Full Text
Introduction
Vocal cord paralysis is not a disease per se but is a sign of an underlying disease process that may be central (10%) or peripheral (90%) in origin [1-3]. Due to the long anatomical course of the vagus and recurrent laryngeal nerves, many disease processes can cause vocal cord paralysis [4]. Surgery, malignancy, trauma, infection, and inflammation can all result in vocal cord paralysis. Vocal cord paralysis is most frequently unilateral but can be bilateral [5-8].
Left laryngeal nerve is more vulnerable than the right because the longer course of the nerve creates additional vulnerability, especially within the mediastinum. Paralysis of the left vocal cord is reported 1.4-2.5 times more than right [9]. The main presenting symptom in unilateral vocal cord paralysis is hoarseness of voice, the degree of which depends on the position of paralyzed vocal cord [10, 11]. The other associated symptoms include weak voice, cough, aspiration, and swallowing difficulty. However, about 30–40 % of patients with unilateral vocal cord paralysis are asymptomatic.
All patients with vocal cord palsy need to be evaluated thoroughly with a detailed history, and complete examination of the head and neck, nervous system, and larynx with appropriate radiological investigations to find out the site of the lesion whether in the brain stem, neck, chest, and mediastinum. Direct laryngoscopy of the glottis is the most sensitive and specific method of evaluating the appearance and movement of vocal cords. Unilateral vocal cord palsy is a relatively common finding in Otorhinolaryngology clinics. It may be asymptomatic or may present with a change in voice or even dysphagia and aspiration. Most cases do not present to the clinic due to spontaneous recovery or compensation by the opposite cord. Due to reasons more than one, the exact incidence of the etiology behind unilateral vocal cord palsy has remained a mystery difficult to unfold.
The present study was undertaken to determine the clinical presentation and etiopathology of unilateral vocal cord paralysis.
Materials and methods
The present study was a longitudinal interventional prospective study undertaken in the Department of Otorhinolaryngology at KIMS Hospital, Secunderabad from June 2018 to May 2020 after the approval of the Ethical Committee among 50 adult patients with a confirmed diagnosis of unilateral vocal cord palsy. Patients with the fixity of the vocal cord, laryngeal malignancies, bilateral vocal cord palsy/paresis, patients less than 18 years of age, and patients who lost follow-up were excluded from the study.
All 50 patients were evaluated thoroughly- after a detailed history and complete ear, nose, & throat (ENT), head, neck and systemic examination underwent relevant endoscopic, radiological, hematological, microbiological, and pathological examination to make an etiological diagnosis of vocal cord palsy. For patients with no cause found, a CT/ MRI imaging was done before labelling them as idiopathic. The study was analyzed to determine the etiological factors causing vocal cord paralysis, age distribution, sex incidence, presenting symptoms, and side of paralysis/paresis in the tertiary hospital’s otolaryngology department.
Results
15,955 patients attended the ENT outpatient department of Krishna Institute of Medical Sciences, Secunderabad from June 2018 to May 2020. Of these, 62 patients were diagnosed with unilateral vocal cord palsy. Out of 62, we lost to the follow-up of 12 patients. Thus, the incidence (number of new cases/year) of such patients was found to be 0.35% or 35 per ten thousand new patients. The youngest patient was 21 years while the eldest was 81 years old. Patients were observed in the age range of 21 years to 81 years. Most of the patients (34%) presented in the 4th and 5th decades of life. Male and female patients were 28(56%) and 22(44%) respectively.
28 patients had left-side vocal cord palsy and 22 patients had right-side vocal cord palsy. 40 (80.0%) patients presented with hoarseness of voice (HOV) alone, 3(6%) patients presented with weakness of voice, 5(10.0%) patients presented with difficulty in swallowing, and 2(4.0%) patients presented with cough with aspiration (Figure 1).
