Short Communications
2015
December
Volume : 3
Issue : 4
Analysis of vitamin B12 and D deficiency and the effect of supplementation on patients at tertiary care hospital
Srinivasa Rao B, Sakuntala Devi G, Kavitha K, Kanaka Bhushanam GVVS
Pdf Page Numbers :- 203-207
Srinivasa Rao B1,*, Sakuntala Devi G2,*,Kavitha K1 and Kanaka Bhushanam GVVS1
1KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India
2Department Obstetrics & Gynaecology (O & G), Visakhapatnam Steel General Hospital (VSGH), Visakhapatnam, AP., India
*Corresponding author: Dr. Srinivasa Rao B, M.Sc., Ph.D., KIMS Foundation and Research Centre, Minister Road, Secunderabad -500003, Telangana, India. Email: srinumicros@yahoo.co.in
Received 9 July 2015; Revised 11 September 2015; Accepted 22 September 2015; Published 29 September 2015
Citation: Srinivasa Rao B, Sakuntala Devi G, Kavitha K, Kanaka Bhushanam GVVS. Analysis of vitamin B12 and D deficiency and the effect of supplementation on patients at tertiary care hospital. J Med Sci Res. 2015; 3(4):203-207. DOI: http://dx.doi.org/10.17727/JMSR.2015/3-039
Copyright: © 2015 Srinivasa Rao B, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Vitamins are essential organic compounds for the body and the study aims to understand the extent of deficiency present among the patients tested for deficiency and the effect of supplementation. Our study also aims in understanding the effect of supplementation on treating the deficiency along with its effect on any secondary disease conditions present among the patients such as diabetes, cardiovascular disease, rheumatoid arthritis, osteoporosis and/or hypertension. Assessment was carried out in randomly selected, 500 patients from the patient pool (March 2013 to March 2015) and supplemented with vitamins at KIMS hospital, Secunderabad. Data such as biochemical measures, medications, food supplements and herbal medicines were also taken into consideration. The assessment showed improvement in deficiency symptoms after supplementation. Along with this, the improvement in general health of patients that have secondary conditions was analyzed. The study shows that patients with osteoporosis are benefited by vitamin D supplementation and supplementation seems to also helped patients with pain in case of rheumatoid arthritis. Patients with diabetes and/or cardiovascular disease did not show much improvement with supplementation. Patients with hypertension solely or with other conditions show improvement with this problem compared to other conditions. We observed that supplementation does have a role in general health improvement in patients with some chronic conditions.
Keywords: vitamin D; vitamin B12; deficiency; general health; supplementation
Full Text
Vitamins are essential organic compounds required in trace amounts (microgram to milligram quantities/ day) and play a vital role in the normal growth and functioning of the various physiological processes in the body. Vitamin B12 also known as cyanocobalamin is a water soluble hematopoietic vitamin necessary for the maturation of erythrocytes and other countless processes within the body involving DNA and cell growth. It also plays a role in cardiovascular protection and proper functioning of nervous system [1]. Its plays a pivotal role in the metabolism of carbohydrates, proteins and fats [1]. Vitamin D also known as calcitriol is a fat soluble vitamin essential in the formation and maintenance of healthy bones and teeth. It also plays a key role in absorption and metabolism of phosphorus and calcium [2]. It is necessary for proper muscle functioning, bone mineralization and stability, and multiple immune functions [2]. Vitamin D and B12 can be obtained from many natural resources. Primarily the vitamin D used by the body is produced in the skin after exposure to ultraviolet light from the sunlight. It can also be found in the fatty fish. Vitamin B12 is found in most animal derived foods, including fish and shellfish, meat (especially liver), poultry, eggs, milk, and milk products. The major causes of vitamin B12 deficiency are nutritional inadequacy or mal-absorption and elevated levels of methylmalonic acid and homocysteine.
The aim of this study is to understand the extent of deficiency present among the patients tested for deficiency at a tertiary care hospital (KIMS Hospital, Secunderabad) and the effect of supplementation. The study also aims at understanding the effect of supplementation on treating the deficiency along with its effect on any secondary disease conditions present among the patients.
