Review
2015
March
Volume : 3
Issue : 1
Tarsal coalitions
Kakarla S
Pdf Page Numbers :- 43-46
Kakarla S1,*
1Chairman, KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India
*Corresponding author: Prof. Kakarla Subbarao, MS, D.Sc. (HON), FRCR, FACR, FICP, FSASMA, FCCP, FICR, FCGP, Chairman, KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India. Email: subbaraokakarla25@gmail.com
Received 21 October 2014; Revised 28 November 2014; Accepted 12 December 2014; Accepted 19 December 2014
Citation: Kakarla S. Tarsal coalitions. J Med Sci Res 2015; 3(1):43-46. DOI: http://dx.doi.org/10.17727/JMSR.2015/3-009
Copyright: © 2015 Kakarla Subbarao. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Abstract is not available for this article.
Full Text
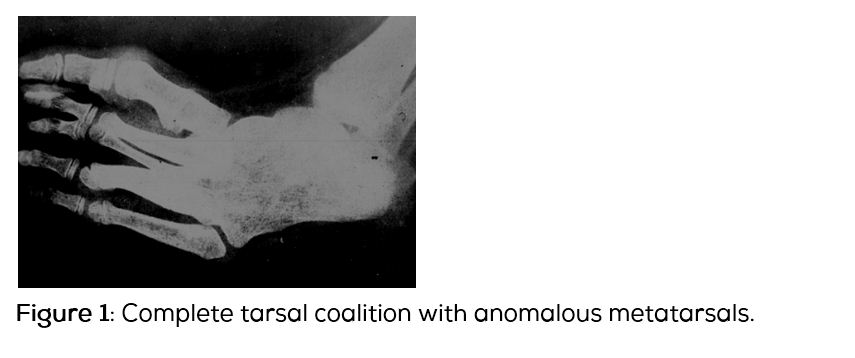
Tarsal coalitions are rare but not uncommon. It is an abnormal, congenital, connection of two or more tarsals in the foot. Total tarsal coalitions are extremely rare (Figure 1). Tarsal coalition may be present at birth, but may not show signs until early adolescence and late in life. It may result in a severe rigid flat foot. It is inherited as autosomal dominance with variable penetrance. The incidence may vary from 1-2%. However, the exact incidence is not known in Indian population.