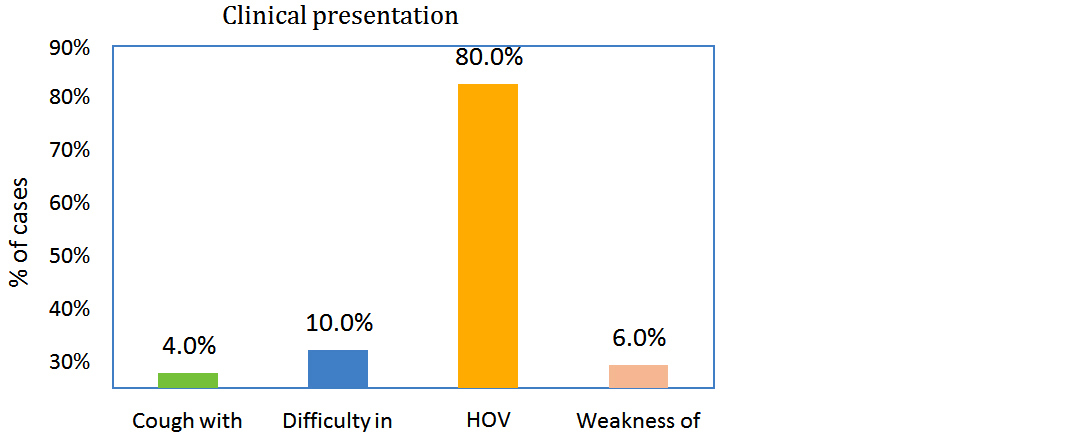
Figure 1: Bar diagram showing distribution based on major presenting symptoms.
In 17 patients (34%) no apparent cause for unilateral vocal cord paralysis was found and thus grouped under the “idiopathic” heading. Other etiological factors are post-surgical trauma, neoplastic, central cause, cardiac, granulomatous disorders, and neurological and post-intubation trauma respectively (Table 1).
Table 1: Shows the percentage of distribution of study subjects based on etiological factors.
|
Etiology of unilateral vocal cord palsy
|
No. of cases
|
Percentage (%)
|
|
Cardiac
|
2
|
4.0
|
|
Central
|
7
|
14.0
|
|
Granulomatous disease
|
1
|
2.0
|
|
Idiopathic
|
17
|
34.0
|
|
Neoplastic
|
10
|
20.0
|
|
Neurological
|
1
|
2.0
|
|
Post intubation
|
1
|
2.0
|
|
Post-surgical trauma
|
11
|
22.0
|
|
Total
|
50
|
100
|
Etiology of unilateral vocal cord palsy No. of cases Percentage (%) Cardiac 2 4.0 Central 7 14.0 Granulomatous disease 1 2.0 Idiopathic 17 34.0 Neoplastic 10 20.0 Neurological 1 2.0 Post intubation 1 2.0 Post-surgical trauma 11 22.0 Total 50 100 Out of 10(22.0%) post-surgical group, 2(18.18%) were post-double valve replacement (DVR) surgery, 1 case (9.09%) was mediastinal tumor excision, 4 (36.36%) was post total thyroidectomy, 1(9.09%) was post carotid tumor excision, 1 (9.09%) was petro-clival meningioma excision and 1(9.09%) was lung biopsy (Table 2).
Table 2: Shows the distribution of the study population among the post-surgical group.
|
Post-surgical group
|
No. of cases
|
Percentage (%)
|
|
Post total thyroidectomy
|
4
|
36.36
|
|
Post-double valve replacement surgery
|
2
|
18.18
|
|
Carotid endarterectomy
|
1
|
9.09
|
|
Lung biopsy
|
1
|
9.09
|
|
Mediastinal tumor excision
|
1
|
9.09
|
|
Petro-clival meningioma
|
1
|
9.09
|
|
post paraganglioma excision
|
1
|
9.09
|
|
Total
|
11
|
--
|
Out of 10(20.0%) neoplastic group, papillary carcinoma cases were 4(40.0%), 2(20.0%) were lymphoma, 1(10.0%) was oat cell carcinoma, 1(10.0%) was carcinoma breast metastasis, 1(10.0%) was carcinoma lung and 1(10.0%) carcinoma oesophagus (Table 3).
Table 3: Shows the distribution of the study population among the neoplastic group.
|
Neoplastic group
|
No. of Cases
|
Percentage
|
|
Carcinoma breast
|
1
|
10.00
|
|
Carcinoma lung
|
1
|
10.00
|
|
Carcinoma oesophagus
|
1
|
10.00
|
|
Lymphoma
|
2
|
20.00
|
|
Oat cell carcinoma
|
1
|
10.00
|
|
papillary carcinoma of the thyroid
|
4
|
40.00
|
|
Total
|
10
|
--
|
Out of 7(14.0%) central group, cerebrovascular accident (CVA) cases were 3(42.86%%), 2(28.57%) were road traffic accident (RTA) cases,1(14.29%) were transient ischemic attack (TIA) and 1 (14.29%) was Jugular Foramen syndrome (Table 4).
Table 4: Shows the distribution of the study population among the central group.
|
Central group
|
No. of cases
|
Percentage (%)
|
|
CVA
|
3
|
42.86
|
|
RTA
|
2
|
28.57
|
|
Jugular foramen syndrome
|
1
|
14.29
|
|
TIA
|
1
|
14.29
|
|
Total
|
7
|
|
The remaining 2(4%) patients had Ortner’s syndrome (cardiac cause), 1(2%) patient had mediastinal lymphadenopathy (Granulomatous disease), 1(2%) patient had post intubation unilateral vocal cord palsy, 1(2%) patient had Parkinson’s disease with unilateral vocal cord palsy.
