Full Text
Introduction
Acute myocardial infarction (AMI) continues to be a leading cause of morbidity and mortality worldwide. Understanding the early prognostic factors of AMI can provide important information regarding disease stratification and clinical management of patients [1]. As per data obtained in 2019, an estimated 17.9 million people died from CVDs, representing 32% of all global deaths. Of these deaths, 85% of the deaths were due to heart attack and stroke [2]. Similar trends were observed in India as well [3].
Red blood cell distribution width-coefficient of variation (RDW-CV) is an easily available parameter of red blood indices and is a reflection of the variation of the red blood cell volume (anisocytosis) [4]. High RDW levels are now being regarded as a strong and independent risk factor for mortality in many diseases among the general population [5] Tonelli et al [6] carried out the first study to analyse the relationship of RDW levels with all-cause mortality and adverse events in people with coronary artery disease, without symptomatic heart failure, in the University of Alberta in 2008 among 4,111 participants. The study concluded that high RDW levels were associated with higher risk of all-cause mortality in people with coronary artery disease.
There are many prognostic scores for acute myocardial infarction and involves multiple parameter in clinical use. As high RDW has been shown in earlier studies to be related with high mortality amongst acute myocardial infarction, the present study was done to assess the relationship between the widely available RDW values with an established acute myocardial infarction mortality predictor like GRACE score.
The GRACE score is the most commonly used risk stratification system to predict death or myocardial infarction in patients with acute coronary syndrome (ACS). It provides an integrated assessment system for both ST- elevated myocardial infarction (STEMI), and non-ST elevated myocardial infarction (NSTEMI) patients. It is recommended by the American Heart Association Guidelines [7] and the current European Society of Cardiology Guidelines [8].
The GRACE score encompasses multiple parameters, i.e., creatinine level, heart rate, systolic BP, Killip class, age, cardiac arrest at admission, ST segment deviation, and elevated cardiac enzymes. The GRACE score range from 2 to 372. A higher GRACE score on admission predicts higher mortality.
This study aimed to correlate the RDW value on admission in the hospital, as a prognostic marker, by correlating it with the GRACE score, in patients with acute myocardial infarction – STEMI and Non-STEMI.
Patients and methods
The present study was a hospital based prospective observational study and it was conducted on 221 patients of acute myocardial infarction admitted in Department of General Medicine and Department of Cardiology, Silchar Medical College and Hospital, in patients of both sexes aged more than 18 years, from January 2022 to June 2022. The institutional ethical committee of Silchar Medical College approved the study and the ethical clearance number was SMC/22/2020. Before data collection, informed written consent was taken in the patient’s own language.
All the patients with clinical features suggestive of acute myocardial infarction, such as chest pain, dyspnoea, sweating, palpitation, and syncope, and with a history of exposure to risk factors or a family history of ACS, were assessed for acute myocardial infarction. If the diagnosis was established, and the inclusion criteria were fulfilled, then the RDW value of the patients and the GRACE score were calculated.
Patients above 18 years of age of both genders were included if they met the diagnostic criteria for acute myocardial infarction according to the universal definition of myocardial infarction [9] which includes the following - detection of a rise and/or fall in cardiac biomarker values (preferably cTn), with at least one value above the 99th percentile URL, and with at least one of the following: (1) symptoms of ischemia. (2) new or presumed new significant ST-segment–T wave (ST-T) changes or new LBBB. (3) development of pathologic Q waves on the ECG. (4) imaging evidence of a new loss of viable myocardium or a new regional wall motion abnormality. (5) identification of an intracoronary thrombus by angiography or autopsy.
Patients with acute myocardial infarction were excluded from the study if they had anaemia i.e. haemoglobin < 11 g/dl) of any cause, had received a blood transfusion within the past 3 months, were suffering from haematological malignancy, were on previous therapy for myocardial ischemia, had other debilitating conditions like stroke, sepsis, pneumonia; or were receiving anti-platelet drugs, anticoagulant therapy, or immune suppressants.
The patients were divided into two groups: high and low RDW-CV groups, based on the 50th percentile RDW-CV value (13.7). The low RDW-CV group (n = 115) was defined as patients in lower two tertiles (<13.7), and the high RDW-CV group (n = 106) was defined as patients in the upper two tertiles (>13.7).
