Original Research
2016
March
Volume : 4
Issue : 1
Myocardial infarction in young population: An increasing trend
Khalid Mohiud-Din, Syed Mazoor Ali, Bashir Naiku, Nazir Lone, Parvez A Zagar
Pdf Page Numbers :- 4-7
Khalid Mohiud-Din1,*, Syed Mazoor Ali1, Bashir Naiku1, Nazir Lone1 and Parvez A Zagar1
1Division of Cardiology, Govt. Medical College, Srinagar, Jammu and Kashmir, India
*Corresponding author: Dr. Khalid Mohiud Din, Consultant Cardiologist, Govt. Medical College, Srinagar, Jammu and Kashmir, India. Email: khalidmm786@gmail.com
Received 23 September 2015; Revised 14 November 2015; Accepted 27 November 2015; Published 10 December 2015
Citation: Mohiud-Din K, Ali SM, Naiku B, Lone N, Zagar PA. Myocardial infarction in young population: An increasing trend. J Med Sci Res. 2016; 4(1):4-7. DOI: http://dx.doi.org/10.17727/JMSR.2016/4-002
Copyright: © 2016 Mohiud-Din K, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To define the correlation of clinical features with the angiographic findings in young patients (≤40 years) who presented to our institute with angina symptoms and also have an idea of disease burden in our community.
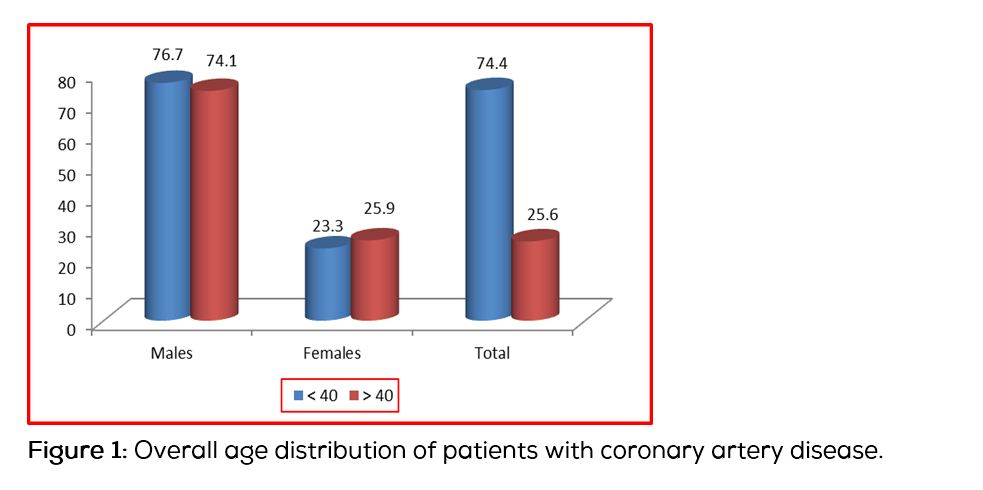
Methods and results: A retrospective study was conducted over a 5 year period from 2010 to 2015. One hundred and twenty nine consecutive patients <40 years of age were admitted for evaluation and were reviewed. The mean age was 37.7 years (range 28-40), 76.7% (99) were males and 23.3% (30) were females. This was similar to the figures for more than 40 years cohort, 74.1% males and 25.9% females. Sixty two percent were urban and 13.2% were non-Kashmiri security forces. Predominant presentation was acute myocardial infarction (47.3%) followed by angina on effort (44.2%), atypical chest pain (7%), and unstable angina (1.6%). Among males 59.5% had angiographically documented coronary artery disease while only 23% of females had coronary artery disease documented. Three females presented with anterior wall myocardial infarction secondary to infective endocarditis, spontaneous left main coronary dissection and takotsubo cardiomyopathy respectively.
Conclusion: The study focuses our attention on rising prevalence of coronary artery disease in young individuals from urban communities. Symptomatic males may need thorough early evaluation, young females presenting with myocardial infarction should be evaluated for non-atherosclerotic etiologies.
Keywords: Myocardial infarction; young population; coronary artery disease
Full Text
Although coronary heart disease (CHD) primarily occurs in patients over the age of 40, younger men and women can be affected. Most studies have used an age cut-off of 40 years to define “young’’ patient with CHD. However in some studies 45 years is taken as an upper limit. We have used 40 years as the upper age limit for young CHD.
Myocardial infarction in young adults can be broadly divided two groups, those with angiographically normal coronary arteries and those with coronary artery disease of varying etiology. There is significant overlap in pathophysiology between these two groups.
