Orginal Research
2023
March
Volume : 11
Issue : 1
Subchondral raft plate fixation for lateral tibial plateau fractures - A prospective study
Kumar KA, Kumar SSS, Jayachandran N, Shibu R
Pdf Page Numbers :- 32-36
Akhil Kumar K1, Santhosh Kumar SS1, Jayachandran N1 and Shibu R1,*
1Department of Orthopaedics, Government Medical College, Thiruvananthapuram, Kerala-695011, India
*Corresponding author: Dr. R. Shibu, Assistant Professor, Department of Orthopaedics, Government Medical College, Thiruvananthapuram, Kerala-695011, India. Email: drshibur@gmail.com
Received 30 August 2022; Revised 2 November 2022; Accepted 16 November 2022; Published 29 November 2022
Citation: Kumar KA, Kumar SSS, Jayachandran N, Shibu R. Subchondral raft plate fixation for lateral tibial plateau fractures - A prospective study. J Med Sci Res. 2023; 11(1):32-36. DOI: http://dx.doi.org/10.17727/JMSR.2023/11-7
Copyright: © 2023 Kumar KA et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Tibial plateau fractures are often complex fractures that are difficult to stabilize. Subchondral raft technique is used to prevent depression and reduction loss using Kirschner wires, lag screws or locking screws with or without plates. The study aimed to assess the functional outcome of lateral tibial plateau fractures fixed with raft plate and the associated complications.
Materials and methods: A prospective observational study of 45 consecutive patients with depressed lateral tibial plateau fractures treated with raft plate were studied at a tertiary care centre for a period of one year. Patients were followed up for a minimum period of 6 months. The Lysholm Knee Scoring Scale (LKSS) was used to assess the functional outcomes.
Results: The mean age of the patients was 43.8 ± 10.54 years (range 18-60 years). Male- Female ratio was 2.75:1 (M=33, F=12). Proportion of type II Schatzker fractures was 44.4%. 35 patients (77.8%) sustained injury due to road traffic accident and the rest due to fall. Bone grafting was done in 18 patients (40%). Knee stiffness and flexion less than 95⁰ were noted in 5 patients (11.1%). Superficial wound infection was noted in 2 patients (4.4%). Knee pain was observed in 7 patients (15.6%).
Conclusion: Laterally placed raft plate with periarticular locking screws through it offers an excellent method of fixation of tibial plateau fractures, which preserves the anatomical joint line and the normal mechanical axis with minimal complications. Raft plating may obviate the need for dual plating in most of the tibial plateau fractures.
Keywords: tibial plateau fracture; Schatzker classification; raft plate; anterolateral approach; locking screws
Full Text
Introduction
Tibial plateau fractures account for 1% of all fractures [1]. The fragmentation and displacement of fracture is determined by the magnitude of energy. The widely used classification to assess the severity and morphology of these fractures is the Schatzker classification [2, 3]. Lateral tibial plateau fractures are more common because it is thinner, convex, relatively weaker and more proximal than medial plateau [3]. Lateral tibial plateau split-depressed fractures (Schatzker type II) may result from low energy injuries in osteoporotic bone [3]. Of the tibial plateau fractures, Schatzker type II accounts for 25%-33% [4, 5].
Tibial plateau fractures are often complex fractures that are difficult to stabilize. A thorough knowledge of anatomy is required for adequate reconstruction, early mobilization and to prevent long term complications [6]. Fixation of these fractures can be done through conventional or minimally invasive arthroscopic aided methods [7-9]. Anterolateral approach along with lateral buttress plating is used generally [10, 11]. Subchondral raft technique is used to prevent depression and reduction loss using Kirschner wires, lag screws or locking screws with or without plates [12, 13]. Rafting is a technique by which parallel screws are passed subchondrally such that it retains the articular congruity once the fracture is reduced. After elevation of subchondral bone, fixation of lateral cortex is done with a ‘raft’ plate, through which subchondral raft screws are placed [14]. Raft plate is a buttress plate which is pre-contoured for lateral tibial plateau through which locking 3.5mm screws can be placed. Only few studies are there in literature about the outcome of lateral tibial plateau fractures treated with raft plate [14, 15].
