Case Report
2022
December
Volume : 10
Issue : 4
Testicular calcified parasitic mass masquerading as neoplasm
Kovuri U, Motrapu L
Pdf Page Numbers :- 251-252
Umadevi Kovuri1,* and Lavanya Motrapu1
1Department of Pathology, Government Medical College, Nizamabad, Telangana-503001, India
*Corresponding author: Dr. Umadevi Kovuri, Department of Pathology, Government Medical College, Nizamabad, Telangana 503001, India. Mobile: 7989330498; Email: dr.umadevik113@gmail.com
Received 12 July 2022; Revised 14 September 2022; Accepted 23 September 2022; Published 29 September 2022
Citation: Kovuri U, Motrapu L. Testicular calcified parasitic mass masquerading as neoplasm. J Med Sci Res. 2022; 10(4):251-252. DOI: http://dx.doi.org/10.17727/JMSR.2022/10-47
Copyright: © 2022 Kovuri U et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Endemic filariasis is very common in Uttar Pradesh, Bihar, Jharkhand, Odisha, Andhra Pradesh and Tamil Nadu. It’s occurrence in lymph node and lymphatic vessels is common, but rare in other sites and should always be reported. Testicular mass may be mistaken as malignancy. Here we report a case of 29-years-old male who presented with testicular swelling and diagnosed as pyocele clinically. Biopsy sent as low orchidectomy specimen showed filarial worm on histopathology.
Keywords: testicular filariasis; calcified concretions; orchidectomy
Full Text
Introduction
The term filariasis usually refers to lymphatic filariasis caused by Wuchereria bancrofti and Brugia malayi and mainly involves lymphatic system of the body [1, 2]. It is very rare to find filarial worm in testis. Here we report a case of testicular filariasis presented as a pyocele.
Case presentation
A 29-years-old year male hailing from Nizamabad presented with right testicular swelling to surgery department. There was a history of trauma three days back and swelling gradually increased in size. Clinically diagnosed as pyocele and right low orchidectomy was done and specimen sent to histopathology, Department of Pathology, Government General Hospital Nizamabad. Blood smear does not reveal peripheral eosinophilia. Figure 1 shows gross picture of specimen and globular mass measuring 6.8×3×3cm, firm to hard in consistency, external surface grey brown, cut section showed variegated appearance with grey white to grey brown areas and specks of calcified areas. Multiple sections were taken from testis. H and E stained multiple and serial sections studied from testis and paratesticular region showed large collections of inflammatory cells composed predominantly of lymphocytes, eosinophils and histiocytes (Figure 2 and Figure 3). Collection is predominantly around blood vessels and seminiferous tubules. Also localised area composed of cyst like space lined by homogeneous eosinophilic material with calcified concretions noted with surrounding granulomatous reaction composed predominantly of lymphocytes, eosinophils and histiocytes- possibility of calcified parasite, filarial worm was suggested.
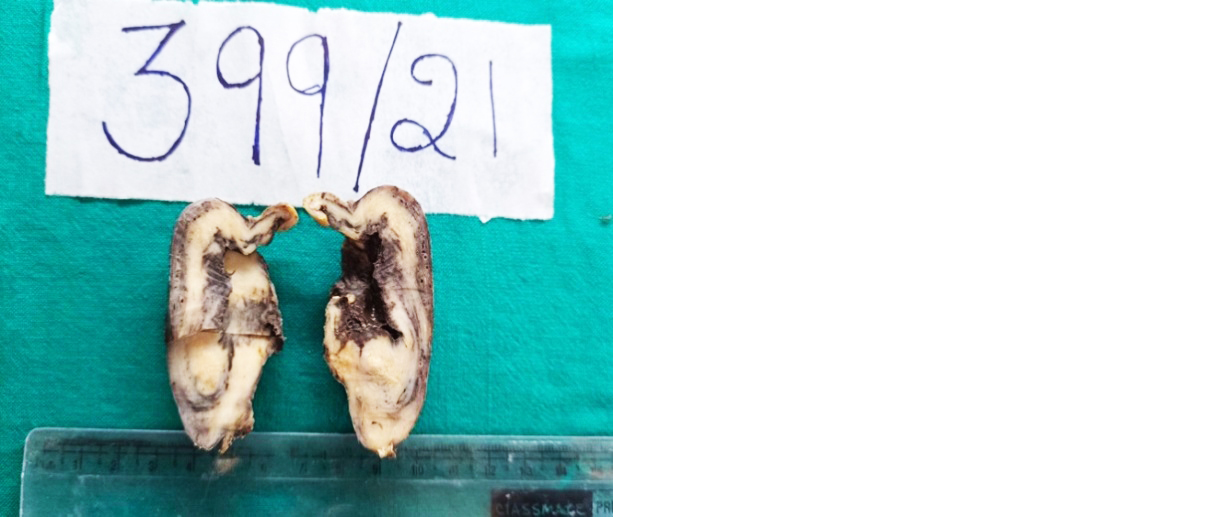
Figure 1: Cut section of testis showing variegated appearance with specks of calcification.
