Orginal Research
2022
June
Volume : 10
Issue : 2
Factors affecting diabetes mellitus among rural geriatric population in Tigiria Block of Odisha: Findings from AHSETS study
Sethi S, Sethi S, Kshatri JS, Nayak RR, Pradhan PC, Bhoi T
Pdf Page Numbers :- 100-104
Sujata Sethi1,*, Somanath Sethi2, Jaya Singh Kshatri3, Rasmi Ranjan Nayak3, Purna Chandra Pradhan1 and Trilochan Bhoi3
1Department of Community Medicine, SLN Medical College and Hospital, Koraput- 764020, Odisha, India
2Department of Community Medicine, PRM Medical College and Hospital, Baripada, Odisha, India
3ICMR-Regional Medical Research Center, Bhubaneswar-751023, Odisha, India
*Corresponding author: Dr. Trilochan Bhoi, Research Assistant, ICMR-Regional Medical Research Center, Bhubaneswar-751023, Odisha, India. Mobile: +91 9040242560; Email: trilochanphysio@gmail.com
Received 18 January 2022; Revised 11 March 2022; Accepted 19 March 2022; Published 26 March 2022
Citation: Sethi S, Sethi S, Kshatri JS, Nayak RR, Pradhan PC, Bhoi T. Factors affecting diabetes mellitus among rural geriatric population in Tigiria Block of Odisha: Findings from AHSETS study. J Med Sci Res. 2022; 10(2):100-104. DOI: http://dx.doi.org/10.17727/JMSR.2022/10-19
Copyright: © 2022 Sethi S et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: In India, the population of elderly is predicted that it will be increased from 8% in 2015 to 19% in 2050. Geriatric population contributes around 9% of the total Odisha population and 86.3% of them reside in rural areas. The study aimed to estimate the prevalence of diabetes mellitus and find out its risk factors among rural geriatric population in Tigiria block of Odisha, India.
Methods: This was a community-based study, cross-sectional in design among 725 rural geriatric populations of Odisha. Socio-demographic information was collected following the standard census of India operational definitions. Self-reported diabetes mellitus status was collected and classified as "present" or "absent". Statistical analysis was performed using "R version 4.0.4".
Results: Among the total elderly, 88 (12.13%) participants were diagnosed with diabetes. Common factors found to be significant with diabetes were illiterates (AOR=0.32, CI=0.125-0.817), not working elderly (AOR=2.51, CI=1.103-5.723), high socioeconomic status (AOR=3.79, CI=1.351-10.632) and overweight elderly (AOR=2.19, CI=1.286-3.753) respectively.
Conclusion: The frequency of diabetes mellitus among rural geriatric population is less but the risk is high among those not working, literate, with higher SES and overweight elderly group. The researcher should emphasize real-time diagnosis of blood sugar levels using standardized measures among the rural elderly population.
Keywords: diabetes mellitus; geriatric population; rural; Odisha
Full Text
Introduction
India is a rural-based country where 65% of the total population resides in rural areas and it is predicted that in 2050, population will be equally distributed between rural and urban areas [1]. The population of elderly is predicted that it will be increased from 8% in 2015 to 19% in 2050. Geriatric population contributes around 9% of the total Odisha population and 86.3% of them reside in rural areas [2].
As lifespan is increasing, it will increase the opportunity to carry out many activities for themselves and also for the family and society, but it also impacts negatively due to the physical and psychological abnormality [3]. Among the rural elderly people the common disorders found are such as musculoskeletal disorders (osteoarthritis, joint pain), hypertension (HTN), cataract, depression, diabetes mellitus, and hearing problems [4–6].
Diabetes is a chronic metabolic disease manifested by elevated blood glucose levels. Diabetes leads to many serious complications over time. In the past 30 years, the prevalence of diabetes has raised in all income group countries. Affordability to treatment is critical to survival for those who are living with diabetes. About 422 million people are living with diabetes globally and larger sections of diabetic population are from low-and middle-income group countries. Diabetes contributes to about 1.6 million premature deaths yearly worldwide. The prevalence of diabetes has been rising rapidly in LMICs. The prevalence of diabetes is nearly 6% in India, 6.1% in men and 6.5% in women in all age groups. Diabetes is the major cause of kidney failure, stroke, blindness, heart attack and lower limb amputation. Diabetes contributed 5% increase in premature deaths between 2000 and 2016 and 1.5 million premature deaths in 2019 [7–9].
