Full Text
Introduction
Benign lesions of the larynx are non-neoplastic tumors of the larynx usually caused by infection, trauma, allergy, acid reflux, degeneration, vocal abuse, or frequent cough [1, 2]. They are broadly classified into non-neoplastic, neoplastic, and saccular swellings. Benign neoplastic is less common than malignant tumors. The common lesions of the vocal cord are screamer’s nodules, vocal polyp, papilloma, Reinke’s edema, vocal cysts, or intra-chordal cysts. Rare disorders include pleomorphic adenoma, oncocytoma, rhabdomyoma, neurofibroma, neurilemmoma, lipoma, and fibroma. The importance of benign lesions of the larynx is in the quality of speech and phonation. As phonation results from a cyclic interaction of air exhaled and vocal cord oscillations in the glottis cycle. Voice disorders cause communication disabilities leading to psychosocial disturbances and impaired quality of life [3, 4].
The most common presentation in vocal fold disease is hoarseness seen in almost 100% of cases [5, 6]. Various other symptoms include cough, painful swallowing, difficulty in swallowing, fever, lump in the throat, and respiratory distress. Vocal nodules which are the most common benign lesions are found at the junction of the anterior 1/3rd and posterior 2/3rd of the true vocal cords. This is because the mechanical force of vibration is more intense at this junction.
Video-laryngeal stroboscopy (VLS) is considered the most efficient diagnostic tool for diagnosing vocal cord disorders [7, 8]. Treatment of benign lesions of the vocal cord includes medical management, speech therapy, and surgical therapy [9]. Micro laryngeal surgery (MLS) is considered the best treatment modality for the restoration of speech quality and diagnosis of disease and further management. It preserves the adequate vibratory characteristics of the multiple-layered microvascular structure of the vocal cord [10].
Materials and methods
A total number of 30 patients with clinical evidence of a benign vocal cord lesion, above the age of 15 years who presented to the department of ENT of SVIMS-SPMC, a tertiary care referral center in Andhra Pradesh were enrolled in this study from January 2017 to June 2022. The study was approved by the institutional ethical committee.
All patients above 15 years of age with benign lesions of vocal folds who have not responded to medical management were included in the study, whereas patients with age less than 15 years, fluency and articulation disorders, malignant lesions of the larynx and patients who refused surgery were excluded from the study.
A total of 30 patients were diagnosed on the basis of history and clinical examination (VLS) as cases of benign disease of the larynx and were posted for surgery after pre anesthesia check-ups. All patients underwent micro laryngeal surgery under general anesthesia. Patients were followed up every month to rule out any recurrence of symptoms and a repeat video laryngoscopy was performed on the follow-up visit for the next six months.
Results
In the study, the maximum incidence of benign lesions was found in the age group of 20-60 years. There were 25 males and 5 females in the present study with a male: female ratio of 1:5. The overall sex distribution showed a male preponderance over the female group in cases of nodules.
The total number of patients having benign mucosal lesions of the vocal folds included in this study was 30. Out of 30, 12 patients had vocal nodules, 10 had polyps, 3 presented with a hemorrhagic polyp, one patient had Reinke’s edema, two patients had haemangioma (Figure 1), one patient had juvenile papilloma and one patient had condyloma acuminata (Figures 2 and 3).
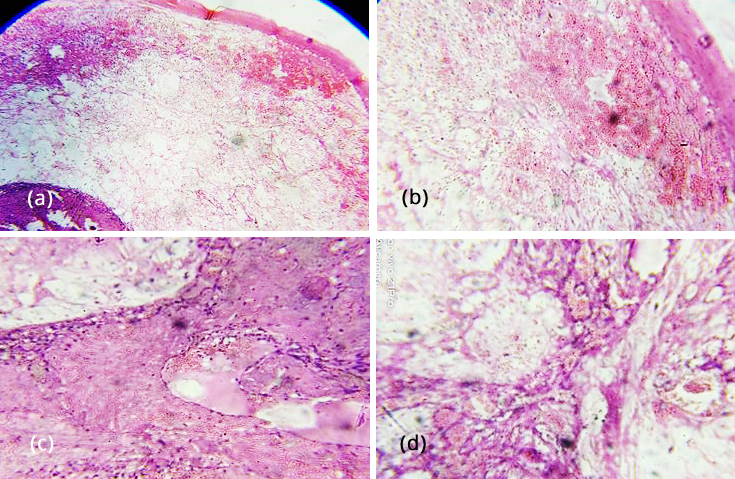
Figure 1: Haemangioma: (a) H&E 4X showing lining stratified squamous epithelium, sub epithelium showing variable sized blood vessels filled with RBCs, (b) H&E 10X lining stratified squamous epithelium sub epithelium showing variable sized blood vessels, (c&d) H&E 20X deeper portion of the subepithelial stroma shows variable sized communicating blood vessels with variably thickened walls, the lumen shows RBCs and fibrin.
