
No. of cases requiring additional analgesic
|
Group A
|
Group B
|
p value
|
|
No
|
%
|
No.
|
%
|
|
30 min
|
1
|
3.3
|
4
|
13.3
|
0.1766
|
|
1 h
|
Nil
|
Nil
|
3
|
10
|
0.1186
|
|
6 hrs
|
1
|
3.3
|
Nil
|
Nil
|
0.5
|
|
12 hrs
|
1
|
3.3
|
9
|
30
|
0.0153
|
|
24 hrs
|
1
|
3.3
|
4
|
13.3
|
0.1766
|
|
36 hrs
|
Nil
|
Nil
|
Nil
|
Nil
|
-
|
|
48 hrs
|
Nil
|
Nil
|
Nil
|
Nil
|
-
|
Note: Rescue analgesic requirement for ropivacaine was 30% as opposed to 3.3% for bupivacaine group with a p value of 0.0153 showing statistically significant difference at 12 hrs after epidural infusion
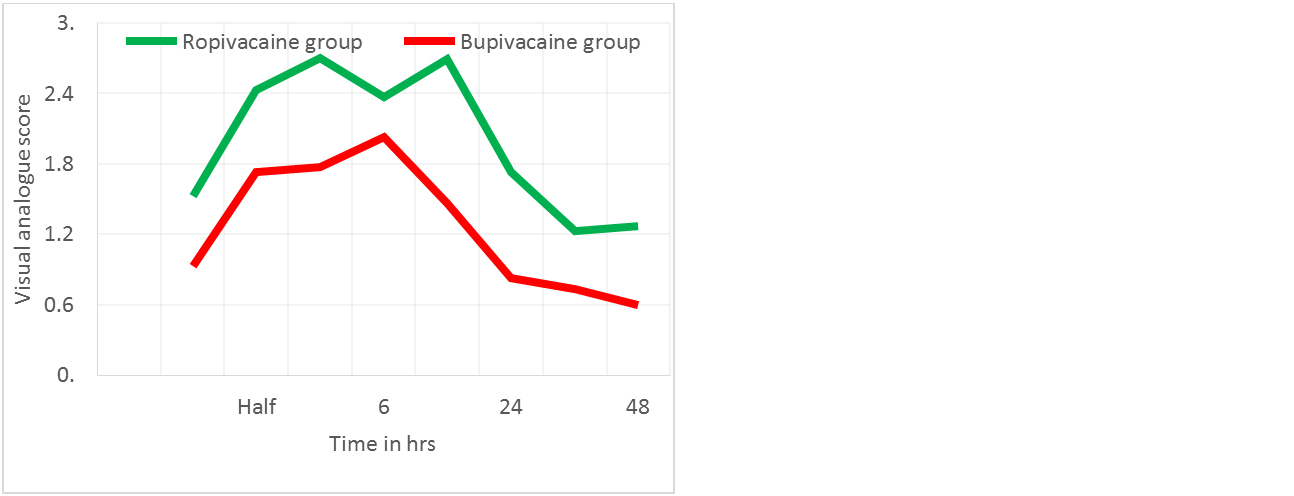
Figure 2: Visual Analogue scale variations. Statistically significant increase in pain perception was noted at one hour, twelve hrs and twenty-four hrs after starting epidural infusion for ropivacaine group of patients than bupivacaine group.