Angiographically “normal” coronary arteries: The definition of normality is arbitrary, as we know that angiographically normal looking coronary arteries can have significant atherosclerotic plaque burden when assessed using intracoronary ultrasound. The pathophysiology of myocardial infarction in the presence of “normal’’ coronary arteries remains unclear but can be explained on the basis o f coronary artery thrombosis (5%), embolisation (5%), spasm, or a combination of these processes. Coronary thrombosis can be seen in hypercoagulable states such as in the nephrotic syndrome, antiphospholipid antibody syndrome, protein S and factor XII deficiencies [1-4] coronary embolisation is rare but has been reported with endocarditis usually affecting the aortic valve [5], coronary arteries spam causing myocardial ischemia. All of these factors should be taken into consideration when treating young patients with CHD.
Material and methods
This is a retrospective study of young adults, presenting with various coronary syndromes at our institute over five year period (2010 to 2015). We used an age of 40 years and less to define young ischemic heart disease. Angiographic registries of patients were analyzed and case files and angiographic records of patients <40 years were studied for presenting symptoms, investigations, diagnosis and angiographic findings. Angiograms showing more than 50% of luminal narrowing were labeled to have significant coronary artery disease.
Statistics
Variables were analysed by SPSS 16. Frequencies of all variables were generated and standard deviation of quantitative variables like age was also generated. Categorical variables were given in number (percentages/frequencies).
Results
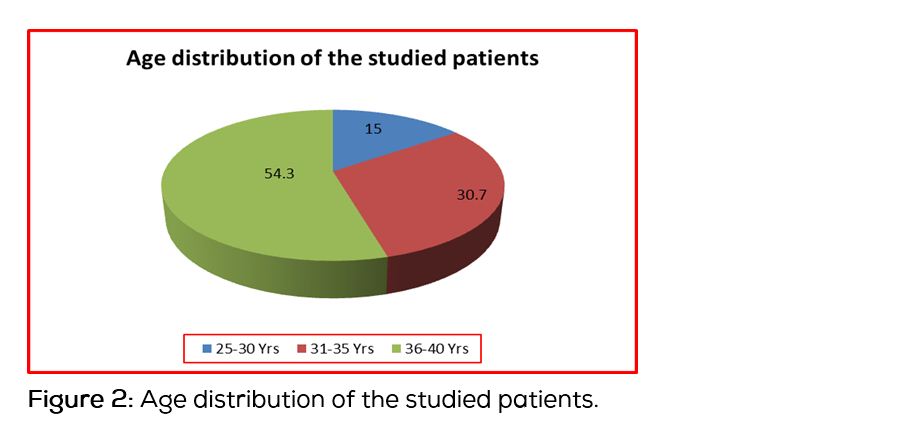
A total of 1326 patients were subjected to coronary angiography over a course of 5 year from 2010 to 2015 (Table 1). Out of them 986 (74.4%) were males and 340 (25.6%) females. One hundred twenty nine patients were less than 40 years of age thus qualifying for young ischemic heart disease. The mean age was 37.7 years (range 28-40), 99 (76.7%) were males and (30) 23.3% females (Figure 1), similar to the figures in higher age group. In the young ischemic heart disease cases youngest patient was 28 years old and majority were clustered at 40 years (54.3%) (Figure 2). Sixty two percent were urban and 38% rural. A significant percentage of patients (13.2%) were non-Kashmiri’ population from security forces. Among males 58 (58.5%) had myocardial infarction, 9 patients (9%) had atypical chest pain and 2 (2%) had unstable angina. Fifty nine (59.5%) males had angiographically documented coronary artery disease. Among 30 females 3 patients had NSTEMI, 2 had angina on effort with angiographically documented Double vessel disease, one had anterior wall myocardial infarction secondary to coronary embolism from infective endocarditis. One patient had spontaneous coronary dissection of left main coronary artery and one patient presented with extensive anterior wall myocardial infarction with normal coronary angiogram and apical left ventricular ballooning, Takotsubo cardiomyopathy. A total of seven (23%) females had coronary involvement. Atherosclerotic involvement was seen in 5 females (16.6%).
Table 1: Patients evaluated for CAD at our institute over 5 years (2010 to 2015).
|
Age (Years)
|
Males
|
Females
|
Total
|
|
< 40
|
99 (76.7%)
|
30 (23.3%)
|
129 (9.7%)
|
|
> 40
|
887 (74.1%)
|
310 (25.9%)
|
1197 (90.3%)
|
|
Total
|
986 (74.4%)
|
340 (25.6%)
|
1326 (100.0%)
|
Discussion
In our population, there were 9.7% of patients younger than 40 years who were subjected to coronary angiography for various coronary syndromes over last five years, consistent with figures of world literature in which myocardial infarction below 40 years. The majority of sufferers are men but an increasing prevalence among women has been observed nowadays, one in four patients with myocardial infarction younger than 45 years are females. Our observations showed coronary atherosclerosis 3.7 times more common in young males.
