Original Research
2017
June
Volume : 5
Issue : 2
Right vertical infra axillary thoracotomy: Anatomically and cosmetically a superior approach for repair of simple congenital cardiac defects
Rajesh Kishan Rao, Girish B, Jayaprakash, Nikhil S
Pdf Page Numbers :- 49-52
Rajesh Kishan Rao1,*, Girish B1, Jayaprakash1 and Nikhil S1
1Department of Cardiothoracic Surgery, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bangalore-560 069, Karnataka, India
*Corresponding author: Dr. Rajesh Kishan Rao, MS., MCh., Associate Professor, Department of Cardiothoracic Surgery, Sri Jayadeva Institute of Cardiovascular Sciences and Research. Bannergatta Road, Jayanagar 9th block, Bangalore-560069, Karanataka, India. Mobile: +9198869 64031; Fax: 080-22977422; Email : merajesh14@yahoo.com
Received 25 January 2017; Revised 16 March 2017; Accepted 23 March 2017; Published 31 March 2017
Citation: Rao RK, Girish B, Jayaprakash, Nikhil S. Right vertical infra axillary thoracotomy: Anatomically and cosmetically a superior approach for repair of simple congenital cardiac defects. J Med Sci Res. 2017; 5(2):49-52. DOI: http://dx.doi.org/10.17727/JMSR.2017/5-10
Copyright: © 2017 Rao RK et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: To evaluate the safety of Right Vertical Infra Axillary Thoracotomy (RVIAT) for the repair of simple congenital cardiac defects in adolescent girls.
Method: Between February 2016 and July 2016 we performed intracardiac repair for ostium secundum defects in 16 adolescent girls through RVIAT. Median age and weight was 14.5yrs and 33.5Kg respectively. All patients were approached through right vertical infra-axillary incision and right plural cavity was entered through third intercostal space. Cardio Pulmonary Bypass (CPB) was instituted with aortic and bicaval cannulation. Regular aortic cross clamp was used and cardioplegic arrest was employed in all the patients. In nine patients the defect was closed with autologous pericardium and in seven patients direct closure was done.
Results: Operative time, CPB and clamp time were slightly longer in our study repair was safely performed with central cannulation in all the patients. There was no conversion to another approach. At fifth month follow up all were in sinus rhythm with no residual defects. There was no deformity of the thorax or asymmetry of the breast.
Conclusion: RVIAT can be safely performed for repair of simple congenital cardiac defects without compromising the quality of repair. This approach does not interfere with growth of breast tissue, does not cause deformity of the thorax and can be performed with regular instruments and cannulae.
Keywords: RVIAT; atrial septal defects; anterolateral thoracotomy
Full Text
Introduction
In cardiac surgery least importance is given to the cosmesis, as it is important to achieve safe and reliable cardiac repair. If a good quality of repair is provided by a cosmetically superior approach many will opt for such approaches.
Anterolateral thoracotomy once considered a cosmetically superior approach has lead to less optimal than expected results, as it causes deformation of the thoracic cage and assymetirc development of the breast in pre-pubescent and adolescent girls [1, 2]. Right Vertical Infra Axillary Thoracotomy (RVIAT) is away from the breast bud and also away from anterior and posterior hinge points of the ribs. Hence this approach does not interfere with development of breast and does not cause deformity of the thorax. It can be performed safely with central cannulation with excellent cosmetic results [3].
This approach can also be used to repair other defects like ventricular septal defects (VSD) [4], Ostium Primum defects [5], Sinus Venosus with partial anomalous pulmonary venous connection, Mitral and Aortic valve replacements [6, 7].
Method
Between February 2016 and July 2016 we selected adolescent girls with Ostium Secundum Atrial Septal Defects (OS-ASD) who were not suitable for device closure. Total number of patients were 16. Informed consent was taken and this study was approved by ethical committee of our institution. Median age and weight was 14.5yrs and 33.5Kg respectively. Demographic and clinical data of the patients are summarized in Table 1.