The aim of this study was to assess the functional outcome of lateral tibial plateau fractures fixed with raft plate and the associated complications.
Materials and methods
Study was done as a prospective observational study at Department of Orthopaedics, Government Medical College, Thiruvananthapuram, Kerala for a period of one year from October 2020 to September 2021 after Institutional Ethics Committee clearance.
All consecutive patients in the age group 18 to 60 years, with depressed lateral tibial plateau fractures treated with raft plate; who gave written informed consent were included in the study. The exclusion criteria were – open fractures, type 1,4,6 Schatzker fractures, poly trauma patients, associated neurovascular injuries and patients who were lost in the follow up. There were a total of 45 patients who were followed up for a minimum period of 6 months.
Surgical technique
All surgeries were done in supine position under spinal anaesthesia, with a bolster under knee to allow knee flexion. All patients were given Inj. cefuroxime-sulbactum 1.5g IV preoperatively as routine prophylaxis. Anterolateral approach based on Gerdy’s tubercle extending distally over anterior compartment, was used to expose the fracture site. Care was taken along the posterolateral border of the tibia to protect the anterior tibial artery. Submeniscal arthrotomy was done to evaluate intra articular damage. The fracture fragments elevated and reduced under direct vision. Bone graft from ipsilateral iliac crest was used to fill large voids after elevation. A large compression clamp was applied across the transverse diameter of tibia under fluoroscopy to maintain reduction. In grossly comminuted cases, provisional fixation with Kirschner wires were used. Finally, a raft plate (Figure 1) was applied on the lateral aspect and fracture stabilized with multiple locking screws through the plate. The raft screws were placed as periarticular screws just below subchondral bone, in such a way that it extends from lateral raft plate to medial cortex of medial tibial plateau, under fluoroscopic guidance. The distal part of plate was fixed with locking screws to the tibial diaphysis (Figure 2).

Figure 1: Raft plate.
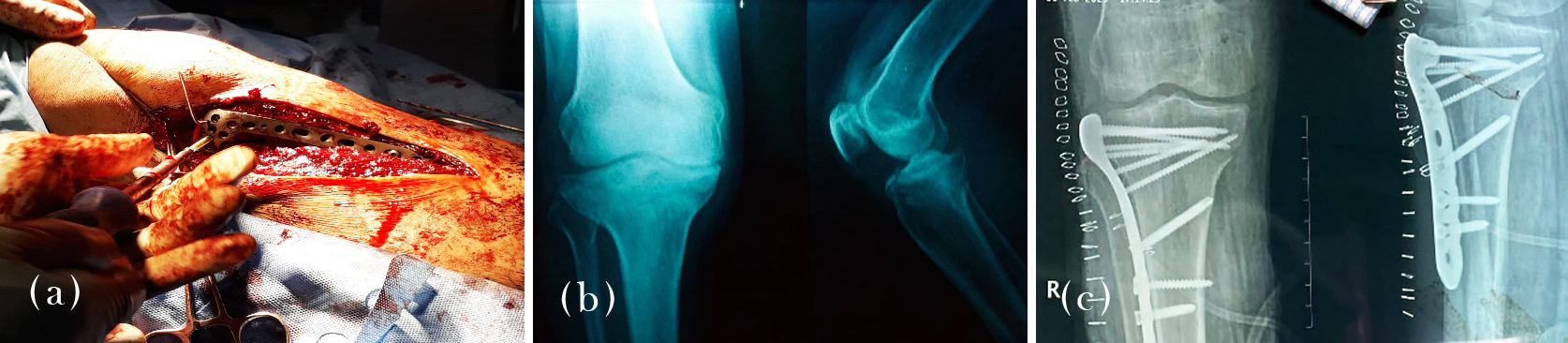
Figure 2: (a) Raft plate placement, (b, c) Raft plate fixation (pre-op and post-op).