The main cause of myocardial infarction in young people is atherosclerosis (about 80% of cases) usually one vessel disease [6]. Atherosclerotic process begins at birth and significant lesions in coronary arteries may be present as early as age of 25 or 30 years [7, 8], after the age of 40 the first symptom of exercise induced angina are not uncommon. The reasons for such a rapid progression of atherosclerosis causing Myocardial infarction at the age of 40 years are still being investigated. Beresewiez et al. [9] indicate that the process may even begin in foetus. The authors emphasize that although the dynamics of atherosclerosis are determined by classic risk factors, the susceptibility to atherosclerotic process is programmed by external influences during intrauterine growth, for example mother’s hypercholesterolemia. Recent studies prove environmental influences on genotype may promote the development of coronary artery disease in young age.
Most recent studies have identified smoking as the strongest risk factor in both men and woman under 40 suffering from acute coronary syndrome [10]. Religa [11] found that of 100 women admitted with first myocardial infarction, 45% were smokers while in subset of patients <45 years of age the figure was 95%. In our study none of the young females was a smoker.
Dyslipidemia occurs in about 29% of patients with myocardial infarction below the age of 40. Premature coronary artery disease is most common in patients with familial hypercholesterolemia, less often in familial mixed dyslipidemia. The results of many studies indicate significantly higher levels of triglycerides and total cholesterol and low concentration of HDL cholesterol (especially HDL2) in patients with coronary artery disease under 40, compared with those in whom disease occurred >60 years [12, 13]. The GRIPPS study of over 500 patients confirms that a high level of LDL cholesterol is a significant risk factor of myocardial infarction in men under 45 years. In patients with hypercholesterolemia the highest risk of ischemic heart disease occurs when the triglyceride level is moderately increased but often accompanied by severe increase of highly atherogenic VLDL.
Premature ischemic heart disease in the first degree relatives is recognized as an independent risk factor for this disease under age of 40 [14]. Many proatherogenic genetic factor were discovered. E4 allel of the lipoprotein, E is an important risk factor for atherosclerosis and ischemic heart disease [15].
Arterial hypertension is less common in young patients [16]. Type 2 diabetes mellitus affects only 3-5% of patients after myocardial infarction under the age of 45 [17]. Between 35% and 58% of patients after myocardial infarction under the age of 45 are obese [18]. Obesity doubles the risk of myocardial infarction in men and increases the risk in women by 2.5 times.
In population younger than 40 years, myocardial infarction in patients without coronary artery stenosis is not uncommon. In our study non- atherosclerotic disease was seen in 10% of young females, one patient had spontaneous coronary artery dissection of left main coronary artery, one patient anterior wall myocardial infarction secondary to infective endocarditis on a rheumatic mitral valve and one patient presented with anterior wall myocardial infarction with reversible left ventricular apical ballooning and normal coronary angiogram – Takotsubo cardiomyopathy.
Cocaine and amphetamine use is a factor associated with an increasing number of myocardial infarctions by increasing sympathetic output and increase in coronary artery spasm and triggering coronary artery thrombosis. Spontaneous coronary artery thrombosis occurs secondary to imbalance between coagulation and fibrinolytic processes. Weiss et al. [19] emphasize the importance of many polymorphisms of platelet receptors (glycoprotein 1b and 11b/11 la). Patients with polymorphisms have six times greater risk of coronary thrombosis. Antiphospholipid antibody syndrome is a rare background of myocardial infarction in young women. In rare cases of myocardial infarction in young people a coronary artery anomaly is diagnosed [20, 21].
We had a significant percentage of patients (13.2%) from non-Kashmiri residents from various states of the country employed in security forces in whom coronary artery disease at a young age possibly because of their difficult occupation and stress of living way from their families.
The results of GISSI study [17] indicate that young age is an independent prognostic factor of a favourable clinical course in myocardial. It is estimated that increased risk of recurrent coronary events concerns in only 5% of patients with myocardial infarction under the age of 40.
Conclusion
As with other parts of the world coronary artery disease is increasing in prevalence in the young adult population of the valley (region in north India) predominantly in the urban setup. The disease is more frequent in males. In males around sixty percent had positive correlation for atherosclerotic coronary artery disease and more than one third with myocardial infarction had non-atherosclerotic causes for their infarctions.
