Case Report
2015
September
Volume : 3
Issue : 3
Synchronous double malignancy: Acute lymphoblastic leukemia and carcinoma rectum
Meher Lakshmi Konatam, Triveni B, Sai Mallikarjun S, Sree Lakshmi S
Pdf Page Numbers :- 134-136
Meher Lakshmi Konatam1,*, Triveni B1, Sai Mallikarjun S1 and Sree Lakshmi S1
1MNJ Institute of Oncology and & Regional Cancer Centre, Red Hills, Lakadikapul, Hyderabad-500004, Telangana, India
*Corresponding author: Dr. Meher Lakshmi Konatam, Assistant Professor, MNJ Institute of Oncology and Regional Cancer Centre, Red Hills, Lakadikapul, Hyderabad-500004, Telangana, India. Tel.: 9440592569; Email: mehercancercare@gmail.com
Received 11 May 2015; Revised 13 June 2015; Accepted 26 June 2015; Published 30 June 2015
Citation: Meher Lakshmi K, Triveni B, Sai Mallikarjun S, Sree Lakshmi S. Synchronous double malignancy: Acute lymphoblastic leukemia and carcinoma rectum. J Med Sci Res. 2015; 3(3):134-136. DOI: http://dx.doi.org/10.17727/JMSR.2015/3-026
Copyright: © 2015 Meher Lakshmi K, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Synchronous double malignancy involving hematopoietic system and solid organs is rare. We report an interesting case of acute lymphoblastic leukemia (ALL) and carcinoma rectum. High index of suspicion is required in leukemic patients with bleeding per rectum to diagnose synchronous malignancy at an early stage.
Keywords: double malignancy; carcinoma rectum; acute lymphoblastic leukemia; synchronous malignancy
Full Text
The occurrence of second malignancy in a different organ in a known patient with malignancy is known as double malignancy. It is observed that a person with a malignant tumor may be more prone to develop another malignancy than would be expected by mere chance alone [1]. Certain criteria have been laid down to diagnose two separate malignant neoplasms [2], i.e., in order to make the diagnosis of a second primary malignant neoplasm, each tumor should be separate from the other, each should be malignant, and neither should be a metastasis from the other, i.e., microscopic and morphologic features of the two tumors must be entirely different.
Treatment strategies in case of double malignancy depend on treating the malignancy that is more advanced first, or sometimes both malignancies could be treated simultaneously if chemotherapeutic agent is the same. Double malignancy involving hematopoietic system and solid organs is very rare and there are hardly any case reports.
Due to several benign causes bleeding per rectum is common during induction therapy for ALL. Hence second malignancy is rarely suspected in such cases. We report a rare case with carcinoma rectum in a patient suffering from ALL.
Case report
A 55-year-old man presented with fever and fatigue of one month duration. Complete blood picture was suggestive of acute leukemia. Diagnosis of precursor B acute lymphoblastic leukemia was confirmed by flow cytometry on peripheral blood.
He was started on induction chemotherapy according to MCP 841 protocol. On day 16 of induction when the counts were low, he complained of bleeding per rectum while passing stools. It was a painless bleed along with stools. He developed febrile neutropenia on day 16. He was given supportive care with antibiotics, blood products and stool softening agents. Bone marrow done, at the completion of induction, was suggestive of marrow in remission. Bleeding continued despite recovery of blood counts.