Post-operatively, intravenous antibiotics continued for 3 days. Quadriceps exercise and range of motion exercises were started as early as pain tolerated. Patients were discharged on 5-14 post-op days with instructions to continue knee mobilization and quadriceps exercises; and non-weight bearing. Sutures were removed after 2 weeks. Patients were followed up monthly. Partial weight bearing was advised at 6-12 weeks and full weight bearing at 12-16 weeks post-op, depending on radiological union.
Statistical analysis
Data was collected using a study proforma and Lysholm Knee Scoring Scale (LKSS) was used to assess the functional outcome [16]. The LKSS is a 100-point scoring system for knee specific symptoms including mechanical locking, pain, instability, swelling, climbing stairs, squatting and need for support. Score of 91-100 was considered excellent; 84-90 as good; 65-83 as fair and ≤ 64 as unsatisfactory. The patients were reviewed at 1 month, 3 months and 6 months. The LKSS score at 6 months were analysed. Data were entered in MS excel and analysed using statistical software SPSS V-24.0 (IBM Corp, Armonk, NY, USA). Categorical variables were expressed as percentages and continuous variables as mean and standard deviation.
Results
The mean age of the patients in this study was 43.8 ± 10.54 years (range 18-60 years) (Table 1). Majority were in the age group 41-50 years. Male- Female ratio was 2.75:1 (M=33, F=12) (table 2). Injury was on right side for 24 and left side for 21 patients (Table 2).
Table 1: Age distribution.
|
Age Group
|
Type 2
|
Type 3
|
Type 5
|
|
18-30
|
3
|
2
|
1
|
|
31-40
|
2
|
2
|
1
|
|
41-50
|
10
|
6
|
7
|
|
51-60
|
5
|
3
|
3
|
Note: Mean age = 43.8 ± 10.54 years.
Table 2: Sex and side distribution.
|
Type of fracture
|
Male
|
Female
|
Right
|
Left
|
|
Type 2
|
14
|
6
|
12
|
8
|
|
Type 3
|
9
|
4
|
7
|
6
|
|
Type 5
|
10
|
2
|
5
|
7
|
Note: Male: Female= 2.75: 1
Proportion of type 2 was more (44.4%) compared to type 4 (28.9%) and type 5 (26.7%) (Table 3). Thirty eight patients (84%) sustained injury due to road traffic accident and the rest due to fall (Table 3). Bone grafting was done in 18 patients (40%). Mean range of movement (knee flexion) for patient with raft plating at 6 months was 107⁰ ± 9.32⁰ (Table 4).
Table 3: Type of fracture and mode of injury.
|
Type of fracture
|
No. of patient
|
Percentage
|
Road traffic accident
|
Fall
|
|
Type 2
|
20
|
44.4
|
16
|
4
|
|
Type 3
|
13
|
28.9
|
9
|
4
|
|
Type 5
|
12
|
26.7
|
13
|
2
|
Table 4: Range of motion at 6 months.
|
Range of motion
|
Type 2
|
Type 3
|
Type 5
|
|
75⁰-85⁰
|
0
|
0
|
1
|
|
86⁰-95⁰
|
2
|
2
|
2
|
|
96⁰-105⁰
|
5
|
3
|
3
|
|
106⁰-115⁰
|
11
|
7
|
5
|
|
116⁰-125⁰
|
2
|
1
|
1
|
Note: Mean ROM = 107⁰ ± 9.32⁰.