Discussion
The most common cause is usually the involvement of the vagus or its recurrent laryngeal branch somewhere between the jugular foramen and its entrance into the larynx posterior to the cricothyroid joint [12, 13]. The reported annual incidence of vocal cord paralysis varies from 17%26 to 29.3% [13] as compared to the present study where it is 0.35% which is lower. Most of the patients were in the 4th and 5th decades of life. The mean age is 50 years. Merati [14], Havas [15], and Glazer [16] reported the mean age as 53 years. Ahmed et al. [17] have reported the maximum number of patients in the 5th and 6th decades. Gandhi et al. [18] reported that unilateral vocal cord palsy peaked in the 4th and 5th decades. Regarding male to female ratio (1.27: 1), this finding is consistent with the finding of Alassiry and Hassan [19] in which male to female ratio was 1.2:1.35. Gandhi et al [18] in which male to female ratio was 1.82: 1. Myssiorek [4] has similar findings. On the contrary, Rosenthal et al. [20] reported that the female-to-male ratio was (1.43:1) for those who were diagnosed with vocal fold paralysis. The reason of male to female ratio discrepancy in literature is still not clear, it may be related to the type of centers and scope of the patients.
In the present study left vocal cord (56.0%) was more frequently involved than the right (44.0%), the ratio is 1.27: l. This is attributed to the longer and more tortuous course of the recurrent laryngeal nerve on that side [12]. Ko et al. study reported nearly 68% paralysis on the left side [21] and Srirompotong et al. study reported 73% paralysis on the left side [22]. In the study done at Gartnavel General Hospital-Scotland to identify the etiology of unilateral vocal fold paralysis between 1997 to 2001, out of 77 patients 83% had vocal fold paralysis on the left side and only 17% had right vocal fold paralysis [23].
In the present study, most of the patients with unilateral vocal cord palsy presented with the complaint of hoarseness of voice at 80.0 %. An Indian study by Gupta et al [24] showed hoarseness of voice in 98.21 % of cases. In the present study, symptoms include hoarseness of voice (most common), weakness of voice, difficulty in swallowing, and cough and aspiration. In another study order of symptoms include hoarseness of voice (most common), respiratory problems like difficulty in breathing, cough, aspiration, dysphagia, and dysphonia [25]. The universal presenting symptom, hoarseness of voice, was due to vocal cord paralysis while other symptoms were related to the underlying disease process. Similar observations were made by Swift and Jorger [26].
The etiological factors for vocal cord paralysis could be grouped as idiopathic, neoplastic, neurological, central, cardiac, postsurgical trauma, post-intubation, and inflammatory. In the present study, the commonest group was idiopathic (34.0%) which is consistent with those of Cunning [12] (31%). Though the incidence of idiopathic vocal cord palsies has reduced with improving imaging and fiberoptic endoscopy, it remains the most 38 common etiologies in the present series. A study conducted in Government Medical College Srinagar from November 1998 to January 2000 showed the commonest group was idiopathic (38.18%) [27].
In the present series, postsurgical trauma is the commonest identifiable cause of vocal cord paralysis in 17 cases (22%), in that, post thyroid surgical trauma 4 cases; 2 cases of post-double valve replacement surgery, 1 case each of carotid endarterectomy (Figure 2), lung biopsy, mediastinal tumor excision, petroclival meningioma, and carotid tumor excision Studies state that the most popular causes of vocal cord palsy following surgery are thyroid, esophagus and heart surgeries [28, 29]. In our study also it is thyroidectomy followed by cardiac surgery. The incidence of post-thyroidectomy vocal cord paralysis has been reported in the range of 3.5–6.6%, in the present study it is 8%. In the study by Nerurkar et al [30], surgical trauma was the main cause of paralysis in 38(44.27 %) cases out of these 11 (28.95 %) cases were post thyroidectomy.
In the present study, neoplastic lesions accounted for 10(20%) cases, among which 4 cases are papillary carcinoma of the thyroid (Figure 3), lymphoma neck 2 cases, one case of carcinoma breast metastasis, carcinoma lung, carcinoma esophagus, oat cell carcinoma. A study conducted in the Department of ENT, Himalayan Institute of Medical Sciences, Dehradun, India showed the most common cause of unilateral vocal cord palsy is neoplastic (34.82%) [24]. In neoplastic cases, vocal cord paralysis can occur either by direct involvement of recurrent laryngeal nerve by the malignant disease or by the involvement of the nerve by secondaries to the lymph nodes of mediastinum and neck In the present series following neoplastic, next common cause is central (7 cases), in that 3 cases of cerebrovascular accident, 2 cases of road traffic accident and one of a case of Jugular foramen syndrome and transient ischemic attack.