Conflicts of interest
Authors declare no conflicts of interest.
References
1. Fujimura O, Gulamhusein S. Acute myodcardial infarction thrombotic complication of nephritic syndrome. Can J Cardiol. 1987; 3(6):267–269.
2. Hamsten A, Norberg R, Björkholm M, de Faire U, Holm G. Antibodies to cardiolopin in young survivcrs of myocardial infarction an association with recurrent cardiovascular events. Lancet. 1986; 1(8473):113–16.
3. Manzer KJ. Padder FA. Conrad AR, Freeman I, Jonas EA. Acute myocardial infarction with normal coronary artery a case report and review of literalure Am J Med sci. 1997; 314(5):342–345.
4. Penny WJ, Colvin BT, Brooks N. Myocardial infarction with normal coronary arteries and factor XII deficiency. Br Heart J. 1985; 53(2):230–234.
5. Agirbasli MA, Hansen DE, Byrd BF. Resolution of vegetations with anticoagulation after myocardial infarction in primary antiphospholipid syndrome. J Am Soc Echocardiolgr. 1997; 10(8):877–880.
6. Choudhry L, Marsh JD. Myocadial infarction in young patients. Am J Med. 1999; 107(3):254–261.
7. McGill HC, McMahan CA, Zieska AW, Tracy RE, Malcom GT, et al. Association of coronary heart disease risk factors with microscopic qualities of coronary atherosclerosis in youth. Circulation. 2000; 102(4):374–379.
8. Tuzcu EM, Kapadia SR, Tuar E, Ziada KM, Hobbs RE, et al. High prevalence of coronary atheroslerosisn in asymptomatic teenagers and young adults: Evidence from intravascular ultrasound. Circulation. 2001; 103(22):2705–2710.
9. Beresewicz A, Skiercynska. Atherosclerosis: Disease of whole live and whole population of eastern civilization countries. Choroby Serca. Naczyn. 2006; 3:1–6.
10. Teo KK, Ounpuu S, Hawken S, Pandey MR, Valentin V, et al. Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART Study: a case control study. Lancet 2006; 368(9536):647–658.
11. Religa W, Krzeminska-Pakula M, Bednarkiewicz Z, Shirzynska D. Myocardial infarction in women: Part I. Analysis of acute phase and inhospital period. Med Science Monitor. 1997; 3:518–523.
12. Chen I, Chester M, Kasaki JC. Clinical factors and angiographic features associated with premature coronary artery disease. Chest. 1995; 108(2):364–369.
13. Farmer JA, Gotto AM Jr. Dyslipidemia and other risk factors for coronary artery disease. Heart disease: A textbook of Cardiovascular Medicine. WB Saunders Philadelphia. 1997:1126–1160.
14. Klein KW, Aggarwal JB, Herlich MB, Leary TM, Hellant RH. Prognosis of symptomatic coronary disease to young adults aged 40 years or less. Am J Cardiol. 1987; 60(16):1269–1272.
15. Berenson GS, Wattinghney WA, Tracy RE, Newman WP, Srinivasan SR, et al. Ahterosclerosis of aorta and coronary arteries and cardiovascular risk factors in persons aged 6 to 30 years and studied at necropsy (The Bogalusa Heart Study). Am J Cardiol. 1992; 70(9):851–858.
16. Williams MJA, Restieaux NJ, Low CJS. Myocardial infarction in young people with normal coronary arteries. Heart. 1998; 79(2):191–194.
17. Machete T, Malacrida R, Pasotti E, Sessa F, Genoni M, et al. Epidemiological variables and outcomes of 1972 young patients with acute myocardial infarction. Data from GISSI 2 database. Investigators of the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardico (GISSI-2). Arch Intern Med. 1997; 157(8):865–869.
18. Dagalp Z, Pamir G, Alpman A, Omurlu K, Erol C, et al. coronary artery aneurysme. Report of two cases and of thetature. Angiology. 1996; 47(2):197–201.
19. Weiss EJ, Bray PF, Tayback M, Schulman SP, Kickler TS, et al. A polymorphism of a platelet receptor as an inherited risk factor for coronary thrombosis. NEJM. 1996; 334(17):1090–1094.
20. Corrado D, Thiene GH, Cocco P, Frescurara C. Nonatherosclerotic coronary artery disease and sudden death in young. Br Heart J. 1992; 68(6):601–607.
21. Warren SE, Thompson SI, Vieweg WV. Historic and angiographic features of young adults surviving myocardial infarction. Chest. 1979; 75(6):667–670.