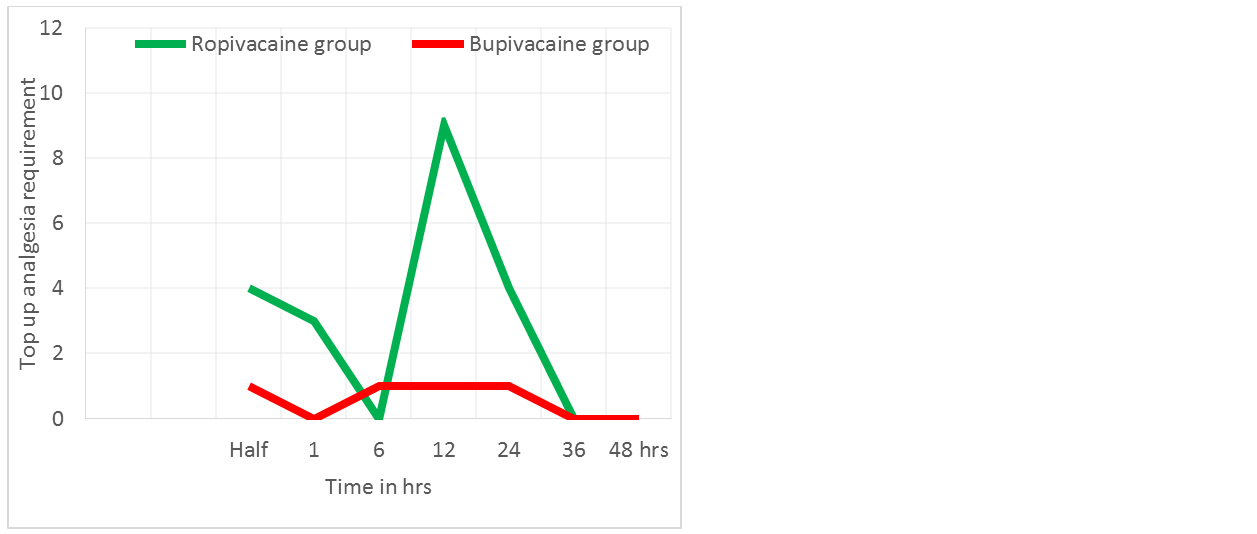
Figure 3: Requirement of top-up analgesia. Statistically significant top up analgesic requirement was noted at 12 hrs with ropivacaine group requiring more rescue analgesia than bupivacaine group.
Discussion
Multimodal analgesia plays a major role in the management of postoperative pain. Inadequate analgesia prolongs the duration of hospital stay and increases morbidity as well as mortality in the perioperative period. Epidural analgesics are largely employed in the management of pain both acute and chronic. Epidural analgesia was used in paediatric patients as well as in sepsis [5].
Bupivacaine was initially used commonly for providing epidural analgesia. Later ropivacaine and levo-bupivacaine the S enantiomer came into use to reduce the cardiac side effects of bupivacaine. Ropivacaine was found to be less cardiotoxic than bupivacaine and, therefore, can be safely used in intra articular analgesia (Piper et al). Most studies comparing bupivacaine and ropivacaine in post-operative epidural analgesia are clouded by the addition of adjuvants like opioids, clonidine, dexmedetomidine etc [7-10]. In our study we compared plain ropivacaine and bupivacaine.
Demographic profile of patients included in the two groups in our study were comparable. This included the age, sex, height and weight of the patients. Our study included patients in ASA Ⅰ and Ⅱ groups only as higher ASA grades are more prone for hemodynamic instability and other complications. We conducted the study in lower limb orthopedic procedures with comparable durations.
The analgesic potency of ropivacaine is nearly 1 to 1.5 times less than that of bupivacaine. We used 0.2% solution of ropivacaine and 0.125% solution of bupivacaine so as to achieve an equipotent dose. Stefan et al., compared ropivacaine and bupivacaine in thoracic epidural in patients undergoing open renal surgery and the concentrations compared were similar to that of our study [3]. Study conducted by Kanai et al in lower limb surgical procedures used 0.125% bupivacaine, 0.2% and 0.1% ropivacaine [11].
The rate of epidural infusion in our study was fixed as 6ml/hr as per institutional protocol. Kanai et al used a continuous epidural infusion of 6ml/hr. Soliman et al compared the effect of adding dexmedetomidine and fentanyl to bupivacaine in postoperative pain relief in patients undergoing total knee replacement surgeries using a continuous epidural infusion at 5ml/hr [12].