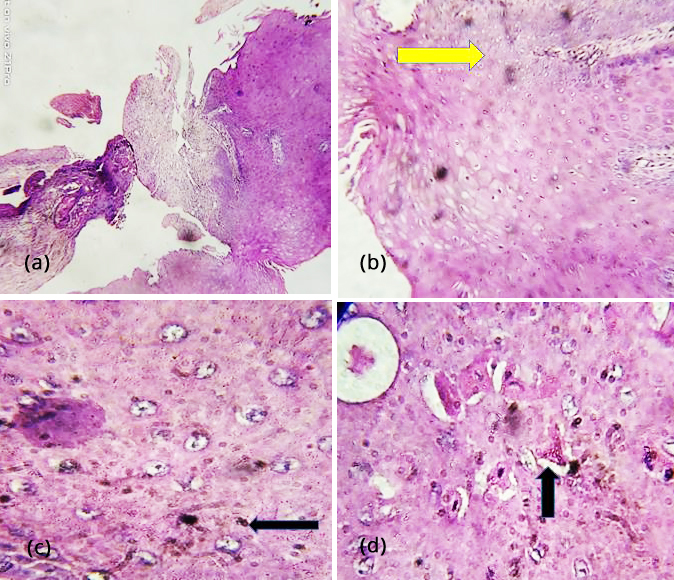
Figure 2: Condyloma acuminata – (a) H&E 4X showing strips of irregularly hyperplastic squamous epithelium, (b) H&E 10X epithelium showing papillomatosis(arrow), (c&d) acanthosis. H&E10X squamous epithelial cells showing koilocytotic atypia involving the superficial layers of the epithelium, few of the superficial squamous cells showing parakeratosis (arrows).
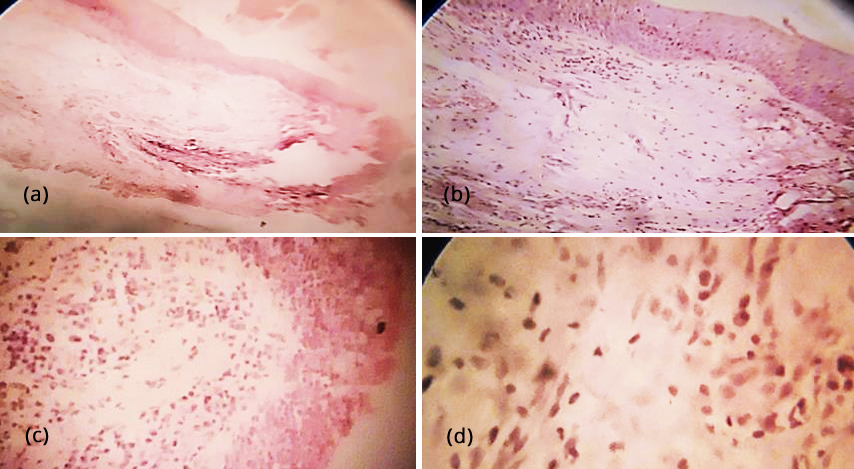
Figure 3: Laryngeal nodule - (a) H&E 4X showing polypoidal mass with lining stratified squamous epithelium, sub epithelium showing fibro collagenous stroma, (b) H&E 10X showing lining stratified squamous epithelium, underlying fibro collagenous stroma, few blood vessels, areas of collagenisation and lymphoid aggregate, (c) H&E 10X one focus showing pseudostratified ciliated columnar epithelium in transition to stratified squamous epithelium, (d) H&E40X stroma is oedematous with proliferating fibroblasts and inflammatory cells.