Investigations and imaging findings
Two most common coalitions include calcaneo talar and calcaneo navicular, although other coalitions have been described. In 50% of the patients, these are bilateral. The bridge between the tarsal bones may be fibrous, cartilaginous or osseous. The investigations include conventional radiographs in A.P., oblique and lateral radiographs preferably weight bearing. To demonstrate complete osseous bridge computed tomography (CT) may be necessary. Magnetic resonance imaging (MRI) would certainly demonstrate all types of bridges.
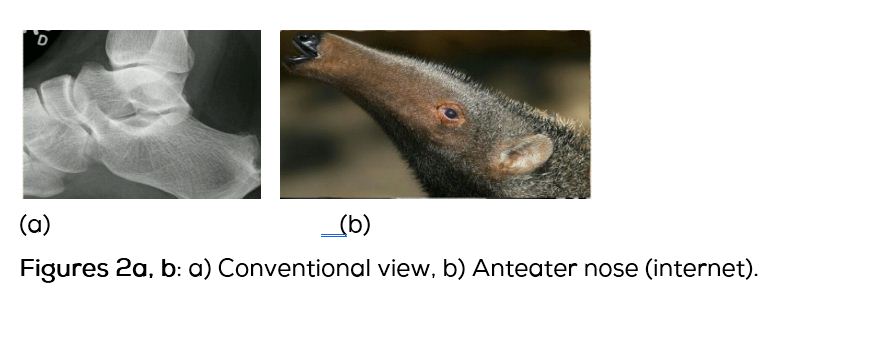
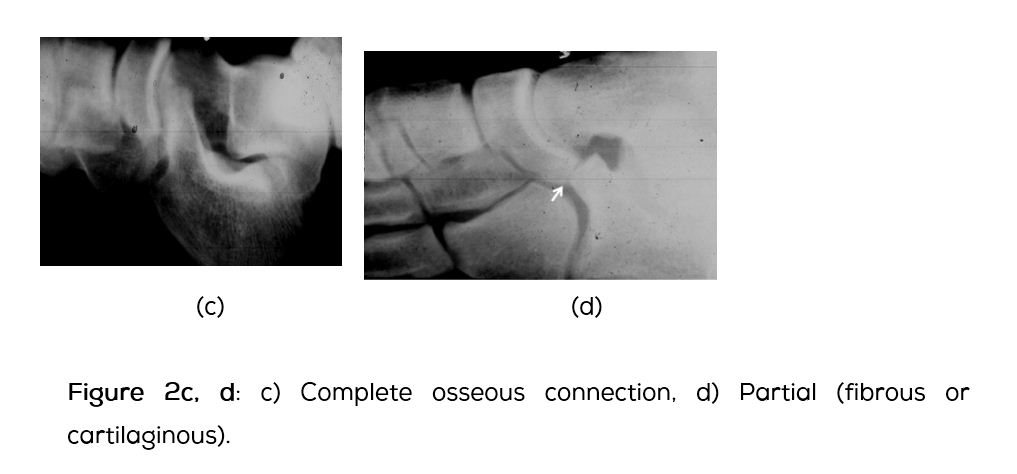
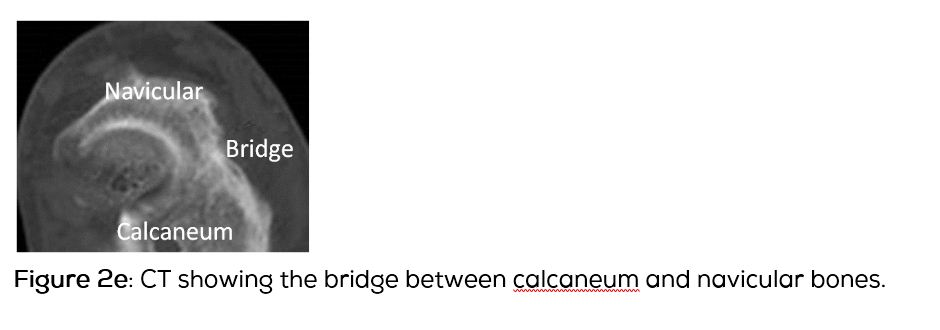
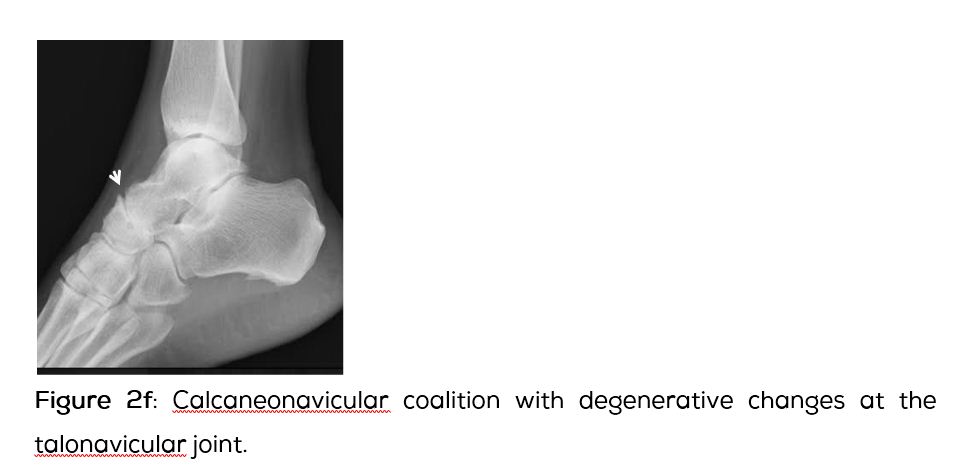
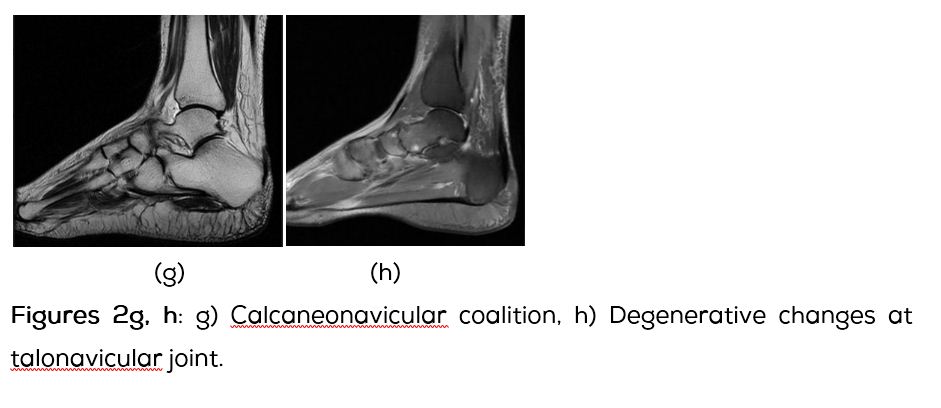
Calcaneonavicular coalitions amount to 45%. It involves the anterior process of calcaneum and is often named as “anteater nose sign”. This is better seen on conventional oblique views (Figures 2a, b). The coalition may be a complete bridge or segmented with a fibrous connection (Figures 2c, d). CT shows the complete osseous connection while MRI may show the cartilaginous portion (Figures 2e, f).