The study aimed to estimate the prevalence of diabetes among rural elderly population in Tigira block, Cuttack district of Odisha, and find the different determinants of diabetes among rural elderly population in Tigira block, Cuttack district of Odisha.
Methodology
Study design and setting
This cross-sectional study was carried out in the rural block of Tigiria in Cuttack district, Odisha, India, between June 2019 and February 2020. Tigiria is an administrative block of Odisha, India, consisting of 52 revenue villages with a total population of 74639 as per Census 2011 [10]. In Tigiria, there is Model Rural Health Research Unit (MRHRU) of the host institute (ICMR-RMRC, Bhubaneswar) which is the field site for community and implementation research. The study participants were residents of Tigiria block, Cuttack aged over 60 years who were conversant, comprehensible and provided their written informed consent to participate. Seriously ill, bedridden patients as well as those with severe cognitive impairment were excluded from the study.
Sample size and sampling
Assuming the prevalence of multimorbidity among elderly as 20%, which is our primary research question of the AHSETS Study (Assessment of Health Status of the Elderly in Tigiria block: a Syndemic approach), with 95% confidence level and width of confidence interval at 8%, beta of 0.20 and alpha of 0.05, the minimum sample size was calculated to be 407 [11]. Assuming a design effect of 1.6 due to clustering and a non-response rate of 10%, the sample size required was rounded off to 725. Participants were selected using a cluster sampling technique from a list of 30 clusters (revenue villages) selected based on a Probability Proportional to Size (PPS) method. Systematic random sampling method was used in each of the clusters for identification of study households, and all eligible participants from the selected household were recruited for the study. This was done until the necessary cluster size of 25 was attained. Immediate neighboring household was approached if the selected household failed to meet the eligibility criteria.
Data collection
Data were collected by trained field investigators using a pre-tested tool based on Open Data Kit (ODK) software installed on android tablets. Previous medical history of diabetes diagnosed by a medical professional was taken as positive for diabetes. Standard census of India operational definitions was followed to collect socio-demographic information. Current socioeconomic status (SES) of the participants was classified using the BG Prasad SES scale. Information on their personal habits such as smoking, chewing tobacco, and alcohol consumption behavior was collected.
Quality control
Data collection was commenced after a comprehensive training of the study staff using a standardized manual of operating procedures (MOP) for the study. To reduce entry errors, tablets were used to collect data. Periodic verification of the data was done by the investigators by checking for its completeness, duplications and range errors.
Statistical analysis
Frequencies and proportions were used as descriptive measures for categorical variables and mean with standard deviation for continuous variables. Bivariate analysis was done using the chi-square test. The binary logistic regression model was used to find out the predictors of diabetes.
Ethical considerations
Ethical approval was obtained from the institutional human ethics committee of ICMR-RMRC Bhubaneswar (Approval No- ICMR-RMRCB/IHEC-2019/022). Written informed consent was obtained from all participants and the national ethical guidelines for biomedical research were followed [12].
Results
This cross-sectional study was carried out among 725 rural elderly (>60 years) people in the Cuttack district of Odisha, in which 52.1% were male and the rests were female. Mean age of the study participants had found to be 70.24 years (SD=8.37 years). Among the total elderly, 88 (12.13%) participants were diagnosed with diabetes. Socio-demographic features of the study participants along with the prevalence of diabetes were tabulated (Table 1). 63.9% of the rural elderly were from 60-69 years age group while most of them were illiterates. Prevalence of diabetes among various age groups was presented in Figure 1. In comparison to females, males were more prevalent to have diabetes while more educated more was the diabetes prevalence. Common factors found to be statistically associated with diabetes were gender, education and SES.