Hoarseness was one of the most common presenting symptoms and was present invariably in all the cases (100%). Fatigue of voice was the second most common presenting symptom (80%) followed by foreign body sensation (50%), heartburn (2%), and dry cough (1%). In occupation, wise distribution farmers with a history of smoking were the most common group associated with benign vocal fold lesions followed by housewives and teachers with a history of vocal abuse and alcohol consumption. The most common risk factors predisposing to a benign lesion of the larynx are smoking (73.33%) followed by vocal abuse (10%), alcohol intake (10%), gastroesophageal reflux (3.33%), and allergy (3.33%).
All patients underwent MLS surgery and followed up every month to access any recurrence of symptoms or lesions. All of them were subjected to repeat video laryngoscopy (Figures 4, 5 and 6) on each follow-up visit. In our study, only one patient with condyloma acuminata had a recurrence of the disease for which re-surgery was performed and followed accordingly. Postoperative lifestyle modification related to underlying pathology was explained and advised to all the patients.
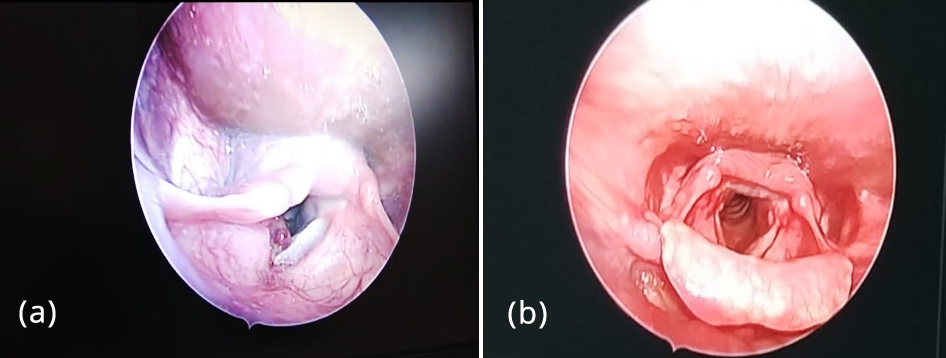
Figure 4a,b: Hemorrhagic vocal polyp – preoperative and postoperative VLS images.
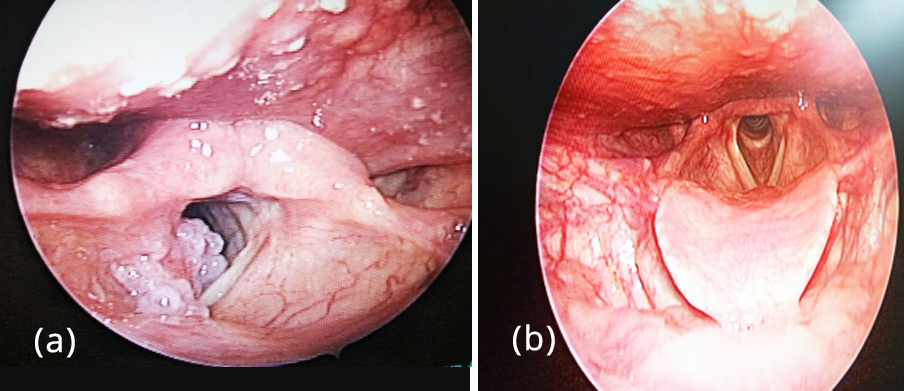
Figure 5a,b: Condyloma accuminata - preoperative and postoperative VLS images.
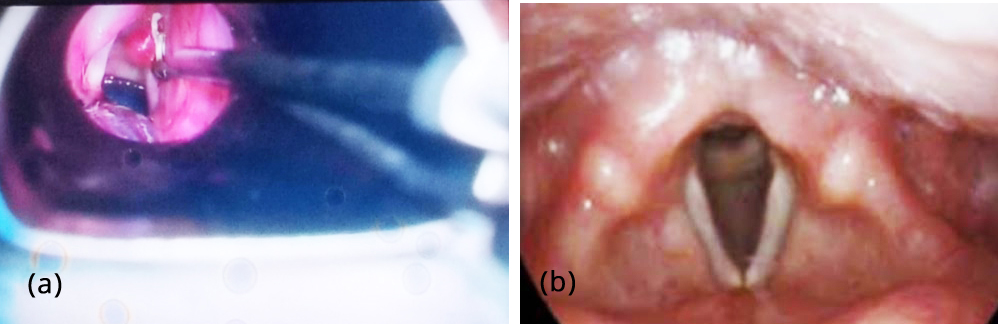
Figure 6a,b: Operative picture of haemorrhagic vocal polyp and postoperative VLS image.