In chronic calcaneonavicular coalitions secondary changes in the talonavicular joint occur and show narrowing of the space with enthesopathy (Figure 2f). MRI may show edema of the adjacent bones (Figure 2g).
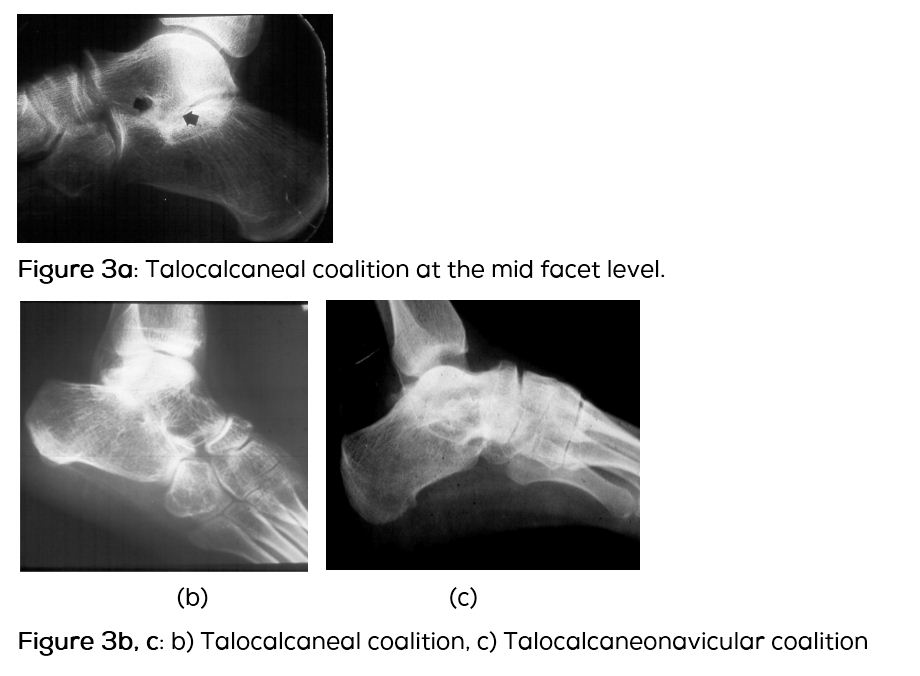
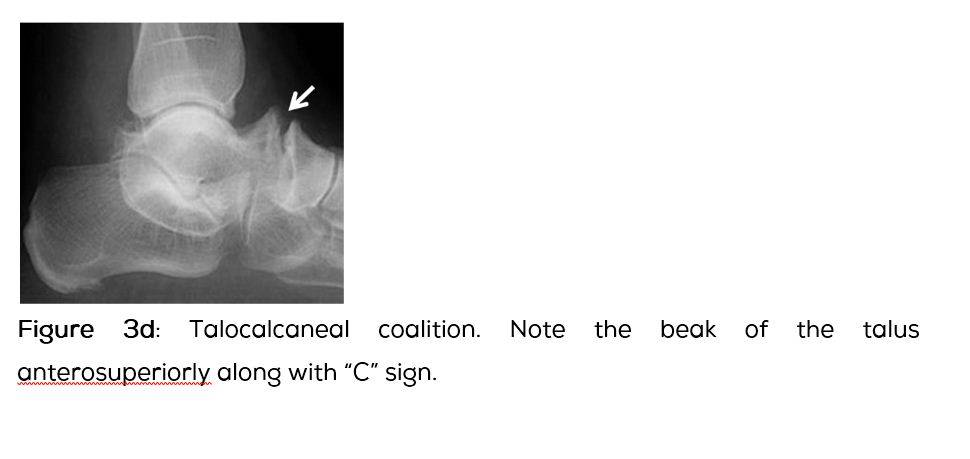
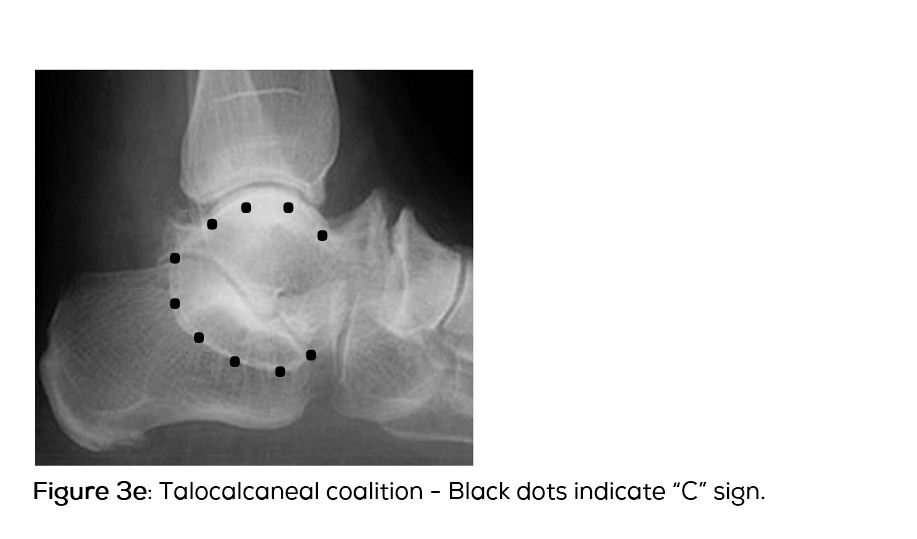
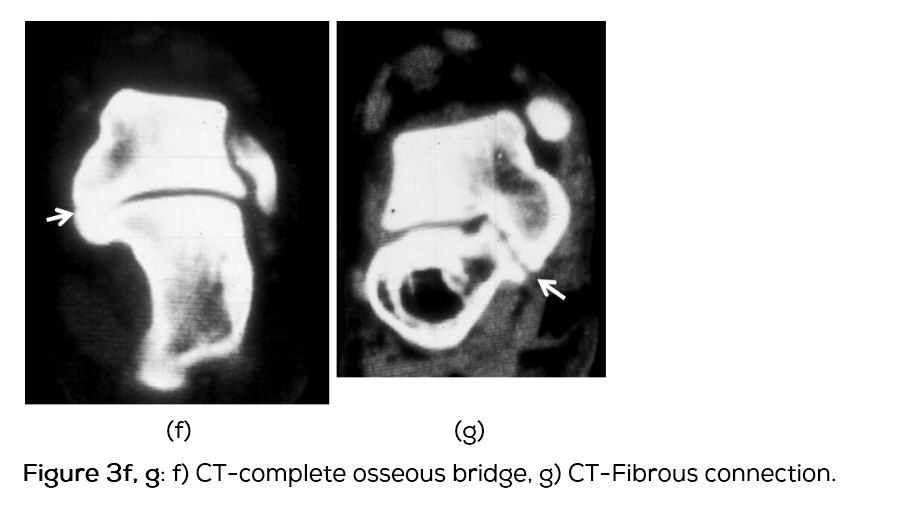
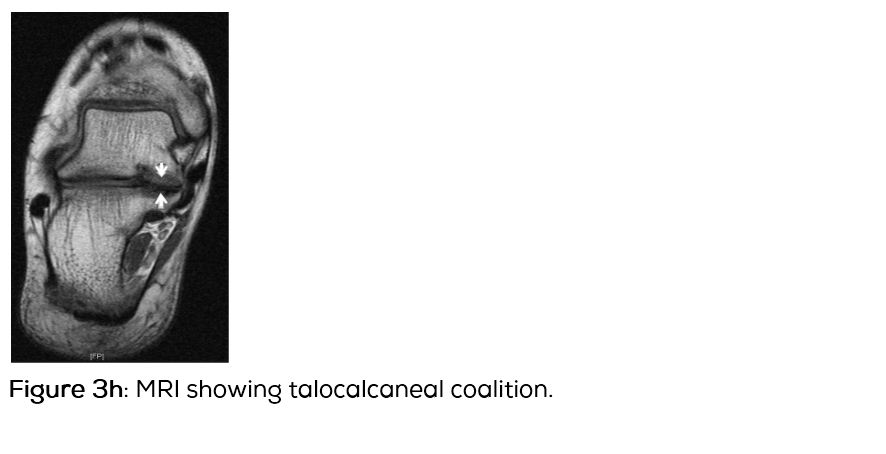
Talocalcaneal coalitions amount to another 45%. Involvement of the middle facet is common (Figure 3a). This is best seen on lateral views of the foot. Others include posterior and anterior joints (Figures 3b, c). Talar beak sign indicates impaired subtalar movements (Figure 3d). Another important finding is the “C” sign which constitutes complete posterior ring around talus and sustentaculum tali (Figure 3e). CT definitely demonstrates the osseous bar with bridging between talus and sustentaculum tali, particularly in axial view (Figures 3f, g). A sign called “drunken waiter’s” has been also described. Drunken waiter sign is based on the