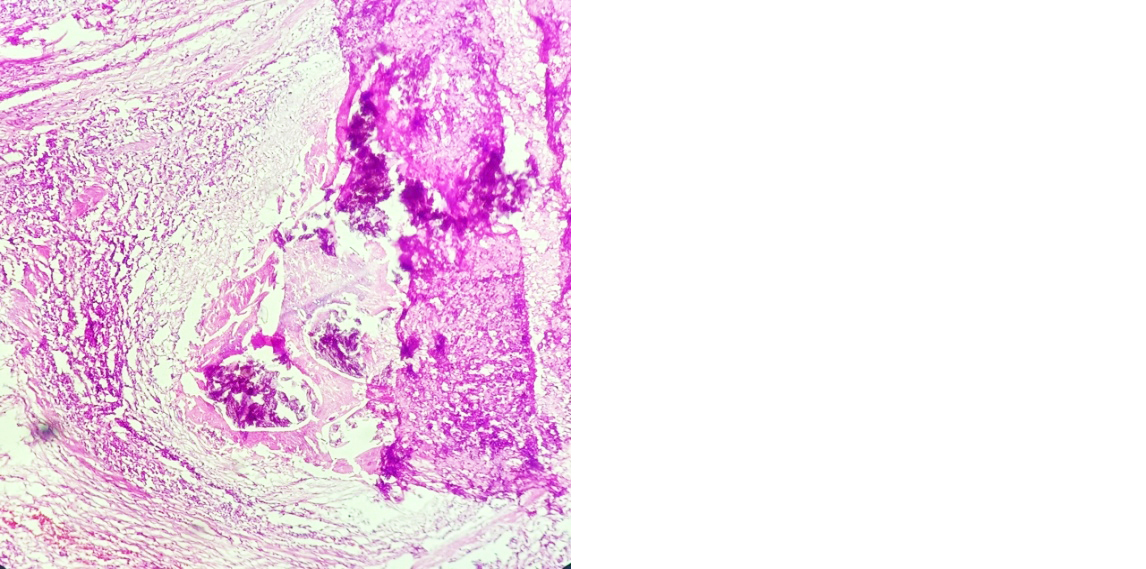
Figure 2: H &E cyst like space lined by homogeneous eosinophilic material with calcified concretions and collections of lymphocytes, eosinophils and histiocytes (10x).
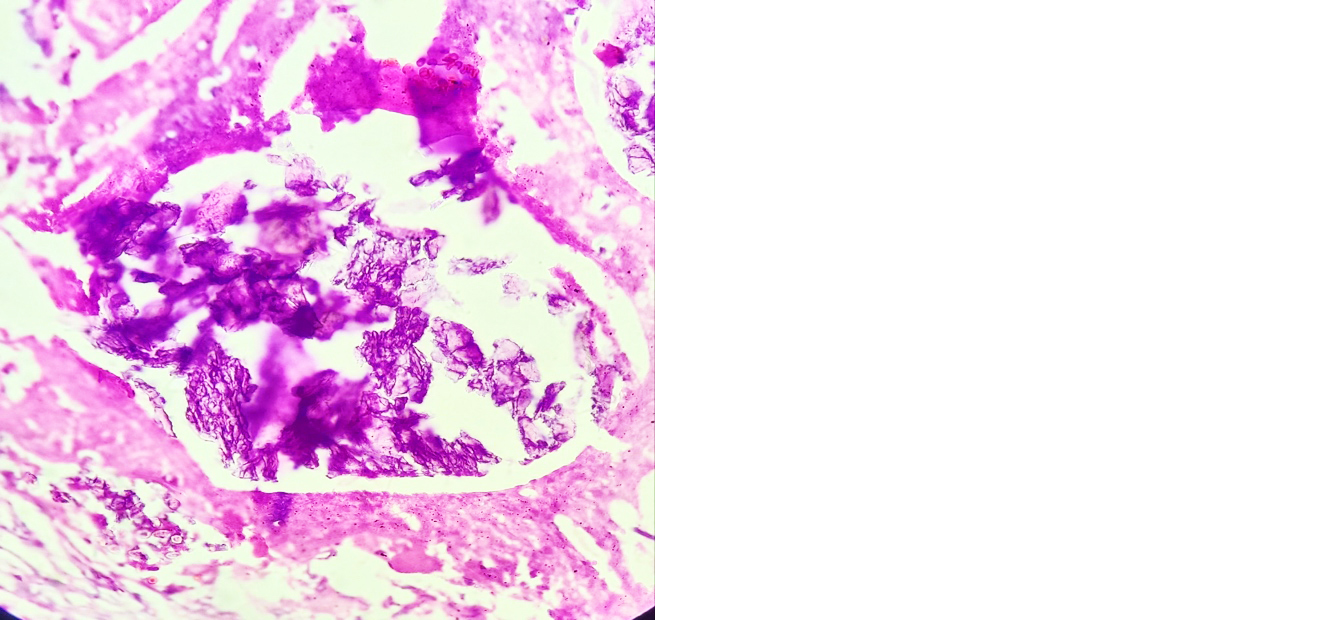
Figure 3: Eosinophilic material with calcified concretions (40x).