In our study the maximum incidence of benign lesions was found in the age group of 20 - 60 years. Hoarseness was one of the most common presenting symptoms and was present invariably in all the cases (100%). Fatigue of voice was the second most common presenting symptom (80%) followed by foreign body sensation (50%), heart burn (2%) and dry cough (1%) (Table 1).
Table 1: Percentage of predominance of symptoms.
|
Symptoms
|
Percentage
|
|
Hoarseness
|
100%
|
|
Voice fatigue
|
80%
|
|
Foreign body sensation
|
50%
|
|
Heart burn
|
2%
|
|
Dry cough
|
1%
|
In the present study shows farmers with history of smoking were most commonly affected group with benign vocal cord lesions followed by house wife and teachers with history of vocal abuse and alcohol consumption (Tables 2&3).
Table 2: Occupation wise distribution.
|
Occupation
|
Percentage
|
|
Farmer
|
80%
|
|
Teacher
|
3.33%
|
|
House wife
|
16.66%
|
Table 3: Association of risk factors.
|
Risk factor
|
Percentage
|
|
Smoking
|
73.33%
|
|
Vocal abuse
|
10%
|
|
Alcohol
|
10%
|
|
Gastro oesophageal reflux
|
3.33%
|
|
Allergy
|
3.33%
|
Discussion
In our study, out of the 30 patients with vocal fold lesions, the most common lesion was vocal nodules (40%), whereas the second most common was vocal polyps, which is seen in about 33.33% of patients followed by hemorrhagic polyp (10%), fibroepithelial polyp (6.66%), Rinke’s edema (3.33%), haemangioma (3.33%), and condyloma accuminata (3.33%). Our study correlates with Saha et al., who also found the largest subset comprised of vocal nodules, seen in about 60% of patients and the second most common pathology is vocal fold polyp seen in 20% of patients [11]. Siddapur et al also found that vocal nodules are the most common benign vocal fold lesions but with a lower incidence rate of 35% observed in their study [12]. Mahesh et al reported an incidence of 28.57% and 24%, of vocal nodules and vocal polyps respectively [13]. The most common age group affected in our study population is between the age of 20 to 60 years, which is similar to the lower limit of Singhal et al [14]. Their study reported a maximum number of patients in the age group of 20 to 40 years. Our study revealed more male preponderance as compared to females which is supported by Chopra et al [15] and Saha et al [11].
This study results also show hoarseness to be the most common presenting symptom followed by vocal fatigue. This incidence correlates with the results of similar Siddapur et al [4]. Wani et al also found that hoarseness was a predominant symptom in 73% of patients, followed by cough (20%), foreign body sensation (19%), heartburn (17%), frequent throat clearing (13%) and low-grade pain in (9%) of patients [16].
Our study shows smoking and vocal abuse to be the most common predisposing etiological factors which are similar to the conclusion of Baitha et al [17]. Cigarette smoking chronically irritates the mucosa of the larynx and results in lesions. Prolonged exposure predisposes to laryngeal carcinoma. Micro laryngeal surgery remains the best treatment modality for benign vocal fold lesions. Thomas et al reported that micro laryngeal surgery provides reversal to normal vocal fold anatomy and physiology, return of normal mucosal wave and improved amplitude of vibration with complete glottic closure [18]. Micro laryngeal surgery followed by lifestyle modification including vocal hygiene, voice rehabilitation or speech therapy, cessation of smoking, avoidance of alcohol, and spicy food helps in reducing the incidence and recurrence of benign vocal fold lesions significantly as observed in our study similar to Baitha et al [17] and Thomas et al [18] studies.