The primary endpoint of the study was cardiovascular mortality during the hospital stay.
Blood collection and assays
A complete blood count analysis, including the RDW of the sample, was done. Patients' blood samples were taken from the antecubital vein with a 5 ml syringe and immediately mixed in EDTA vacutainers. The sample was run within two hours after venipuncture using an automatic haematology analyzer (Sysmex XN 550) [10]. The Sysmex analyzer works on the principles of the RF/DC detection method, hydrodynamic focusing (DC detection), flow cytometry method (using the semiconductor laser), and SLS-haemoglobin method to perform the complete blood count.
For the analysis of serum cardiac biomarkers, serum creatinine VITRIOS 5600 Integrated System [11] was used, which uses the principles of colorimetry, photometry, and chemiluminescence.
Statistical analysis
A predetermined pro forma was used for collecting the data. Calculations and analysis were done using the Social Statistics Website, [12] Tables and graphs were made using Microsoft Word Plus 2016 and Microsoft Excel Professional Plus 2016 version.
Categorical variables are expressed as the number of patients (frequencies) and the percentage of patients. All the variables did not follow a normal distribution. The chi-square test (χ2) was used to compare the categorical variables. It was used to identify the significance of the relations, associations, and interactions among various variables, e.g. between RDW and GRACE score, in-hospital mortality. For finding the correlation between RDW and GRACE scores, Karl Pearson's correlation coefficient was used to measure the intensity or degree of a linear relationship between two quantitative variables. Continuous variables are expressed as the mean, median, and standard deviation. An independent sample "t" test was used to compare means between the parametric variables and to know whether there was statistical significance between two groups in the parameters measured.
Spearman's rank correlation was used to find the correlation coefficient for qualitative characteristics that could not be measured quantitatively, but were ranked in sequence. An alpha level of 5% was taken, i.e., a p value of less than 0.05 was considered significant.
Definition of variables
The GRACE score was calculated on admission for both the STEMI and NSTEMI patients. [13] It was calculated using the age, heart rate, systolic blood pressure, creatinine value, and physical examination for heart failure according to Killip Classification [14], ST segment deviation, cardiac arrest at admission and elevated cardiac enzymes/markers, upon first arrival in the hospital. In the GRACE scoring system, the patients are grouped into three divisions.
The patients with STEMI were grouped into the following categories, low risk with a GRACE risk score 49–125; intermediate risk with a GRACE risk score 126–154; and high risk with a GRACE risk score 155–319.
For the NSTEMI patients, the groups were low risk with a GRACE risk score of 1–108, intermediate risk with a GRACE risk score of 109–140, and high risk with a GRACE risk score 141-372.
Results
The study included 221 patients with acute myocardial infarction (STEMI or NSTEMI). The mean age of the study population was 58.15 ± 12.45 years. The majority of the population were male (79.64 %) (Table 1).
Table 1: Demographics of patients in two groups according to admission RDW-CV values.
|
Demographics
|
Low RDW-CV
|
High RDW-CV
|
All
patients
|
p- valuec
|
|
No of patients
(n,%)
|
115(52.03)b
|
106(47.96) b
|
221
|
|
|
Age (years)
|
57.57 ±12.22a
|
58.77 ± 12.78a
|
58.15 ± 12.48a
|
|
|
Men
|
101(57.39) b
|
75(42.61) b
|
176 (79.63) b
|
|
|
Heart rate
|
77.26 ±20.42a
|
99.91±11.88a
|
86.69 ±19.50a
|
<0.05 e
|
|
SBP
|
134.99± 25.29a
|
119.75± 21.28a
|
127.70 ±24.45a
|
<0.05 e
|
|
Creatinine
|
1.04 ±0.46a
|
4.04 ±18.07a
|
2.49±12.59a
|
<0.05 e
|
|
Cardiac arrest (at admission)
|
3
|
6
|
9
|
<0.05 d
|
|
STEMI (n,%)
|
85(44.97) b
|
102(53.97) b
|
189
|
<0.05 d
|
|
Trop- I
|
19.79 ±22.49a
|
19.79 ±33.23a
|
28.20±
27.97a
|
<0.05 e
|
|
nT pro BNP
|
2290± 4091.31a
|
3903.58± 5715.66a
|
3064.34±
4980.47a
|
<0.05 e
|
|
Killip class ≥3
|
103
|
118
|
121
|
<0.05 e
|
|
GRACE score
|
143± 33.19
|
189.67± 38.67
|
173.71±38.99
|
<0.05
|
|
Mortality, n
|
4(25) b
|
12(75) b
|
16
|
<0.05d
|
Abbreviations: a: mean ± standard deviation; b: the number in brackets includes the percentage; c: significance of association; d: Chi-square test; e: test of association.