Table 1: Socio-demographic characteristics of the study population.
|
|
Diabetes
|
P value
|
|
No
N (%)
|
Yes
N (%)
|
Total
N (%)
|
|
Age group (Years)
|
> 80
|
84
92.3%
|
7
7.7%
|
91
12.6%
|
0.371
|
|
70-79
|
150
87.7%
|
21
12.3%
|
171
23.6%
|
|
60-69
|
403
87.0%
|
60
13.0%
|
463
63.9%
|
|
Sex
|
Male
|
323
85.4%
|
55
14.6%
|
378
52.1%
|
0.037*
|
|
Female
|
314
90.5%
|
33
9.5%
|
347
47.9%
|
|
Education
|
No Education
|
320
92.5%
|
26
7.5%
|
346
47.7%
|
<0.001*
|
|
Primary School
|
261
86.7%
|
40
13.3%
|
301
41.5%
|
|
Secondary School
|
30
78.9%
|
8
21.1%
|
38
5.2%
|
|
High School & Above
|
26
65.0%
|
14
35.0%
|
40
5.5%
|
|
Occupation
|
Not Working
|
496
87.5%
|
71
12.5%
|
567
78.2%
|
0.443
|
|
Laborer
|
46
85.2%
|
8
14.8%
|
54
7.4%
|
|
Agriculture
|
95
91.3%
|
9
8.7%
|
104
14.3%
|
|
SES
|
Poor
|
347
89.2%
|
42
10.8%
|
389
53.7%
|
<0.001*
|
|
Lower-middle
|
192
88.5%
|
25
11.5%
|
217
29.9%
|
|
Upper-middle
|
83
88.3%
|
11
11.7%
|
94
13.0%
|
|
High
|
15
60.0%
|
10
40.0%
|
25
3.4%
|
|
*Statistically significant at alpha ≤0.05 level
|
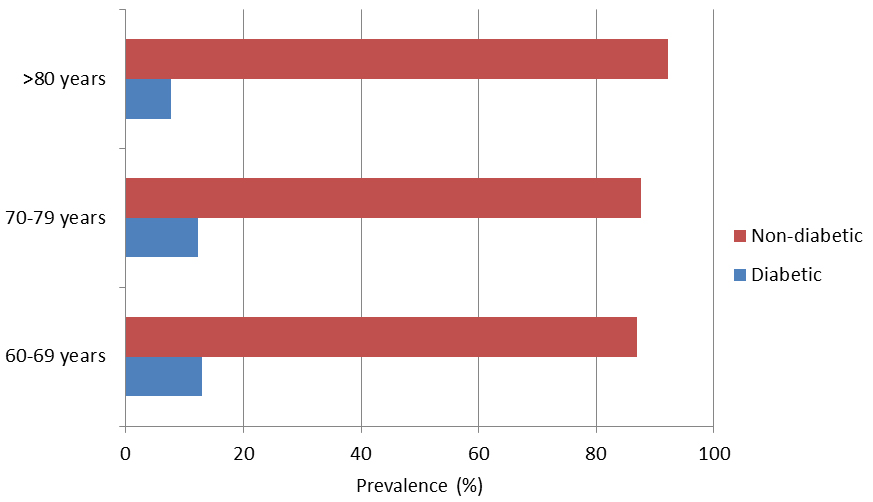
Figure 1: Prevalence of diabetes mellitus among age group.
The logistic regression model was run to find out the predictors of diabetes among the rural elderly population (Table 2). Common factors found to be significant with diabetes were illiterates (AOR=0.32), not working elderly (AOR=2.51), high socioeconomic status (AOR=3.79) and overweight elderly (AOR=2.19) respectively.
Table 2: Logistic regression model for diabetes.
|
Attributes
|
Diabetes, odds ratio (95% CI)
|
|
Male gender
|
1.162 (0.898, 2.938)
|
|
Age group (Years)
|
|
>80
|
0.540 (0.220, 1.324)
|
|
70-79
|
0.871 (0.477, 1.589)
|
|
60-69
|
Ref
|
|
Education
|
|
Illiterate
|
0.320* (0.125, 0.817)
|
|
Primary
|
0.565 (0.240, 1.328)
|
|
Secondary
|
0.868 (0.288, 2.620)
|
|
High School &Above
|
Ref
|
|
Occupation
|
|
Not working
|
2.513* (1.103, 5.723)
|
|
Laborer
|
2.036 (0.692, 5.989)
|
|
Agriculture
|
Ref
|
|
Family type
|
|
Single
|
0.758 (0.259, 2.219)
|
|
Nuclear
|
1.450 (0.865, 2.431)
|
|
Joint
|
Ref
|
|
SES
|
|
High
|
3.791* (1.351, 10.632)
|
|
Upper-Middle
|
0.846 (0.846, 0.391)
|
|
Lower-Middle
|
0.972 (0.552, 1.713)
|
|
Low
|
Ref
|
|
Smoking
|
0.454 (0.178, 1.160)
|
|
Smokeless tobacco
|
1.190 (0.711, 1.993)
|
|
Alcohol
|
0.450 (0.098, 2.049)
|
|
BMI
|
|
Overweight
|
2.197* (1.286, 3.753)
|
|
Underweight
|
0.488 (0.168, 1.416)
|
|
Normal
|
Ref
|
|
*Statistically significant at alpha ≤0.05 level
|
Discussion
The rural elderly population in the Tigira block of Odisha had shown a prevalence of 12.13% for diabetes. The prevalence of diabetes among rural elderly in Uttarakhand and UP was found to be 14.6% and 23.95% respectively [13, 14]. Among the rural adults in different parts of India, the prevalence ranges from 9% in Maharashtra to 37.33% in South India whereas prediabetes ranges from 8.5% to 11.5% in South India [15–19]. The difference in diabetes status among the rural elderly might be due to social and cultural differences. Among the urban geriatric population, the prevalence was found to be 15.7% and 45.3% in Chandigarh and Punjab [20, 21]. The prevalence is high in comparison to the rural elderly which might be affected due to the lifestyle of the urban population. There is cultural variation throughout the different region in India, which also affect their health status including the risk of diabetes.