Limitations
The present study is based on a limited sample size and therefore it is inadequate to provide conclusive data. The tertiary centre does not precisely reflect the disease profile of the community.
Conclusion
The benign vocal fold lesions produce a spectrum of symptoms from hoarseness to stridor. These lesions can affect social functioning and work performance. Micro laryngeal surgery plays a vital role in managing vocal fold lesions. Postoperative lifestyle modification including vocal hygiene, voice rehabilitation or speech therapy, cessation of smoking, and avoidance of alcohol and spicy food helps in reducing the incidence and recurrence of benign vocal fold lesions significantly.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] McGlashen J. Disorders of the voice. In: Hibbert J, editor. Scott-Brown otolaryngology, head and neck surgery 7th Edn. London: Edward Arnold; 2008.pp.2192–2210.
[2] Altman KW. Vocal cord masses. Otolaryngol Clin North Am. 2007; 40(5):1091–1108.
[3] Murry T, Rosen CA. Outcome measurements and quality of life in voice disorders. Otolaryngol Clin North Am. 2000; 33(4):905–916.
[4] Halawa WE, Perez SS, Antonio CG. Measurement of vocal handicap in patients with vocal nodules and functional dysphonias. Egypt J Ear Nose Throat Allied Sci. 2011; 12(2):121–124.
[5] Mehta AS. An etiological study of hoarseness of voice. Thesis, Gujarat University, 1985. [6] Parikh N. Aetiology study of 100 cases of hoarseness of voice. Indian J Otolaryngol Head Neck Surg. 1991; 43(2):71–73.
[7] Mehta DD, Hillman RE. Current role of stroboscopy in laryngeal imaging. Curr Opin Otolaryngol Head Neck Surg. 2012; 20(6):429–436.
[8] Yelken K, Gultekin E, Guven M, Eyibilen A, Aladag I. Impairment of voice quality in paradoxical vocal fold motion dysfunction. J Voice. 2010; 24(6):724–727.
[9] Verdolini K, Rosen C, Branski R. Classification manual for voice disorders. East Sussex: Psychology Press; 2006.
[10] Ford CN. Advances and refinements in phonosurgery. Laryngoscope. 1999; 109(12):1891–1900.
[11] Saha PP. A clinicopathological study of benign lesions of the vocal fold. Journal of Dental and Medical Sciences. 2017; 16(2):9–12.
[12] Siddapur GK, Siddapur KR. Comparative study of benign vocal fold lesions in a tertiary health centre. Int J Otorhinolaryngol Head Neck Surg. 2015; 1(2):65–68.
[13] Mahesh C, Panduranga KM, Kiran B, Ranjith P, Ravi BP. Benign lesions of larynx-a clinical study. Indian J Otolaryngol Head Neck Surg. 2012; 57(1):35–38.
[14] Singhal P, Bhandari A, Chouhan M, Sharma MP, Sharma S. Benign tumors of the larynx: A clinical study of 50 cases. Indian J Otolaryngol Head Neck Surg. 2009; 61(1):26–30.
[15] Chopra H, Kapoor M. Study of benign glottic lesions undergoing microlaryngeal surgery. Indian J Otolaryngol Head Neck Surg. 1997; 49(3):276–279.
[16] Wani AA, Rehman A, Hamid S, Akhter M, Baseena S. Benign mucosal cord lesion as a cause of hoarseness of voice-a clinical study. Otolaryngology. 2012; 2(3):3–4.
[17] Baitha S, Raizada RM, Kennedy AK, Puttewar MP, Chaturvedi VN. Predisposing factors and etiology of hoarseness of voice. Indian J Otolaryngol Head Neck Surg. 2004; 56(3):186–190.
[18] Thomas G, Mathew SS, Chrysolyte SB, Rupa V. Outcome analysis of benign vocal cord lesions by videostroboscopy, acoustic analysis and voice handicap index. Indian J Otolaryngol Head Neck Surg. 2007; 59:336–340.
[19] Shivaram Gautaam N, Gopakumar K, Suresh Kumar M, Ragitha Binu Krishnan. Clinicopathological study of non-malignant lesions of the larynx: a prospective observational study. Int J Otorhinolaryngol Head Neck Surg. 2022; 8(1):57–63.