Materials and methods
The distribution of males and females in the randomly selected from the patient pool of 500 patients supplemented with vitamin package was estimated from March 2013 to March 2015. Biochemical measures such as vitamin D and B12 levels were collected from the KIMS hospital database along with gender and age. Information on dietary intake (vegetarian/ non-vegetarian) was not collected. Medicines, sun exposure, food supplements and information on herbal medicines were obtained using a questionnaire (Annex 1) by telephonic discussion with the patients and this information was recorded.
The number of diagnosed deficiency cases for vitamin D/B12/B12 & D was estimated from the patient pool (500) and the effect of supplementation with vitamin package was calculated from improvement in the deficiency symptoms of the patients with no secondary condition. Among the selected pool of patients, the number of cases of cardiovascular disease, rheumatoid arthritis, hypertension, diabetes and osteoporosis cases were determined and the effect of supplementation on their disease symptoms was estimated.
Results
The study shows that 81.62% of the male population is deficient in vitamin B12 and/or D and 81.2% of females are deficient in vitamin B12 and/or D (Figure 1). In the vitamin deficient male population, 3.41% of patients were diagnosed with vitamin B12 deficiency, 50.42% with vitamin D deficiency and 27.77% with a combined vitamin B12 & D deficiency (Figure 2). In the vitamin deficient female population, 3% of patients were diagnosed with vitamin B12 deficiency, 61.27% with vitamin D deficiency and 16.91% with a combined vitamin B12 & D deficiency (Figure 2).
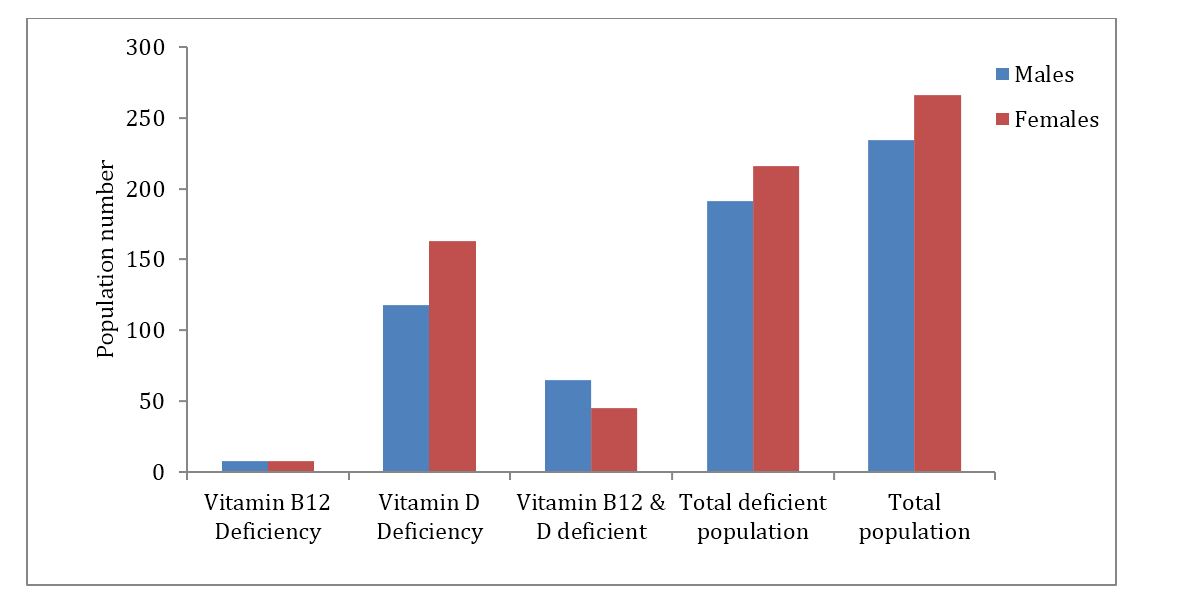
Figure 1: Vitamin B12 and D deficiency in population.