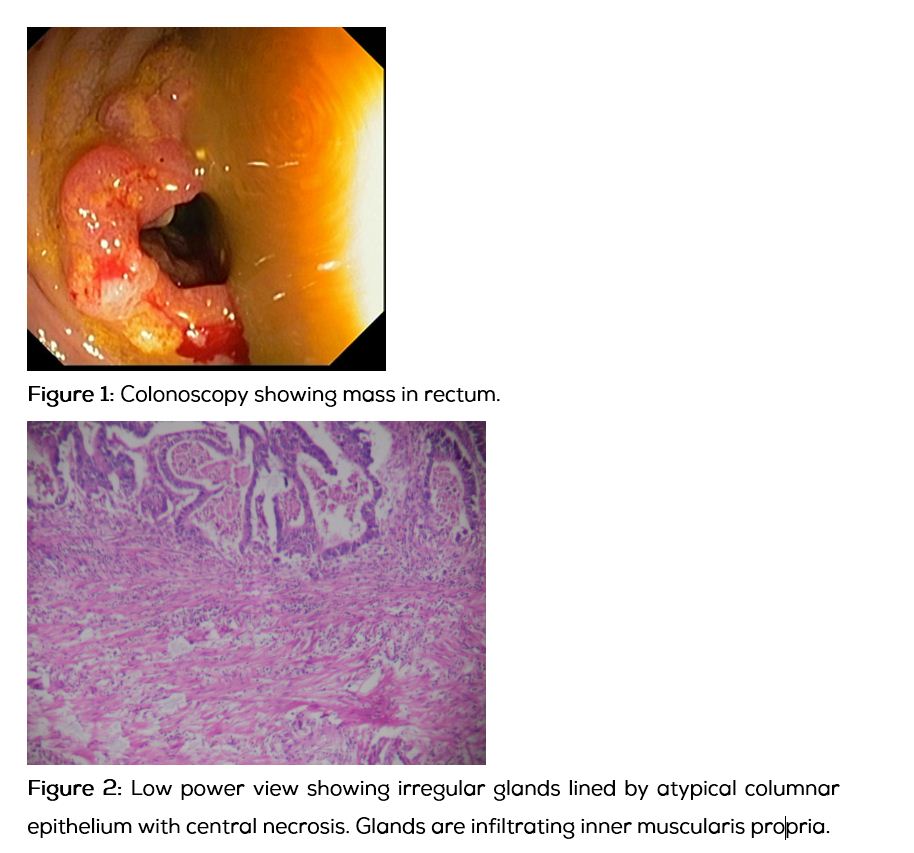
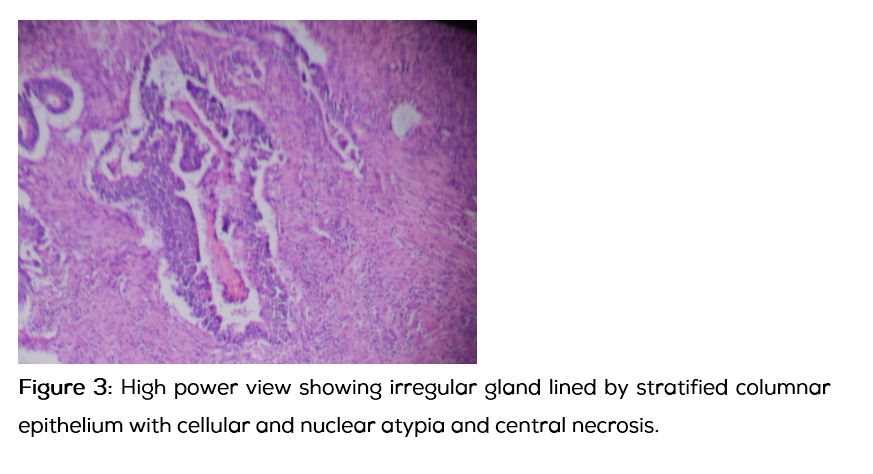
Gastroenterologist consultation was sought for bleeding per rectum. Colonoscopy showed mass in rectum (Figure 1). Biopsy was done which was suggestive of adenocarcinoma rectum. CECT abdomen showed mass confined to rectum with no visible nodes. Anterior resection was done. Postoperative HPE was suggestive of moderately differentiated adenocarcinoma, pT4N0M0 (Figures 2 and 3). Soon after recovery from surgery he was restarted on chemotherapy for ALL. Prior to the start of maintenance chemotherapy, he was given local RT with concurrent 5FU for carcinoma rectum. He is now in maintenance phase of chemotherapy for ALL and is doing well.