The factors such as high SES group (OR=3.791, 95%CI=1.351-10.632), not working elderly (OR=2.513, 95%CI=1.103-5.723), and overweight (OR=2.197, 95%CI=1.286-3.753) was found to be predictors of diabetes among the rural population. Illiteracy (OR=0.32, 95%CI=0.125-0.817) was inversely affecting diabetes. A similar study among rural elderly in Uttarakhand found the factors such as higher education level and higher BMI as predictors of diabetes [13]. Among the rural adults the factors such as older age (OR=2.17), male gender (OR=2.34), BMI >23 (OR=2.13), WHR >0.8 (OR=2.28), alcohol intake (OR=2.45), systolic BP >140mmHg (OR=2.15), and family history were found to be predictors of diabetes [16, 17]. The predictors of diabetes among urban adults were found to be female gender, age>50years, hypertension, family history of diabetes, family history of hypertension, non-vegetarian diet, BMI>23, and waist circumference>80cm [20, 21]. Apart from the risk factors, some socio-demographic factors were found to be associated with diabetes status such as gender (p=0.037), education (p<0.001), and SES (p<0.001). Among the Indian rural adults, factors such as age, literacy, occupation, physical activity, tobacco use, alcoholism, family history, BMI, WHR, HTN, TC, TGL, HDL, LDL, and hypertension were found to be significantly associated with diabetes status [15, 18, 19, 22].
The risk factors are more when including adults and urban population which is due to the change in lifestyle and working pattern of the relevant population. Diabetes is primarily driven by dietary transitions, with a lack of or insufficient physical activity further leading to obesity and overweight. Most of the people living in rural areas like Tigiria block are farmers and laborers with high physical work whereas, in urban, people have a sedentary lifestyle which increases the risk of diabetes among them. Other than that consumption of junk food in urban areas affects the health status.
Limitations
Self-reported disease status was obtained instead of a standardized method to diagnose blood sugar levels of the participants. Also, this study was limited to rural people of a single block of Odisha, India. Interpretation and generalization of the results from this study need to be carefully made.
Conclusion
The frequency of diabetes mellitus among rural geriatric population is less but the risk is high among those not working, literate, with higher SES and overweight elderly group. The diabetes prevalence may be showing less because the disease status is self-reported as per the previous diagnosis; it means the prevalence might show high if the current blood sugar level is measured. The researcher should emphasize real-time diagnosis of blood sugar levels using standardized measures among the rural elderly population. The strategies should be implemented at the grass-root level for health education, prevention, early detection, prompt management and to reduce complications of this public health problem.
Acknowledgments
We appreciate the support of the MRHRU team, MRHRU, Tigiria, Cuttack. I thank Matrujyoti Pattnaik (MPH) and Dr. Asit Mansingh (MPH) for their expertise and assistance in questionnaire preparation, installing ODK software, and using it for data collection. Funding Intramural funds from the Indian Council of Medical Research’s Regional Medical Research Centre were utilized for the study.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] India population - Worldometer. Accessed on 4 Jun 2020 from: https://www.worldometers.info/world-population/india-population/
[2] Giridhar G, James KS. Caring for our elders: Early responses. 55 Lodi Estate, New Delhi; 2017.