Higher RDW-CV on admission was significantly associated with increased age, tachycardia, lower systolic BP, higher creatinine, Trop-I, and nT pro BNP values (p<0.05). Patients with high RDW -CV had higher Killip class and more number of cardiac arrests. RDW - CV score of ≥ 13.7 correlated with a higher GRACE score of 189.67± 38.67 and was associated with higher mortality (p = 0.049, level of significance p< 0.05) (Table 1).
In patients with STEMI and NSTEMI, the patients in the high-risk group, according to GRACE score, also had significantly more patients in the higher RDW-CV group, than the low-risk and intermediate-risk groups (Table 2).
Table 2: The relationship between RDW-CV, GRACE risk Groups, and GRACE risk score in STEMI/ NSTEMI patients STEMI.
|
STEMI
|
|
GRACE risk group in-hospital mortality
|
Low RDW-CV
|
High RDW-CV
|
p a
|
|
Low (n,%)
|
14 (70)b
|
6(30) b
|
<0.05c
|
|
Intermediate (n,%)
|
39(81.25) b
|
9(18.75) b
|
|
High (n,%)
|
49(41.18) b
|
70(58.82) b
|
|
NSTEMI
|
|
Low (n,%)
|
0(0)
|
0(0)
|
<0.05c
|
|
Intermediate (n,%)
|
5(100)
|
0(0)
|
|
High (n,%)
|
8(27.59) b
|
21(72.41) b
|
Abbreviations: a: mean ± standard deviation; b: the number in bracket includes the percentage; c: Chi square test.
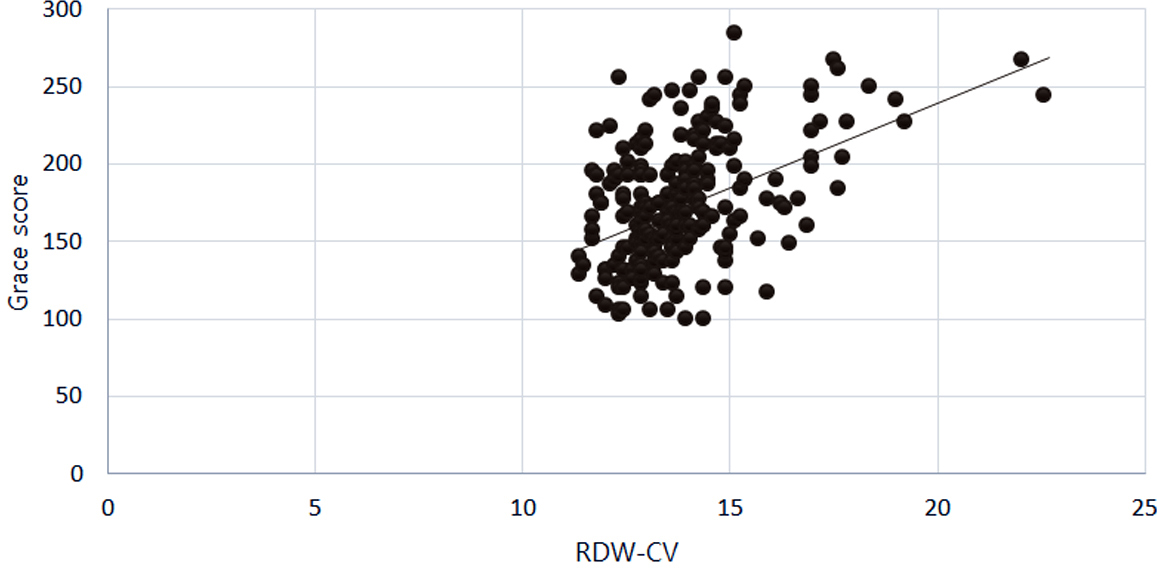
Figure 1: Correlation of RDW-CV and GRACE score: The r value of Pearson’s correlation coefficient test is R= 0.47, p 0.05. There was a positive correlation between RDW-CV and GRACE risk scores of in-hospital death (Pearson’s correlation coefficient, R= 0.47, p<0.05.