Discussion
Synchronous tumors have been described in literature. The hypothesis put forth for occurrence of these tumors is field cancerisation as in head and neck malignancies. Since Billroth published the first report of multiple primary malignancy in 1869, numerous reports of multiple carcinomas of large gut, arising simultaneously or as interval carcinomas, have been published [3].
Double malignancies involving multiple solid organs have been described. One case was reported from Japan, who was having synchronous adenocarcinoma of lung and malignant astrocytoma of brain following exposure to asbestos [4].
Other patients from India include those with squamous cell carcinoma of lung and rhabdomyosarcoma of scapula in a 90 year old male [5], double malignancies of breast and esophagus [6], bladder cancer and leiomyosarcoma [7]. A recent analysis from a cancer centre in India has reported 41 cases of multiple primary malignancies in a period of 4 years. But in their analysis also not a single case involving leukemia and solid organ is described [8].
Our case is rare as rectal malignancy is never suspected in leukemia patients during induction phase. During induction therapy of leukemias, rectal bleeding is common and the most common causes are haemorrhoids, fissure or infection. Bleeding is controlled in most of the patients with supportive care and almost all improve after recovery of blood counts. Rarely bleeding can be due to involvement of gastrointestinal tract. Gastrointestinal tract involvement is described in leukemia including ALL and chronic lymphocytic leukaemia (CLL) [9].
In this patient, continuing bleed even after recovery of blood counts and normal clinical examination led to suspicion and thus to colonoscopy. Though the bleed was not massive prudent clinical approach and the inquisitiveness to explore the cause of bleed led to the diagnosis of carcinoma rectum in early stage. Since leukemia is more aggressive malignancy amongst the two, therapy for leukemia was given priority and soon after completion of surgery the intensive phases of leukemia treatment were completed and the patient was then sent for radiotherapy for carcinoma rectum. Patient is now asymptomatic and stable.
Conclusions
Bleeding per rectum is due to various causes in patients undergoing induction chemotherapy for acute leukemia. Though carcinoma rectum is a rare cause of bleeding per rectum in patients undergoing induction chemotherapy, possibility of it must be borne in mind and colonoscopy must be considered if bleeding continues after recovery of blood counts.
Conflict of interest
The authors declare no conflict of interest.
References
1. Fauvet J, Chavy A, Piet R. Les Cancers primitifs multiples. Rev Prat. 1964; 14:2149–74.
2. David F, Mobley BA, Martinez J. Two histologically different primary carcinomas of the lung. Cancer. 1968; 22:287–292.
3. Billroth H, Die Allgemeire, Chirurgie. Pathologie-u-therapie p.908, R. Reimer, Berlin 1889. Quoted by Harry E.B. et al; Multiple primary malignant tumours involving the colon and rectum. Am J Surg. 1952; 55:83–85.
4. Kishimoto T, Hashimoto H, Ono T, Okada K. Synchronous double malignancy: Adenocarcinoma of lung and malignant astrocytoma induced by asbestos exposure. Cancer Invest. 1992; 10(2):129–133.
5. Masood I, Bhargava R, Ahmad Z, Sharma DK, Sherwani R. A case of double malignancy - Carcinoma lung and rhabdomyosarcoma in a 90 year old male. Journal Ind Acad of Cl Med. 2005; 6(2):167–170.
6. Singh A, Khare IC, Dixit AK, Pandey KC, Mittal DK, et al. Successfully treated synchronous double malignancy of the breast and esophagus: a case report. J Med Case Rep. 2010; 4:169.
7. Viveka BK, Amirtham U, Kumar VM, Babu GK. A case of synchronous double malignancy: Invasive bladder cancer and Leiomyosarcoma of extremity and review of literature. South Asian J Cancer. 2013; 2(3):152.
8. Bagri PK, Singh D, Singhal MK, Singh G, Mathur G, et al. Double primary malignancies: A clinical & pathological analysis report from a regional cancer institute in India. Iran J Cancer Prev. 2014; 7(2):66–72.
9. Kuse R, Lueb H. Gastrointestinal involvement in patients with chronic lymphocytic leukemia. Leukemia. 1997; 11 Suppl 2:S50–51.