Heart rate and blood pressure changes showed no statistical significance. There were no significant variations in heart rate and blood pressure like bradycardia or hypotension throughout the postoperative observations.
Analgesic efficacy of the drugs was compared using ten-point Visual Analogue Scale. Trigger point for additional analgesics were taken as three for our study. Our analysis showed that the efficacy of 0.2% ropivacaine with regards to analgesia is less when compared with 0.125% bupivacaine. Bhasin et al compared 0.125% bupivacaine with 0.1% ropivacaine and 0.2% ropivacaine for postoperative analgesia in total knee replacement surgeries [13]. They found 0.2% ropivacaine and 0.125% bupivacaine equally efficacious in terms of VAS pain scores. Stefan et al compared similar concentrations of both drugs as used in our study and found the pain scores were similar in both groups which were in contrast to the findings of our study [3]. Beilin et al., compared the same drugs in epidural labor analgesia and found similar analgesic effect [14]. Muldoon et al used a Visual Analogue Scale of 100 points and found the scores to be 0 - 13.3 for ropivacaine group and a score of 0 - 0.5 for bupivacaine group [15]. Jorgensen et al., compared the two drugs and found bupivacaine to better in providing analgesia than ropivacaine when both the drugs were used at 0.2% concentrations [16]. Khanna et al., compared both drugs in epidural by adding fentanyl as adjuvant for total knee replacement surgeries and found ropivacaine with fentanyl having superior analgesic efficacy than bupivacaine and fentanyl using patient controlled epidural analgesia technique [17].
In our study 100mg of tramadol was given intravenously when VAS score of the patients were found to be more than three. Higher requirement of additional analgesic top-up was noted in patients receiving ropivacaine infusions throughout the observation period. These were not significant statistically except at 12 hrs. Our observations match with the study conducted by Heid et al., where they found the local anaesthetic consumption was 60% higher in ropivacaine group (1372.5 ± 108.3mg) than bupivacaine group (85.2 ± 75.2mg) with a p value of < 0.001 [18]. Jorgensen et al produced similar results [15]. Pasquele de Negri et al found ropivacaine to be more effective than bupivacaine in children in a study conducted for post operative pain management for hypospadias repair, but this was based on the motor effects produced by bupivacaine [19]. Their analysis showed similar analgesic efficacy among ropivacaine, bupivacaine and levo-bupivacaine. We did not encounter any local anaesthetic systemic toxicity or other side effects during our study.
Limitations of the study
The study was conducted in a small population and limited to orthopaedic procedures only, so the findings cannot be extrapolated to the whole population. Though we assessed the motor power of the patients by asking them to move the limb and started physiotherapy we did not ambulate the patient for 48 hrs, so we were unable to assess the effects on ambulation of the patients postoperatively.
Conclusion
Ropivacaine and bupivacaine can be used as epidural infusions for providing adequate pain relief after orthopaedic surgeries. The analgesia provided by 0.125% bupivacaine is better than 0.2% ropivacaine as the bupivacaine group showed lower pain score and required less rescue analgesics. No significant side effects were noted with both drugs showing that both drugs are equally safe at the above concentrations. Hence the findings of the present study support the use of epidural bupivacaine (0.125%) over ropivacaine (2%).
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Cho JS, Kim HI, Lee KY, Son T, Bai SJ, et al. Comparison of the effects of patient-controlled epidural and intravenous analgesia on postoperative bowel function after laparoscopic gastrectomy: a prospective randomized study. Surg Endosc. 2017; 31(11):4688–4696.
[2] Casati A, Putzu M. Bupivacaine, levobupivacaine and ropivacaine: are they clinically different? Best Pract Res Clin Anaesthesiol. 2005; 19(2):247–268.
[3] Girsberger SA, Schneider MP, Löffel LM, Burkhard FC, Wuethrich PY. Effect of thoracic epidural ropivacaine versus bupivacaine on lower urinary tract function: A randomized clinical trial. Anesthesiology. 2018; 128:511–519.