Duration of post-operative hospital stay ranged from 5-14 days, with mean duration being 8.3 ± 2.1 days. Mean time of union was 14 weeks (range 13 - 18 weeks). The Lysholm knee score at 6 months showed excellent outcome for 20 patients (44.4%), good outcome for 15 (33.3%), fair outcome for 8 (17.8%) and poor outcome for 2 (4.5%). The mean Lysholm knee score was 88.933 ± 10.718 (Table 5). In 18-30, 31-40, 41-50 age groups, the excellent outcomes were accounted for 50%, 60% and 48% respectively (Table 6). Only 27% in the age group 51-60 years showed excellent outcome. 2 patients (18%) in that age group showed poor outcome. Knee stiffness and flexion less than 95⁰ were noted in 5 patients (11.1%) (Table 7). Superficial wound infection was noted in 2 patients (4.4%). Knee pain was observed in 7 patients (15.6%) (Table 7).
Table 5: Lysholm knee score.
|
Knee score
|
Frequency
|
Percentage
|
|
Poor
|
2
|
4.5
|
|
Fair
|
8
|
17.8
|
|
Good
|
15
|
33.3
|
|
Excellent
|
20
|
44.4
|
Note: Mean Lysholm knee score = 88.933 ± 10.718.
Table 6: Age dependent functional outcome.
|
Age group
|
Number of patients
|
Average knee score
|
Grading
|
|
Excellent
|
Good
|
Fair
|
Poor
|
|
18-30
|
6
|
91.0+/-9.27
|
3
|
2
|
1
|
0
|
|
31-40
|
5
|
91.8+/-8.93
|
3
|
1
|
1
|
0
|
|
41-50
|
23
|
92.5+/-6.13
|
11
|
10
|
2
|
0
|
|
51-60
|
11
|
79.0+/-14.25
|
3
|
2
|
4
|
2
|
Table 7: Complications.
|
Complications
|
Type 2
|
Type 3
|
Type 5
|
|
Knee-stiffness
|
2
|
1
|
2
|
|
Infection
|
0
|
1
|
1
|
|
Pain
|
3
|
2
|
2
|
Discussion
Mean age of the patients in this study was 43.8 ± 10.54 years. The majority of the patients were in the age group of 41-50 years. This is similar to mean age of 42.7 years in the study conducted by Kulkarni et al [15]. 38 patients (84%) sustained injury due to road traffic accident. In our study, males outnumbered females in the ratio of 2.75:1. This can be explained by the more active lifestyle of males and hence more chance of road traffic accidents. In the study conducted by Kulkarni et al., the male : female ratio was 4.42:1. Type II fractures constituted 44.4% in the present study. Schatzker type II accounts for 25%-33% as per literature [4, 5]. The mean range of movement was 107o ± 9.32o and in the study conducted by Kulkarni et al. the mean range of movement was 118o. In our study, among 45 patients, 20 had an excellent outcome (44.4%), 15 had good outcome (33.3%), 8 had a fair outcome (17.7%). The mean Lysholm knee score was 88.933 ±10.718. This is similar to the functional outcome in the study conducted by Kulkarni et al., who studied 38 patients of lateral tibial plateau fracture treated with raft plate and the Lysholm knee score was excellent in 26 patients, good in 8 and fair in 4 patients.
Bone grafting was employed in 18 out of 45 patients, mainly to fill up metaphyseal defect after elevation of depressed lateral articular surface fragment, to prevent the chance of late metaphyseal collapse. Mean time for union was 14 weeks, ranges from 13 to 18 weeks. Bone grafting did not contribute to faster healing as metaphyseal fracture can be expected to heal faster even without grafting. Major complications found in our study were knee-stiffness, superficial wound infection and knee-pain. Knee-Stiffness and flexion less than 95o were noted in 5 patients (11.1%). Superficial wound infection was noted in 2 patients (4.4%) and was treated with parenteral antibiotics for one week. Knee pain was observed in 7 patients (15.5%). Norris et al. reported that 6.4% patients of proximal tibial fractures had deep surgical site infection [17]. We had no case of deep surgical site infection.