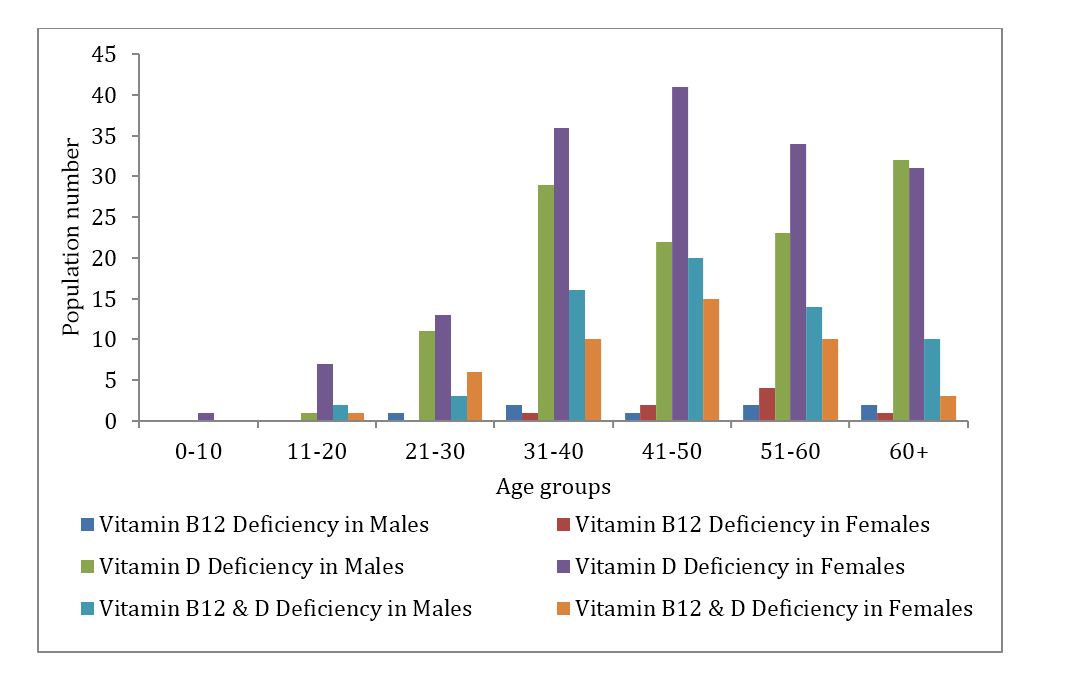
Figure 2: Vitamin B12 and D deficiency in different age groups.
Among the patients who were diagnosed and treated for vitamin deficiency, 29.48% people responded to the follow up exam. The effect of supplementation was assessed by alleviation of the physical symptoms after supplementation for patients with no secondary conditions such as hypertension, diabetes, osteoporosis, rheumatoid arthritis and/ or cardiovascular disease (Figure 3). The presence and absence of improvement among the patients was assessed along with the completion/ discontinuation of supplements, any additional measures taken by patients during the supplementation period such as alternative forms of medicine (Ayurveda/ Homeopathy), better diet and sun exposure.
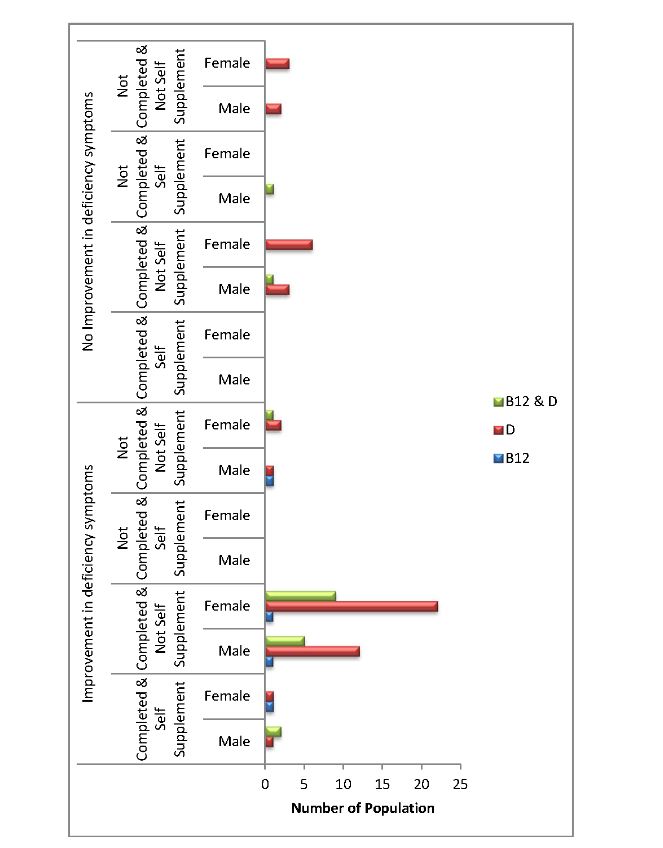
Figure 3: Improvement and non-improvement of deficient patients with no secondary conditions.