Discussion
The majority of the patients in our study were men (79.63 %) in the age group of 50–60 years. There were 115 (52.03%) patients in the low RDW group and 106 (47.96%) patients in the higher RDW group. The patients in the higher RDW group had a higher mean GRACE score as compared to the lower RDW group, with a significant association (p<0.05).
A similar retrospective study carried out by Polat et al [15] in 193 patients of NSTEMI or unstable angina showed similar results to our study, where they found a positive correlation between RDW and GRACE score, with the end point of in-hospital mortality and 6-month mortality.
A similar retrospective cohort study, by Sangoi et al [16] conducted in Brazil with 109 patients, showed that RDW is an independent predictor of in-hospital mortality, suggesting that RDW may provide additional information to the GRACE risk score in patients with AMI.
The study found that red cell distribution width levels were strongly associated with higher GRACE scores in patients who died in hospital due to acute myocardial infarction.
The majority of the patients in our study were men (79.63 %) in the age group of 50–60 years. There were 115 (52.03%) patients in the low RDW group and 106 (47.96%) patients in the higher RDW group. The patients in the higher RDW group had a higher mean GRACE score as compared to the lower RDW group, with a significant association (p<0.05) (Table 2).
A similar retrospective study carried out by Polat et al [15] in 193 patients of NSTEMI or unstable angina showed similar results to our study, where they found a positive correlation between RDW and GRACE score, with the end point of in-hospital mortality and 6-month mortality.
A similar retrospective cohort study, by Sangoi et al [16] conducted in Brazil with 109 patients, showed that RDW is an independent predictor of in-hospital mortality, suggesting that RDW may provide additional information to the GRACE risk score in patients with AMI.
In the study, it was seen that red cell distribution width levels were strongly associated with high GRACE scores in patients suffering from in-hospital mortality due to acute myocardial infarction.
The study also showed that RDW was independently associated with several cardiovascular risk factors and biochemical risk markers of acute MI included in the GRACE score, such as age, heart rate, systolic blood pressure, creatinine, cardiac arrest at admission, ST-elevation in ECG, cardiac biomarkers, and Killip classification.
It can be inferred from this study that RDW can be regarded as an inexpensive mortality marker in patients with acute myocardial infarction, and this was also the conclusion derived in several previous studies [17, 18].
The mechanism as to how the elevated RDW levels impact the prognosis in coronary artery disease remains unclear, but many studies suggest that it may be because RDW reflects the factors that independently affect the prognosis in MI, such as anaemia, chronic inflammation, oxidative stress, glucose levels, vitamin D3 and iron deficiency. Thus, increased RDW values may reflect the intensity of these phenomena. [19], which is also a poor prognostic indicator for acute myocardial infarction.
In a state of hypoxia, stimulation of erythropoiesis by erythropoietin (EPO) promotes the release of enlarged RBCs from bone marrow, similarly, chronic inflammation shortens the life span of erythrocytes by affecting membrane stability, which may impact RDW values. Since RBCs have a massive oxygen carrying capacity, any alteration in RBC morphology will also independently contribute to tissue injury in MI, which is reflected in the RDW value.
Further, since RDW is positively correlated with a well-established marker of mortality, i.e. GRACE risk score, it can be used as a useful marker in emergency settings and in areas with low financial capacity.
Our study is one of the few prospective studies carried out till date, most of the other studies being retrospective. Thus, it is hoped that further studies will be done on this inexpensive, easily available upcoming marker to be used as a screening tool to predict the prognosis of a dreaded disease, with a high global burden. i.e., acute myocardial infarction, leading to optimizing resources and treatment.