[3] Bate J, Rasmussen E. Ageing and Health. WHO. 2018; pp.2–3.
[4] Tiwari S, Sinha AK, Patwardhan K, Gehlot S, Gambhir IS, et al. Prevalence of health problems among elderly . Indian J Prev Soc Med. 2010; 41(3 and 4):229.
[5] Kumar D, Shankar H. Prevalence of chronic diseases and quality of life among elderly people of rural Varanasi. Int J Contemp Med Res. 2018; 5(7):G2.
[6] Kamble SV, Professor A, Ghodke YD, Professor A, Dhumale GB, et al. health status of elderly persons in rural area of India. Ind Med Gaz. 2012; (12):297.
[7] Akhtar S, Dhillon P. Prevalence of diagnosed diabetes and associated risk factors: Evidence from the large-scale surveys in India. J Soc Heal Diabetes. 2017; 5(1):28–36.
[8] Geldsetzer P, Manne-Goehler J, Theilmann M, Davies JI, Awasthi A, et al. Diabetes and Hypertension in India: A Nationally Representative Study of 1.3 Million Adults. JAMA Intern Med. 2018; 178(3):363–72.
[9] Corsi DJ, Subramanian SV. Socioeconomic Gradients and Distribution of Diabetes, Hypertension, and Obesity in India. JAMA Netw Open. 2019; 2(4):e190411.
[10] Tigiria block population, religion, caste cuttack district, Odisha - Census India. Available from: https://www.censusindia.co.in/subdistrict/tigiria-block-cuttack-odisha-2949.
[11] Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing clinical research: an epidemiologic approach, 2nd Ed. Vol. 78, Optometry and Vision Science. 2001; pp.81.
[12] Mathur R (editor). Handbook on National Ethical Guidelines for Biomedical and Health Research Involving Human Participants. New Delhi: Director General, Indian Council of Medical Research. 2018; pp.1–16.
[13] Kapil U, Khandelwal R, Ramakrishnan L, Khenduja P, Gupta A, et al. Prevalence of hypertension, diabetes, and associated risk factors among geriatric population living in a high-altitude region of rural Uttarakhand, India. J Fam Med Prim Care. 2018; 7(6):1527–1536.
[14] Agrawal N, Kumar P, Singh AK, Gupta SB. Prevalence of diabetes and associated risk factors in elderly rural population. Int J Curr Microbiol Appl Sci. 2020; 9(7):1642–1650.
[15] Agrawal V, Kshirsagar A, Patil V. Risk factors of type 2 diabetes mellitus in rural population of Karad, Maharashtra, India: an observational study. Int J Adv Med. 2019; 6(5):1584–1588.
[16] Bhalerao SD, Somannavar M, Goudar SS. Prevalence of type 2 diabetes mellitus in rural population of north Karnataka - A community based cross sectional study. Biomed. 2014; 3(1):2278–5221.
[17] Muthunarayanan L, Ramraj B, Russel J. Prevalence of prediabetes and its associated risk factors among rural adults in Tamil Nadu. Arch Med Heal Sci. 2015; 3(2):178–184.
[18] Padmanabha UR, Nalam U, Badiger S, Nagarajaiah P. Prevalence and risk factors of type 2 diabetes mellitus in the rural population of Mangalore, South India. Natl J Community Med. 2017; 8(8):456–461.
[19] Sethuram K, Uma MA, Rao S. A Study of prevalence of diabetes mellitus, prediabetes and cardio metabolic profile among rural population in south India. Int J Contemp Med Res. 2019; 6(3):C4–9.
[20] Ravikumar P, Bhansali A, Ravikiran M, Bhansali S, Walia R, et al. Prevalence and risk factors of diabetes in a community-based study in North India: the Chandigarh Urban Diabetes Study (CUDS). Diabetes Metab. 2011; 37(3):216–221.
[21] Arora I, Singh S, Bhuwal PK, Singh S. Prevalence of diabetes mellitus and its associated risk factor assessment among elderly in urban area of Punjab. Int J Community Med Public Heal. 2019; 6(2):610–614.
[22] Kumar KN, Katkuri S, Ramyacharitha I. A study to assess prevalence of diabetes mellitus and its associated risk factors among adult residents of rural Khammam. Int J Community Med Public Heal. 2018; 5(4):1360–1365.