From the patient pool diagnosed with deficiency, the effect of supplementation was assessed for the ones with secondary health conditions such as hypertension (HTN), diabetes (DB), osteoporosis (OP), rheumatoid arthritis (RA) and/or cardiovascular disease (CVD). The patient pool consists of seven patients with DB and CVD each. There were nine patients with HTN and one with OP. Two patients were seen with both DB and CVD and also HTN and CVD. Four patients were diagnosed with DB and HTN. Two patients had HTN, DB and CVD. One patient had HTN, DB and RA. The number of patients with secondary conditions was estimated (Figure 4).
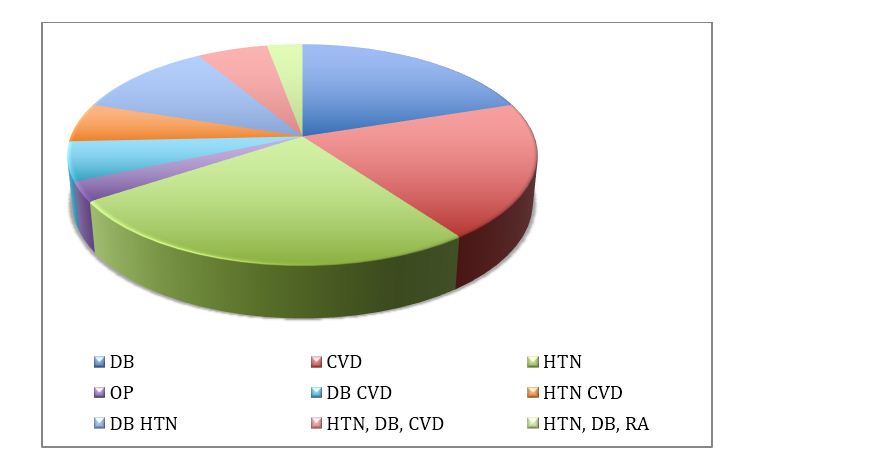
Figure 4: Distribution of patients with secondary condition.
Among these patients, the effect of supplementation was checked by the improvement in their respective conditions via telephonic discussion. In DB patients, two patients with vitamin D deficiency stated improvement in their disease condition. Four people with vitamin D deficiency and one with B12 & D deficiency did not show any improvement in their condition. Among the CVD patients, one patient with vitamin D deficiency was not sure about any improvement. One patient with vitamin D deficiency showed improvement. Four people with vitamin D deficiency and one with B12 & D deficiency did not show any improvement in their condition. Out of the nine patients with HTN, two patients showed improvement, one with vitamin D deficiency and the other with B12 & D deficiency. The seven patients, out of which three had B12& D deficiency and four with vitamin D deficiency, showed no improvement. One patient with osteoporosis showed significant improvement with vitamin D supplementation. Out of the two patients suffering from both DB and CVD, one patient with vitamin D deficiency was not sure of noting any significant improvement and the one with B12 & D deficiency stated that there was no improvement, after supplementation. Four patients had both DB and HTN, out of which only one patient with B12 & D deficiency stated that there is improvement after supplementation. One patient with vitamin D deficiency stated that the effect of supplementation was evidently seen in HTN but did not help with DB. Two patients both with vitamin D deficiency did not show any improvement. Out of the patient pool, two patients had both HTN and CVD. Both patients had shown improvement with regards to HTN but not CVD. One of them was supplemented for vitamin D deficiency and the other for vitamin B12 and D deficiency. Two patients who were diagnosed with vitamin D deficiency had HTN, DB and CVD. Both of them did not show any improvement with vitamin D supplementation. One patient with HTN, DB, and RA stated that the vitamin D supplementation helped with managing RA but not with DB and HTN. The overall effect of supplementation among these conditions was summarized (Figure 5). We observed that the deficiency symptoms where alleviated as treatment progressed and the patients who took additional measures such as sun exposure and better diet where able to sustain their vitamin levels for longer period. Depending on the patient requirement and their lifestyle factors, multiple supplementations may be required to sustain the normal levels.