Limitations: A mutli-centre and large sample size study would be required to confirm the study. The patients were followed up only until their hospital stay, and the long-term prognosis could not be assessed. A few confounding parameters that additionally affect the significance of RDW, e.g., serum vitamin D3 levels and inflammatory markers like CRP and ferritin levels, were not assessed.
Conclusion
The present era aims for complete dependence on evidence-based medicine. The recommended mortality scores in acute myocardial infarction, like the GRACE score, use multiple parameters, the results of which may not be readily available. The present study showed that higher RDW-CV was associated with higher in-hospital mortality in patients with acute myocardial infarction and positively correlated with higher GRACE score and could serve as a poor prognostic marker in acute myocardial infarction.
Acknowledgements
Staff of the Silchar Medical College and Hospital.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Yao J, Xie Y, Liu Y, Tang Y, Xu J. Prediction factors of 6-month poor prognosis in acute myocardial infarction patients. Frontiers Cardiovas Med. 2020; 7:130.
[2] WHO. Cardiovasculardiseases. 2021; Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
[3] Huffman MD, Jeemon P, Prabhakaran D, Harikrishnan S, Leeder S. A race against time II: the challenge of cardiovascular diseases in developing economies. Available from: https://www.scholars.northwestern.edu/en/publications/a-race-against-time-ii-the-challenge-of-cardiovascular-diseases-i-2
[4] Bujak K, Wasilewski J, Osadnik T, Jonczyk S, Kołodziejska A, et al. The prognostic role of red blood cell distribution width in coronary artery disease: a review of the pathophysiology. Disease Markers. 2015; 2015:824624.
[5] Yousefi B, Sanaie S, Ghamari AA, Soleimanpour H, Karimian A, et al. Red cell distribution width as a novel prognostic marker in multiple clinical studies. Indian J Crit Care Med. 2020; 24:49–54.
[6] Tonelli M, Sacks F, Arnold M, Moye L, Davis B, et al. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation. 2008; 117:163–168.
[7] 2012 Writing Committee Members, Jneid H, Anderson JL, Wright RS, Adams CD, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/Non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update) A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation. 2012; 126:875–910.
[8] Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, et al. ESC Guidelines for themanagement of acute coronary syndromes in patients presentingwithout persistent ST-segment elevation: The Task Force for themanagement of acute coronary syndromes (ACS) in patients presentingwithout persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2011; 32:2999–3054.
[9] Thygesen K, Alpert JS, White HD, Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J Am College Cardiol. 2007; 50:2173–2195.
[10] Sysmex. Leading haematology for better patient care - sysmex. Available from: https://www.sysmex-ap.com/wp-content/uploads/2020/05/XN-L-Brochure-E-Book.pdf
[11] VITROS® 5600 integrated, Ortho clinical diagnostics. Available from: https://go.orthoclinicaldiagnostics.com/us/en/clinical-labs/vitros-systems/integrated-systems/vitros-5600
[12] Social Science Statistics. Available from: https://www.socscistatistics.com
[13] Tang EW, Wong CK, Herbison P. Global Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndrome. Am Heart J. 2007; 153:29–35.
[14] Killip T, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967; 20:457–464.
[15] Polat N, Yildiz A, Oylumlu M, Kaya H, Acet H, et al. Relationship between red cell distribution width and the GRACE risk score with in-hospital death in patients with acute coronary syndrome. Clin Appl Thromb Hemost. 2014; 20:577–582.
[16] Sangoi MB, Rodel AP, Zorzo P, Borges PO, Cargnin LP, et al. Prognostic value of red blood cell distribution width in prediction of in-hospital mortality in patients with acute myocardial infarction. Clin Lab. 2014; 60:1351–1356.
[17] Tonelli M, Sacks F, Arnold M, Moye L, Davis B, et al. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation. 2008; 117:163–168.
[18] Skjelbakken T, Aard JL, Ellingsen TS, Connor EB, Brox J, et al. Red cell distribution width is associated with incident myocardial infarction in a general population: The tromso study. J Am Heart Assoc. 2014; 3:e001109.
[19] Warren J. Remarks on angina pectoris. N Engl J Med. 1962; 266:3–7.