cranial height of the sustenaculum as well as how well formed the inner curve appeared. The dysplastic sustentaculum tali occurring with a subtalar coalition has been likened to a waiter having trouble carrying his tray (either an upturned or downturned hand and plate) while intoxicated, where the body of the calcaneus is considered the waiter and the sustentaculum tali is the tray. MRI is specific for non-osseous bars in fibrous bridge, irregularity and narrowing of bony articular margins are noted with associated sclerosis (Figure 3h). The cartilaginous bridge shows intermediate signal on T2. On stir images fluid signal with associated soft tissue and bone marrow edema are noted.
Conclusion
Tarsal coalitions are occasionally encountered with symptoms of pain in the foot. Most common coalitions are talocalcaneal and calcaneonavicular. Three types of bridges are described fibrous, cartilaginous and osseous. Conventional radiology is adequate to diagnose. However, CT and MRI eminently demonstrate the osseous and non-osseous bridges.
Acknowledgements
Acknowledgements are due to the Montefiore and Nizam's Institute of Medical Sciences.
Conflict of interest
The author declares no conflict of interest.
References
1. Brown RR, Rosenberg ZS, Thornhill BA. The C sign: more specific for flatfoot deformity than subtalar coalition. Skeletal Radiol. 2001; 30(2):84–87.
2. Crim JR and Kjeldsberg KM. Radiographic diagnosis of tarsal coalition. AJR Am J Roentgenol. 2004; 182: 323–328.
3. Nalaboff KM and Schweitzer ME. MRI of tarsal coalition: frequency, distribution, and innovative signs. Bull NYU Hosp Jt Dis. 2008; 66(1):14–21.
4. Lateur LM, Van Hoe LR, Van Ghillewe KV, Gryspeerdt SS, Baert AL, et al. Subtalar coalition: diagnosis with the C sign on lateral radiographs of the ankle. Radiology. 1994; 193(3):847–851.
5. Oestreich AE, Mize WA, Crawford AH, Morgan RC Jr. The "anteater nose": a direct sign of calcaneonavicular coalition on the lateral radiograph. J Pediatr Orthop. 1987; 7(6):709–711.
6. Resnick D. Talar ridges, osteophytes, and beaks: a radiologic commentary. Radiology. 1984; 151(2):329–332.