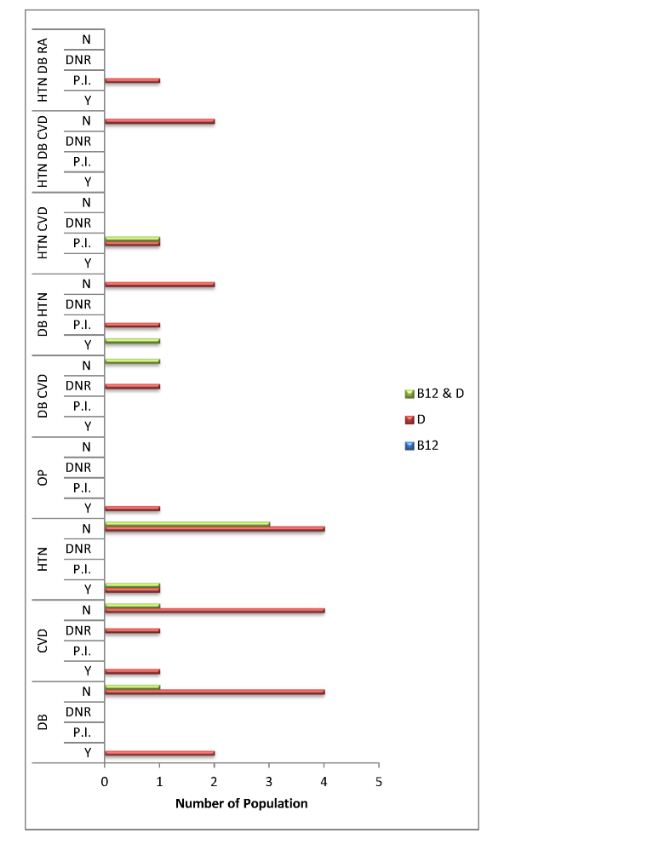
Abbreviations: Y= yes; N = no; P.I = partial improvement; DNR= did not respond
Figure 5: Improvement/ non-improvement of deficient patients with secondary conditions.
Discussion
The occurrence of the deficiency among the patients was much higher in vitamin D than B12 and similar results have been concurred by multiple studies. One of the first studies to understand the prevalence of vitamin D was examined among healthy infants and toddlers [3]. Multiple studies were carried out among Turkish, Moroccan, Indian and sub-Sahara African populations in Europe and their countries of origin [4]. The vitamin D status of studied populations in Turkey and India varied and was similar to the immigrant populations in Europe (low) and similar to or even higher than the indigenous European populations (high) [4]. Vitamin D deficiency is commonly seen among Indians and can be used as lifestyle markers to study risk association of cancer, TB, autoimmune disorders and diabetes among the population. Studies have shown the effect of vitamin D on bone health and the need for supplementation for the normal physiological maintenance of the body [2]. Our study shows that 81.62% of the male population is deficient in vitamin B12 and/or D and 81.2% of females are deficient in vitamin B12 and/or D. Among the male population, most patients got diagnosed with vitamin D deficiency followed by vitamin B12 & D deficiency and the least associated with vitamin B12 deficiency. Similar pattern of deficiency was also observed in the female population. The study shows that the majority of the population is either vitamin D deficient or has B12 deficiency along with D. Vitamin D deficiency can possibly be associated with inadequacy of sun exposure due to lifestyle factors. This life style factor also involves processed food consumption, which contributes to nutritional inadequacy leading to B12 deficiency. Another study in the South Indian population has shown the association of vitamin D deficiency and hyperthyroidism [6]. Since hyperthyroidism is associated with increased rate of bone remodeling & changes in mineral homeostasis, the study establishes that therapeutic vitamin D and calcium supplementation in addition to anti-thyroid medication would be ideal for bone health. Recent research is focused on the diagnostic development and also modes of treating the deficiency. The prevalence among the south Indian population has not been studied in all areas and it has been found that a high proportion of participants have low B12 intake, especially among those from rural and semi-urban areas [7, 8]. Among the patients with no secondary conditions, the effect of supplementation was seen to improve the levels of vitamin B12 and D. The supplementation consisted of either tablet, intramuscular or intravenous injections. Almost 75% of the patients mentioned an improvement stating alleviation in their deficiency symptoms after completion on the prescribed course. Similar results were obtained in various other studies [9]. This proves the efficiency of supplementation in restoring the normal levels of vitamin in the body.