Other causes were 2 cases of Ortner’s syndrome (cardiac cause), 1 case of Parkinson’s disease (neurological), 1 case of granulomatous disorder with mediastinal lymphadenopathy, and 1 case of post-intubation vocal cord palsy.
Studies state incidence of intubation-related vocal cord palsy is 0.2% [31]. In the present study, it is 2 %. Risk factors in these cases include the size of the endotracheal tube, cuff pressure, duration of intubation, hypotension during surgery, neck in prolonged hyperextension position, the patient being a smoker, and associated comorbidities like diabetes and hypertension [32]. There is a three-fold rise in vocal cord palsy in patients being intubated after the age of 50 years, a two-fold rise in patients with hypertension and diabetes, and a 15-fold rise if the ventilator support is for more than 6 hours [33]. Over-extension of the neck during intubation can cause stretching of both vagus nerves. The endotracheal tube's cuff compresses the anterior branch of the recurrent laryngeal nerve between the endotracheal tube and thyroid cartilage, causing degeneration and paralysis by compromising microcirculation and causing ischemic degeneration of the recurrent laryngeal nerve. Lack of intermittent deflation of the cuff can cause pressure neurapraxia leading to vocal cord palsy [34].
Parkinson's disease (PD) is a progressive neurodegenerative disorder that results from a decline in the release of dopamine within the striatal tracts of the basal ganglia. This leading cause of disability affects approximately one million Americans; PD symptoms include bradykinesia, muscle rigidity, tremor, and postural instability. Most patients with PD also have voice problems characterized by vocal tremors, decreased volume, and hoarseness. This study includes 1 case of Parkinson’s disease associated with right-side vocal cord palsy.

Figure 2: (a) Diagnostic laryngoscopy picture showing right vocal cord palsy, (b) picture showing post endarterectomy scar.
Figure 3: (a) Video laryngoscopic picture of papillary carcinoma of thyroid, (b, c) CT scan images show enlargement of the left lobe of the thyroid and enlarged hilar lymph nodes.
Limitations
The present study is based on limited sample size and therefore it is inadequate to provide conclusive data. The tertiary center does not precisely reflect the disease profile of the community.
Conclusion
Vocal cord palsy has got capricious etiologies. Idiopathic causes predominated even now in the present-day scenario. A case of unilateral vocal cord palsy should be labeled idiopathic only after the exclusion of all possible causative factors by thorough clinical, endoscopic, and radiological evaluation. Our study showed that thorough evaluation and investigation of cases with unilateral vocal cord palsy unveils interesting and sometimes rare and probably life-threatening underlying pathologies, which could be treated or managed appropriately.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Harvey MT. Vocal cord paralysis-etiology and management. Laryngoscope. 1980; 90(4):585–590.
[2] Hagen PJ. Vocal cord paralysis. Ann Otol Rhino Laryngol. 1963; 72:206–222.
[3] Goff FW. Vocal cord paralysis. JAMA. 1970; 212(8):1378–1379.
[4] Myssiorek D. Recurrent laryngeal nerve paralysis: anatomy and etiology. Otolaryngol Clin N Am. 2004; 37(1):25–44.
[5] Chen HC, Jen YM, Wang CH, Lee JC, Lin YS. Etiology of vocal cord paralysis. ORL J Otorhinolaryngol Relat Spec. 2007; 69(3):167–171.
[6] Terris DJ, Arnstein DP, Nguyen HH. Contemporary evaluation of unilateral vocal cord paralysis. Otolaryngol Head Neck Surg. 1992; 107:84–90.
[7] Glazer HS, Aronberg DJ, Lee JK, Sagel SS. Extralaryngeal causes of vocal cord paralysis: CT evaluation Otolaryngol Head Neck Surg. 1992; 107:84–90.
[8] Tasar A, Yanturali S, Topacoglu H, Ersoy G, Unverir P, et al. Clinical efficacy of dexamethasone for acute exudative pharyngitis. Clin J Emerg Med. 2008; 35:363–367.
[9] Sagawa M, Donjo T, Isobe T, Notake S, Nakai M, et al. Bilateral vocal cord paralysis after lung cancer surgery with a double-lumen endotracheal tube: a life threatening complication. J Cardiothorac Vasc Anesth. 2006; 20:225–226.