A major concern after treatment of tibial plateau fractures is post traumatic arthrosis [18, 19]. According to Parkkinen et al., post-operative articular congruity and normal mechanical axis were the factors predicting the development of early arthritis [20]. They reported a valgus malalignment ≥5° and articular depression >2 mm lead to severe arthritis. Meticulous elevation of fracture fragments and correction of normal mechanical axis should be seriously met with while fixing tibial plateau fractures [21]. The subchondral raft technique is a method used to resist depression of subchondral fragments and loss of reduction [13]. Cole et al., reported that unstable, comminuted fragments can be kept in their reduced position by placing a raft of small diameter screws parallel to and just below the articular surface. The raft screws are better placed through a buttress or raft plate in such a way that the screws are locked laterally at the plate and fixed medially in the intact medial column of bone [14, 15].
Thamyongkit et al., reported that bicondylar tibial plateau fractures treated with combined medial and lateral locking compression fixation did not offer adequate stability for allowing early full weight bearing [22]. Zhang et al., in their study comparing double plate fixation and locking plate fixation opined, that more effective improvement in clinical symptoms of tibial plateau fracture patients were found in locking plate fixation. Patients with locking plate internal fixation showed shorter fracture healing time and earlier recovery of knee joint function with improved activities of daily living [23]. Chang et al., in a meta-analysis comparing single lateral locking plate with dual plate fixation in highly comminuted bicondylar tibial plateau fractures, concluded that there were no significant differences in the final outcomes. Also incision necrosis, union time and surgical time were lower in single plate group [24]. Biomechanical analysis of single lateral plate versus dual plate by Vélez et al, reported no statistically significant difference [25].
The shortcomings of the present study were a short follow-up and absence of a comparison group.
Conclusion
Laterally placed raft plate with periarticular locking screws through it offers an excellent method of fixation of tibial plateau fractures, which preserves the anatomical joint line and the normal mechanical axis with minimal complications. Raft plating may obviate the need for dual plating in most of the tibial plateau fractures.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Elsoe R, Larsen P, Nielsen NP, Swenne J, Rasmussen S, et al. Population-based epidemiology of tibial plateau fractures. Orthopedics. 2015; 38:e780–e786.
[2] Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968–1975. Clin Orthop Relat Res. 1979; 138:94–104.
[3] Kfuri M, Schatzker J. Revisiting the Schatzker classification of tibial plateau fractures. Injury. 2018; 49:2252–2263.
[4] Zhai Q, Luo C, Zhu Y, Yao L, Hu C, et al. Morphological characteristics of split-depression fractures of the lateral tibial plateau (Schatzker type II): A computer-tomography-based study. Int Orthop. 2013; 37:911–917.
[5] Zhu Y, Yang G, Luo CF, Smith WR, Hu CF, et al. Computed tomography based three-column classification in tibial plateau fractures: introduction of its utility and assessment of its reproducibility. J Trauma Acute Care Surg. 2012; 73:731–737.
[6] Kokkalis ZT, Iliopoulos ID, Pantazis C, Panagiotopoulos E. What's new in the management of complex tibial plateau fractures?. Injury. 2016; 47:1162–1169.
[7] Bowles RJ, Chadayammuri V, Baldini T, Brecevich A, Mauffrey C. Split depressed lateral tibial plateau fractures: a comparison of augmented percutaneous screws versus augmented plate and screw construct in a cadaveric model. J Orthop Trauma. 2018; 32:e270–e275.
[8] Burdin G. Arthroscopic management of tibial plateau fractures: surgical technique. Orthop Traumatol Surg Res. 2013; 99:S208–S218.
[9] Timmers TK, van der Ven DJ, de Vries LS, van Olden GD. Functional outcome after tibial plateau fracture osteosynthesis: a mean follow-up of 6 years. Knee. 2014; 21:1210–1215.