Our aim was to observe if any effect was seen with supplementation in patients with secondary conditions such as diabetes, cardiovascular disease, hypertension, rheumatoid arthritis and osteoporosis. The parameters considered for these patients were improvement in general health and relief from their symptoms. Varied results were obtained in patients with other conditions where few patients stated improvement in their disease symptoms. The patient with osteoporosis showed consistent improvement with supplementation, which concurs with vitamin D deficiency treatment. A study on the vitamin D status of immigrant populations in Europe was poor compared to the indigenous European populations. The positive effect of supplementation has been demonstrated to improve cardiovascular health in such people [5]. However in our study most patients with cardiovascular disease also had diabetes and hypertension, and not show much improvement with supplementation. Only one patient with vitamin D supplementation was seen with a general health improvement. The number of patients with hypertension was the highest among the patients with secondary conditions. The improvement seen was less than 20%. In the case of patient with arthritis, improvement was only seen with respect to reduction in pain but not the disease itself. Patients with either diabetes or cardiovascular disease with along with hypertension only reported improvement in physical symptoms related to hypertension but not the others. This improvement was seen in less than 50% of the population and the rest did not show any. Patients with all the three did not show any improvement.
Conclusion
The study concurs with multiple studies that show deficiency among the patients is much higher with respect to vitamin D than B12 and vitamin supplementation helps improve the symptoms. Although supplementation helps alleviate deficiency symptoms in most patients, significant impact cannot be seen on general health in patients with other disorders such as diabetes, cardiovascular disease and hypertension. Pain improvement was observed in rheumatoid arthritis and significant improvement was observed in osteoporosis patients.
Acknowledgements
Krishna Institute of Medical Sciences (KIMS), Secunderabad, Telangana, India.
Conflict of interest
Authors declare no conflict of interest.
Annex 1
Questionnaire
1. Were you informed that you’re Vitamin D and B12 levels are low?
2. Were you prescribed any medication or vitamin package for your deficiency?
3. Did you finish the course of medication/vitamin package prescribed to you?
4. Did you take any own initiative, such as food supplements, herbal medicines or better diet?
5. Is there any improvement in your health with regards to deficiency related symptoms after finishing the vitamin package/medication?
6. Are you suffering from any of the following conditions?
Hypertension/ Diabetes/ Osteoporosis/ Rheumatoid Arthritis/ Cardiovascular Disease
7. Is there any improvement in your condition/disease after supplementation?
8. Have you monitored vitamin levels after completion of prescription or vitamin supplements?
9. Do you ensure good sun exposure/ intake of nutrient rich foods?
10. Have you been cured of any problems?
11. Have you developed any new problems?
12. Would you be interested to come to KFRC/ KIMS for re-test?
References
1. Robert OH, Brown DL. Vitamin B12 deficiency. Am Fam Physician. 2003; 67(5):979 –986.
2. Wacker M, Holiack MF. Vitamin D - effects on skeletal and extraskeletal health and the need for supplementation. Nutrients. 2013; 5(1):111–148.
3. Gordon CM, Feldman HA, Sinclair L, Williams AL, Kleinman PK, et al. Prevalence of Vitamin D deficiency among healthy infants and toddlers. Arch Pediatr Adolesc Med. 2008; 162(6):505–512.