[10] Tucker HM. Vocal cord paralysis etiology and management. Laryngoscope. 1980; 90(4):585–590.
[11] Titche LL. Causes of recurrent laryngeal nerve paralysis. Arch Otolaryngol. 1976; 102(5):259–261.
[12] Cunning DS. Unilateral vocal cord paralysis. Annals of Otorhinolaryngol. 1955; 64(2):487–494.
[13] Clerf LH. Unilateral vocal cord paralysis. JAMA. 1953; 151:900–903.
[14] Merati AL, Shermirani N, Smith TL, Toohill RJ. Changing trends in the nature of vocal fold impairment. Am J Otolaryngol Head Neck Med Surg. 2006; 27(2):106–108.
[15] Havas T, Lowinger D, Priestly J. Unilateral vocal fold paralysis: causes, options, and outcomes. Aust NZ J Surg.1999; 69(7):509–513.
[16] Glazer HS. Extralaryngeal causes of vocal cord paralysis: CT evaluation. Am J Radiol. 1983; 141(3):527–531.
[17] Ahmad S, Ajaz M, lateef M. A study of incidence and etiopathology of vocal cord paralysis. Indian J Otolaryngol Head Neck Surg.2002; 54(4):294–296.
[18] Gandhi S, Rai S, Bhowmick N. Etiological profile of unilateral vocal fold paralysis: A single institutional experience over 10 years. JLV. 2015; 4(2):58–62.
[19] Alassiry H, Hassan N. Etiological factors and management of vocal fold paralysis: single institution study. Int J Otorhinolaryng. 2018; 4(1):16–20.
[20] Rosenthal LH, Benninger MS, Deeb RH. Vocal cord immobility: A longitudinal analysis of etiology over 20 years. Laryngoscope. 2007; 117(10):1864–1870.
[21] Ko HC, Lee LA, Li HY, Fang TJ. Etiologic features in patients with unilateral vocal cord paralysis in Taiwan. Chang Gung Med J. 2009; 32(3):290–296.
[22] Srirompotong S, Sae-Seow P, Srirompotong S. the cause and evaluation of unilateral vocal cord paralysis. J Med Assoc Thai. 2001; 84(6):855–858.
[23] Loughran S, Alves C, MacGregor FB. Current aetiology of unilateral vocal fold paralysis in a teaching hospital in the West of Scotland. JLO. 2002; 116(11):907–910.
[24] Gupta J, Varshney S, Bist SS, Bhagat S. Clinico-etiolological study of vocal cord paralysis. Indian J Otolaryngol Head Neck Surg. 2013; 65(1):16–19.
[25] Benninger MS, Gillen JB, Altman JS. Changing etiology of vocal cord immobility. Laryngoscope. 1998; 108(9):1346–1350.
[26] Swift AC, Jorger A. Vocal cord paralysis. J Laryngol Otol. 1987; 101(2):169–171.
[27] Ahmad S, Muzamil ZA, Lateef M. A study of incidence and etiopathology of vocal cord paralysis. Indian J Otolaryngol Head Neck Surg. 2002; 54(4):294–296.
[28] Toutounchi SJS, Eydi M, Golzari SEJ, Ghaffari MR, Parvizian N. Vocal cord paralysis and its etiologies: a prospective study. J Cardiovasc Thorac Res. 2014; 6(1):47–50.
[29] Hazem MZ, Naif AA, Ahmed AS. Recurrent laryngeal nerve injury in thyroid surgery. Oman Med J. 2011; 26(1):34–38.
[30] Nerukar N, Tandon S, Kiran K, Joshi A, Gharat P, et al. Unilateral vocal fold paralysis: an Indian scenario. Bombay Hosp J. 2006; 48(4):561–567.
[31] Vyshnavi S, Kotekar N. Aphonia following tracheal intubation: an unanticipated post-operative complication. Indian J Anaesth. 2013; 57(3):306–308.
[32] Nama RK, Bhosale GP, Butala BP, Sharma AR. Bilateral adductor vocal cord palsy: complication of prolonged intraoperative hypotension after endotracheal intubation. Middle East J Anaesthesiol.2015; 23(3):339–342.
[33] Kikura M, Suzuki K, Itagaki T, Takada T, Sato S. Age and comorbidity as risk factors for vocal cord paralysis associated with tracheal intubation. Br J Anaesth. 2007; 98(4):524–530.
[34] Gune A, Kale P, Patankar R, Mathur SK. Bilateraladductor vocal cord palsy: Complication of prolonged endotracheal intubation. Int J Health Sci Res. 2016; 6(8):395–397.