Discussion
Filariasis usually affects lymph nodes and lymphatic system. Culex, Aedes, Anopheles genera acts as intermediate hosts in transmission of W. bancrofti, B. malayi filariasis [1-3]. Filariasis affects male genitals especially lymphatics of the spermatic cord. Suppurative and granulomatous reaction induced by the dead filarial worm mimics neoplasm [4]. Filarial manifestation in male genitals include orchitis, filarial abscess, funiculoepidymitis, hydrocoele, lymphvarix, Filarial granuloma, chyluria, filarial penis, inguinal lymphadenitis, elephantiasis of genitalia or filarial granuloma [3-7]. Our case presented as painful mass in the testis, clinically thought to be pyocoele.
When a person acquires filarial infection during childhood, he may remain asymptomatic or it may progress to infect male genitalia [6, 8]. When we find eosinophils in any tissue it gives clue that person has parasitic or fungal infection. When we find more eosinophilic infiltrates in testis filariasis may be considered in differential diagnosis.
Microfilaria apart from lymph nodes and lymphatics can be found in lesions from breast mass, thyroid mass, pleural fluid, ascitic fluid, pericardial fluid, bronchial aspirates, urine, nipple secretion, joint fluid aspirates and hydrocoele fluid [9]. Adult worms had been found in subcutaneous tissue, peritoneal and pleural cavity, heart, brain, breast and scrotum [9]. Enzyme linked immunosorbent assay (ELISA) is considered as gold standard test for diagnosing filarial infection. Identifying microfilaria in peripheral blood midnight smear is necessary for diagnosis of filariasis [9].
On ultrasonography following diethylcarabamazine treatment, intrascrotal calcified deadworms can be seen as specks of calcification. Undulating movements of live adult worms can be seen as “filarial dance sign” [10, 11].
Conclusion
Filariasis responds very well to treatment if it is diagnosed early. Filarial orchitis can resemble neoplastic, non-neoplastic testicular and paratesticular leisons. Here we present this case to consider filarial infection as differential diagnosis when dealing with testicular swelling for accurate diagnosis, conservative management and evade unnecessary orchidectomy if possible.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Park KP. Textbook of preventive and social medicine. 22nd. Jabalpur: Banarsidas Bhanot; 2013; pp.245–251.
[2] Chatterjee KD. Textbook of parasitology, protozoology and helminthology in relation to clinical medicine. 20th ed. CBS publishers and distributors Ltd. New Delhi; India: 2009; pp.236–241.
[3] Barreto SG, Rodrigues J, Pinto RGW. Filarial granuloma of the testicular tunic mimicking a testicular neoplasm: a case report. J Med Case Repor. 2008; 2:321.
[4] Ranjan R, Choubey D, Kumar P, Besra RC, Sahu SS, et al., Filarial scrotal tumour. J Evol Med Dental Sci. 2003; 2(18):3171–3174.
[5] Garg PK, Bhatt S, Kashyap B, George A, Jain BK. Genital filariasis masquerading as testicular torsion: J Vector Borne Diseases. 2011; 48:119–121.
[6] Hindi SAL, Asghar M, Hassan AA. Epididymal filariasis in a child: Bahrain medical bulletin. 2003; 25:4.
[7] Joshi PM, Shivde SR, Mandolkar M. Testicular filariasis masquerading as a testicular tumor – Case report with review of literature. Int J Surgery. 2009; 23:1.
[8] Behera PK, Rath PK, Panda RR, Satpathy S, Sarkar BK. Adult filarial worm in the tissue section of a breast lump: GW Indian J Surg. 2009; 71(4):210–212.
[9] Basu A, Sistla SC, Verma SK, Jagdish S, Lymphadenovarix in the axilla – an unusual presentation of filariasis. Filaria Journal. 2006; 5:9.
[10] Reddy GS, Das LK, Pani SP. The preferential site of adult- Wuchereriabancrofti: an ultrasound study of male asymp- tomatic microfilaria carriers in Pondicherry, India. Natl Med J India. 2004; 17(4):195–196.
[11] Chaubal NG, Pradhan GM, Chaubal JN, Ramani SK. Dance of live adult filarial worms is a reliable sign of scrotal filarial infection. J Ultrasound Med. 2003; 22:765–769.