4. Van Der Meer IM, Middelkoop BJC, Boeke AJ, Lips P. Prevalence of vitamin D deficiency among Turkish, Moroccan, Indian and sub-Sahara African populations in Europe and their countries of origin: an overview. Osteoporos Int. 2011; 22(4):1009–1021.
5. Woo KS, Kwok TC, Celermajer DS. Vegan diet, subnormal vitamin B12 status and cardiovascular health. Nutrients. 2014; 6(8):3259–3273.
6. Hanmayyagari B, Guntaka M, Sahay R, Jayanthy R, Sri N. Study of bone markers in hyperthyroidism: Single centre experience from south India. J Med Sci Res. 2015; 3(2):1–4.
7. Shobha V, Tarey SD, Singh RG, Shetty P, Unni US, et al. Vitamin B₁₂ deficiency & levels of metabolites in an apparently normal urban south Indian elderly population. Indian J Med Res. 2011; 134:432–439.
8. Patel J DS. A Questionnaire based survey to evaluate practice and attitude of vitamin-D supplement by private practitioners in western region of Indian population. 2015; 5(1):110–114.
9. Butler CC, Vidal-Alaball J, Cannings-John R, McCaddon A, Hood K, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency: a systematic review of randomized controlled trials. Fam Pract. 2006; 23(3):279–285.
10. Hvas AM, Nexo E. Diagnosis and treatment of vitamin B12 deficiency--an update. Haematologica. 2006; 91(11):1506–1512.
11. Yajnik CS, Deshpande SS, Lubree HG, Naik SS, Bhat DS, et al. Vitamin B12 deficiency and hyperhomocysteinemia in rural and urban Indians. J Assoc Physicians India. 2006; 54:775–782.
12. Herrmann W, Obeid R. Causes and Early Diagnosis of vitamin B12 deficiency. Dtsch Arztebl Int. 2008; 105(40):680–685.
13. Ryan-Harshman M, Aldoori W. Vitamin B12 and health. Can Fam Physician. 2008; 54(4):536–541.
14. Evatt ML, Terry PD, Ziegler TR, Oakley GP. Association between vitamin B12-containing supplement consumption and prevalence of biochemically defined B12 deficiency in adults in NHANES III (third national health and nutrition examination survey). Public Health Nutr. 2010; 13(1):25–31.
15. O’Leary F, Samman S. Vitamin B12 in health and disease. Nutrients. 2010; 2(3):299–316.
16. Hovsepian S, Amini M, Aminorroaya A, Amini P, Iraj B. Prevalence of Vitamin D deficiency among adult population of Isfahan city, Iran. J Health Popul Nutr. 2011; 29(2):149–155.
17. Miljkovic I, Bodnar LM, Cauley JA, Bunker CH, Patrick AL, et al. Low prevalence of vitamin D deficiency in elderly Afro-Caribbean men. Ethn Dis. 2011; 21(1):79–84.
18. Mitchell DM, Henao MP, Finkelstein JS, Burnett-Bowie SA. Prevalence and predictors of vitamin D deficiency in healthy adults. Endocr Pract. 2012; 18(6):914–923.
19. Zhu Z, Zhan J, Shao J, Chen W, Chen L, et al. High prevalence of vitamin D deficiency among children aged 1 month to 16 years in Hangzhou, China. BMC Public Health. 2012; 12:126.
20. Shiva Raju K. Vitamin D is not just vitamin, let us see how ? J Med Sci Res. 2013:5–9.
21. Oberlin BS, Tangney CC, Gustashaw KA, Rasmussen HE. Vitamin B12 deficiency in relation to functional disabilities. Nutrients. 2013; 5(11):4462–4475.
22. Song HR, Kweon SS, Choi JS, Rhee JA, Lee YH, et al. High prevalence of vitamin D deficiency in adults aged 50 years and older in Gwangju, Korea: the Dong-gu study. J Korean Med Sci. 2014; 29(1):149–152.
23. Vierucci F, Del Pistoia M, Fanos M, Erba P, Saggese G. Prevalence of hypovitaminosis D and predictors of vitamin D status in Italian healthy adolescents. Ital J Pediatr. 2014; 40:54.