[4] Wheatley RG, Schug SA, Watson D. Safety and efficacy of postoperative epidural analgesia. Br J Anaesth. 2001; 87(1):47–61.
[5] Kotzé A, Hinton W, Crabbe DC, Carrigan BJ. Audit of epidural analgesia in children undergoing thoracotomy for decortication of empyema. Br J Anaesth. 2007; 98(5):662–666.
[6] Piper SL, Kim HT. Comparison of ropivacaine and bupivacaine toxicity in human articular chondrocytes. J Bone Joint Surg Am. 2008; 90(5):986–991.
[7] Forster JG, Rosenberg PH. Small dose of clonidine mixed with low-dose ropivacaine and fentanyl for epidural analgesia after total knee arthroplasty. Br J Anaesth. 2004; 93(5):670–677.
[8] Bajwa SJS, Kaur J, Bajwa SK, Bakshi G, Singh K, et al. Caudal ropivacaine-clonidine: A better post-operative analgesic approach. Indian J Anaesth. 2010; 54(3):226–230.
[9] Paul A, Nathroy A, Paul T. A comparative study of dexmeditomidine and fentanyl as an adjuvant to epidural bupivacaine in lower limb surgeries. J Med Sci. 2017; 37:221–226.
[10] Alansary AM, Elbeialy MAK. Dexmedetomidine versus Fentanyl added to bupivacaine for epidural analgesia in combination with general anesthesia for elective lumbar disc operations: A prospective, randomised double-blinded study. Saudi J Anaesth. 2019; 13(2):119–125.
[11] Kanai A, Nakahara R, Okamoto H, Hoka S. Postoperative analgesia using continuous lumbar epidural infusion of ropivacaine in comparison with bupivacaine. Masui. 2003; 52(8):832–839.
[12] Soliman R, Eltaweel M. Comparative study of dexmedetomidine and fentanyl as an adjuvant to epidural bupivacaine for postoperative pain relief in adult patients undergoing total knee replacement: A randomized study. J Anesthesiol Clin Sci. 2016; 5:1.
[13] Bhasin S, Dhar M, Sreevastava DK, Nair R, Chandrakar S. Comparison of efficacy of epidural ropivacaine versus bupivacaine for postoperative pain relief in total knee replacement surgeries. Anesth Essays Res. 2018; 12(1):26–30.
[14] Beilin Y, Halpern S. Ropivacaine versus bupivacaine for epidural labor analgesia. Anesth Analg. 2010; 111(2):482–487.
[15] Muldoon T, Milligan K, Quinn P, Connolly DC, Nilsson K. Comparison between extradural infusion of ropivacaine or bupivacaine for the prevention of postoperative pain after total knee arthroplasty. Br J Anaesth. 1998; 80(5):680–681.
[16] Jørgensen H, Fomsgaard JS, Dirks J, Wetterslev J, Dahl JB. Effect of continuous epidural 0.2% ropivacaine vs 0.2% bupivacaine on postoperative pain, motor block and gastrointestinal function after abdominal hysterectomy. Br J Anaesth. 2000; 84(2):144–150.
[17] Khanna A, Saxena R, Dutta A, Ganguly N, Sood J. Comparison of ropivacaine with and without fentanyl vs bupivacaine with fentanyl for postoperative epidural analgesia in bilateral total knee replacement surgery. J Clin Anest. 2017; 37:7–13.
[18] Heid F, Schmidt-Glintzer A, Piepho T, Jage J. Epidural ropivacaine - Where are the benefits? A prospective, randomized, double-blind trial in patients with retropubic prostatectomy. Acta Anaesthesiol Scand. 2007; 51(3):294–298.
[19] De Negri P, Ivani G, Tirri T, Modano P, Reato C, et al. A comparison of epidural bupivacaine, levobupivacaine, and ropivacaine on postoperative analgesia and motor blockade. Anesth Analg. 2004; 99(1):45–48.