Table 1: Demographic and clinical data of the patients.
|
Median age(yrs)
|
Median weight(Kg)
|
Median CPB time(min)
|
Median clamp time(min)
|
|
14.5(10-19)
|
33.5(21-44)
|
56(46-65)
|
34.6(26-41)
|
Surgical technique
Single lumen endotracheal tube was used. Trans-esophageal echocardiogram was used intraoperatively to assess the quality of repair and adequacy of de-airing. Patients were placed in 60o - 70o left lateral position with pelvis in a corresponding 45o. The right upper limb was brought over the head and supported by a sling (Figure 1). Right groin was prepared and draped. External defibrillator pads are used in all the cases.

Figure 1: 60o–70o left lateral position.
A 4 - 5 cm vertical skin incision was made in the mid axillary line extending from 2nd to 5th intercoastal space. Flaps are developed in the subcutaneous tissue to allow incision mobility, relative to the chest spreader. 3rd intercostal space was exposed after going through the fibers of serratus anterior parallel to the rib. Right plural cavity entered through third space and lung was retracted posteriorly. Pericardiotomy was done 3 - 4 cm anterior to the phrenic nerve. Pericardial stay sutures are placed and brought out through the skin. This brings ascending aorta and heart closer by 3 - 4 cm.
Cardio pulmonary bypass (CPB)
CPB was instituted with aortic (EOPA, 18Fr - 22Fr) and bicaval (Metal tip or straight , DLP 18Fr - 24Fr) cannulation. Regular aortic cross clamp was used and cold blood cardioplegia was administered through the aortic root (Figure 2). Operative field was flooded with CO2 continously. OS-ASD was closed with autologous pericardium in nine patients and in seven patients closed directly.
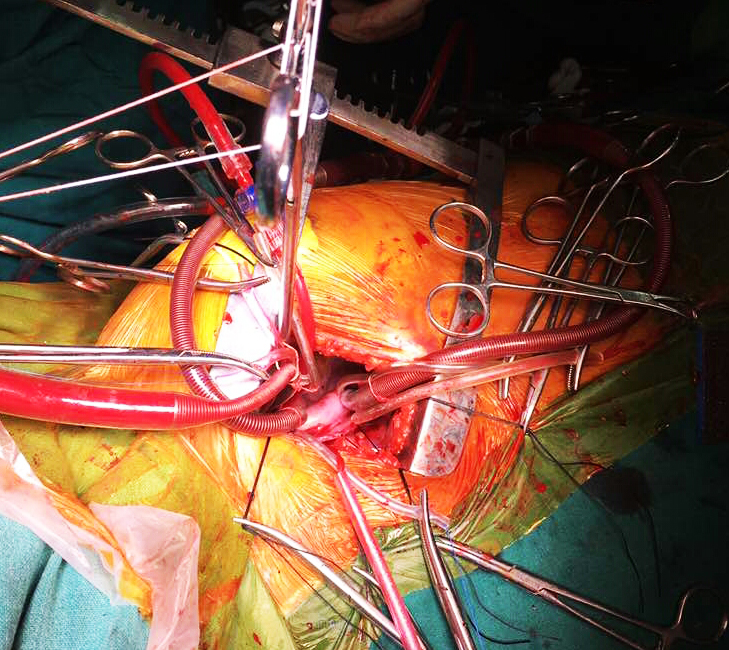
Figure 2: Intra-operative image- central cannulation with cross clamp.
Results
Intracardiac repair was safely performed with central cannulation in all the cases, there was no conversion to another approach. There were no neurological deficits, wound complications, re-exploration or mortality. Extracorporeal circulation time and cross clamp time were longer as this approach needs a greater technical challenge in setting up cardiopulmonary bypass. At fifth month follow-up all patients were in sinus rhythm with no residual defects. Also there was no deformity of the thorax or asymmetry of the breast.
Discussion
Repair of simple congenital cardiac defects like OS-ASD can be safely performed through RVIAT. The same approach can be used to repair wide range of congenital defects [8] like VSD [4], ostium primum defects [5], sinus venosus defects with partial anomalous pulmonary venous connection, mitral and aortic valve replacements [6, 7]. Repair can be performed with central cannulation or peripheral cannulation or combination of both. Through RVIAT approach repair can be safely performed with central cannulation only, thus avoiding peripheral cannulation and its subsequent complications like future femoral artery stenosis especially in smaller children [9].