[10] Wang PC, Ren D, Zhou B. Surgical technique of anterolateral approach for tibial plateau fracture. Orthop Surg. 2015; 7:368–370.
[11] Hake ME, Goulet JA. Open reduction and internal fixation of the tibial plateau through the anterolateral approach. J Orthop Trauma. 2016; 30:S28–S29.
[12] Yoon YC, Oh JK, Oh CW, Sahu D, Hwang JH, et al. Inside out rafting K-wire technique for tibial plateau fractures. Arch Orthop Trauma Surg. 2012; 132:233–237.
[13] Cross WW, Levy BA, Morgan JA, Armitage BM, Cole PA. Periarticular raft constructs and fracture stability in split-depression tibial plateau fractures. Injury. 2013; 44:796–801.
[14] Cole P, Lafferty PM, Levy BA, Watson JT. Tibial plateau fractures. In: Browner B, Jupiter J, Krettek C. Skeletal Trauma: Basic Science, Management and Reconstruction. 5th ed. Philadelphia: Saunder/Elsevier; 2014; pp.1937–2015.
[15] Kulkarni SG, Tangirala R, Malve SP, Kulkarni MG, Kulkarni VS, et al. Use of a Raft Construct through a locking plate without bone grafting for split-depression tibial plateau fractures. J Orthop Surg. 2015; 23:331–335.
[16] Smith HJ, Richardson JB, Tennant A. Modification and validation of the Lysholm Knee Scale to assess articular cartilage damage. Osteoarthritis Cartilage. 2009; 17:53–58.
[17] Norris GR, Checketts JX, Scott JT, Vassar M, Norris BL, et al. Prevalence of deep surgical site infection after repair of periarticular knee fractures: a systematic review and meta-analysis. JAMA Netw Open. 2019; 2:e199951.
[18] Wasserstein D, Henry P, Paterson JM, Kreder HJ, Jenkinson R. Risk of total knee arthroplasty after operatively treated tibial plateau fracture: a matched population-based cohort study. J Bone Joint Surg Am. 2014; 96:144–1450.
[19] Mehin R, O’Brien P, Broekhuyse H, Blachut P, Guy P. Endstage arthritis following tibia plateau fractures: average 10-year follow-up. Can J Surg. 2012; 55:87–94.
[20] Parkkinen M, Madanat R, Mustonen A, Koskinen SK, Paavola M, et al. Factors predicting the development of early osteoarthritis following lateral tibial plateau fractures: mid-term clinical and radiographic outcomes of 73 operatively treated patients. Scand J Surg. 2014; 103:256–262.
[21] Wang Y, Luo C, Zhu Y, Zhai Q, Zhan Y, et al. Updated three-column concept in surgical treatment for tibial plateau fractures—a prospective cohort study of 287 patients. Injury. 2016; 47:1488–1496.
[22] Thamyongkit S, Abbasi P, Parks BG, Shafiq B, Hasenboehler EA. Weightbearing after combined medial and lateral plate fixation of AO/OTA 41-C2 bicondylar tibial plateau fractures: a biomechanical study. BMC Musculoskelet Disord. 2022; 23:86.
[23] Zhang Q, Zhao J, Zhang G, Tang J, Zhu W, et al. The comparison of clinical effect, knee function, prognosis of double plate fixation and locking plate internal fixation for tibial plateau fractures. Pak J Med Sci. 2022; 38:960–964.
[24] Chang H, Zhu Y, Zheng Z, Chen W, Zhao S, et al. Meta-analysis shows that highly comminuted bicondylar tibial plateau fractures treated by single lateral locking plate give similar outcomes as dual plate fixation. Int Orthop. 2016; 40:2129–2141.
[25] Vélez DAG, Headford M, Suresh KV, Liberatos PM, Bledsoe G, et al. Biomechanical analysis of dual versus lateral locked plating in elderly bicondylar tibial plateau fractures: Does medial comminution matter? Injury. 2022; 53:3109–3114.