In cardiac surgery least importance is given to the cosmesis, as it is important to achieve safe and reliable cardiac repair, which not only affect life expectancy and also the quality of life. If a good quality of repair is provided by a cosmetically superior approach many will opt for such approaches. This approach provides excellent cosmesis [3] as the scar is hidden under the arms (Figure 3).

Figure 3: Post-operative healed skin incision.
Development of the breast is at its peak during adolescence. As this approach is away from the anterior axillary line, it avoids injury to the mammary glands. Hence this approach will not interfere with development of breast thereby it avoids asymmetry of the breast [1, 2, 10].
This approach avoids deformity of the thorax, which is seen in some patients after anterolateral thoracotomy due to severing of pectoral muscles and rib deformation [2]. Axillary part of the ribs are away from costochondral and costovertebral junction. Therefore there will be minimal stress on the ribs and their attachments when spread apart in this region. Also the rib fractures are very rare in this approach.
Conclusion
Apart from cosmesis RVIAT is safe for repair of wide range of congenital cardiac defects located at the atrial level and close to atrioventricular junction. This approach does not interfere with growth of breast tissue, hence does not cause asymmetry of the breast, especially in pre-pubescent and adolescent girls. Since it is a muscle sparing approach does not cause deformity of the thorax. It can be performed safely with central cannulation with regular instruments.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Bleiziffer S, Schreiber C, Burgcart R, Regenfelder F, Kostolny M, et al. The influence of right anterolateral thoracotomy in prepubescent female patients on late breast development and on the incidence of scoliosis. J Thorac Cardiovasc Surg. 2004; 127(5):1474-1480.
[2] Cherup LL, Siewers RD, Futrell JW. Breast and pectoral muscle development after anterolateral and posterolateral thoracotomies in children. Ann Thorac surg. 1986; 41(5):492-497.
[3] Neguyen K, Chin C, Lee D S, Mittnacht A, Srinivas S, et al. The Axillary incision: A cosmetic approach in congenital cardiac surgery. J Thorac Cardiovasc Surg. 2007; 134(5):1358-1360.
[4] Wang Q, Li QG, Zhang J, Wu Z, Zhou Q, et al. Ventricular septal defect closure using a minimal right vertical infra axillary thoracotomy: Seven year experience in 274 patients. Ann Thorac Surg. 2010; 89(2):552-555
[5] Yang X, Wang D, Wu Q. Repair of partial atrioventricular septal defects through a minimal right vertical infra axillary thoracotomy. J Card Surg. 2003; 18(3):262-264
[6] Wang D, Wang Q, Yang X, Wu Q, Li Q. Mitral valve replacement through a minimal right vertical infra axillary thoracotomy versus standard median sternotomy. Ann Thorac Surg. 2009; 87(3):704-708.
[7] Ito T, Maekawa A, Hoshino S, Hayashi Y. Right infra axillary thoracotomy for minimally invasive aortic valve replacement. Ann Thorac Surg. 2013; 96(2):715-717.
[8] Dave HH, Comber M, Solinger T, Bettex D, Dodge-Khatami A, et al. Mid-term results of right axillary incision for repair of wide range of congenital cardiac defects. Eur J Cardiothorac Surg. 2009; 35(5):864-870.
[9] Shirasava B, Hamano K, Katoh T, Fujimura Y, Tsuboi H, et al. A case report of open heart surgery in an infant with MNMS caused by femoral arterial cannulation during cardiopulmonary bypass. Nihon Kyobu Geka Gakkai Zasshi. 1996; 44(10):1902-1906.
[10] Schreiber C, Bleiziffer S, Lange R. Mid-axillary lataral thoracotomy for closure of atrial septal defects in pre-pubescent female children : Reappraisal of an “old technique”. Cardiol Young. 2003; 13(6):565-567.