Full Text
Introduction
Hand is the distal functional tool of the upper limb, an important organ for day-to-day functions. Hand anatomy is complex and intricate. This enables hands to do gross as well as precise functions. A total of 27 bones constitute the basic skeleton of the wrist and hand [8 carpals, 5 metacarpals, 14 phalanges and 3 for each digit except thumb which has 2]. The classification of benign tumors occurring in the bones of the hands is mentioned in Table 1.
Table 1: Classification of benign tumors.
|
Benign tumors
- Osseous
- Cartilaginous
- Fibrous
- Vascular
- Miscellaneous – Giant cell tumors, epidermoid cyst, aneurysmal bone cyst etc.,
|
Discussion with radiological characteristics
Conventional radiography plays a major role in the diagnosis of tumors of the bones of the hand. Benign tumors of the bones of the hands are more frequent than malignant lesions [1]. As with any bone tumor in any part of the body, it is critical to know the precise location of the tumor as well as the age of the patient to narrow the differential diagnosis. Also, the margin of the lesion and the zone of transition between the lesion and normal bone are key factors in determining the aggressiveness of the lesion. A lesion with well-defined, sharp margins on radiographs or CT images is considered nonaggressive, whereas a broad zone of transition and poorly defined borders suggest an infiltrative osseous process, such as an aggressive tumor or a destructive metabolic or infectious process. Mineralization and opacity of a lesion can be appreciated at radiography, although they are better characterized with CT, and can help determine the origin of the lesion. Identification of a matrix with a “rings-and-arcs” appearance indicates a chondral origin (e.g., enchondroma or chondrosarcoma). On the other hand, an opaque, cloud-like matrix is suggestive of osseous mineralization (osteoblastoma). The presence and the type of periosteal reaction can also help in the differential diagnosis. In general, periosteal reaction is uncommon in most of the benign tumors. A smooth, solid-appearing periosteal reaction denotes a slow, nonaggressive process and a disrupted or “sunburst” appearance suggests an aggressive lesion [2-4]. More aggressive indicate malignant tumors [5]. Presence of soft tissue swelling without mineralization does not help in arriving at the diagnosis. However, mineralization either cartilaginous or osseous would determine the nature of the lesion.
Imaging characteristics - Osseous tumors
- Osteoma
- Osteoid osteoma
- Osteoblastoma
Osteoma: This lesion is more common in skull bones and paranasal sinuses. However, osteoma can be encountered in the bones of the hand also. The imaging appearance is the same as is encountered in the skull. It is an uniformly dense structure attached to the cortex (Figure 1). A bone island should be distinguished as the latter is located in the medulla (Figure 2).

Figure 1: Osteoma of the proximal phalanx.
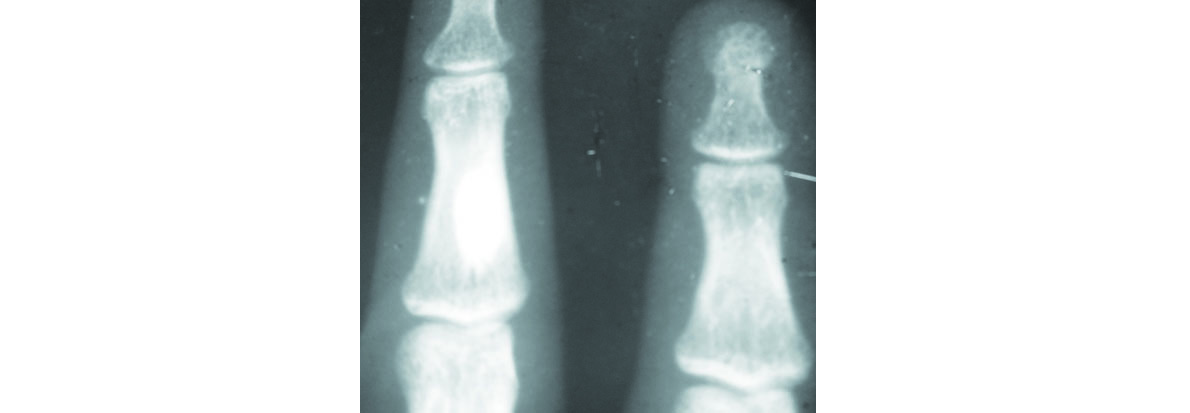
Figure 2: Bone island in the middle phalanx.
Osteoid osteoma: It may be intra cortical, periosteal, intramedullary or subarticular. Intracortical osteoid osteoma is a round lucent lesion with a nidus (Figure 3). Intense new bone formation is noted in both cortical and periosteal lesions. Associated soft tissue swelling is present. Intramedullary lesion does not usually produce reactive new bone. Subarticular lesion produces synovitis simulating arthritis without any periosteal reaction.
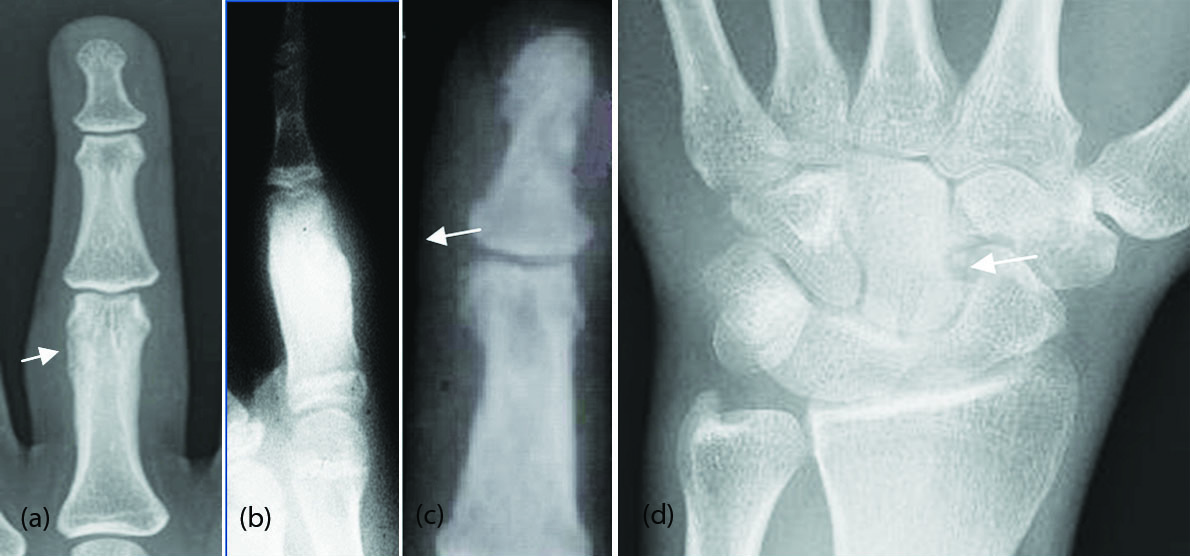
Figure 3: Osteoid osteoma with a sclerotic nidus; (a) proximal phalanx of middle finger, (b) index finger, (c) distal phalanx, (d) Osteoid osteoma of capitate bone.
Osteoblastoma: A benign osteoid producing tumor similar to osteoid osteoma but has a larger nidus. Moderate degree of new bone formation is also present (Figure 4a,b). Morphologically, it may simulate a large osteoid osteoma, aneurysmal bone cyst and when aggressive, an osteosarcoma.

Figure 4: (a) Osteoblastoma of proximal phalanx of index finger; (b) Osteoblastoma of the hamate bone.
Cartilaginous tumors
- Enchondroma
- Enchondroma protuberans
- Periosteal chondroma
- Exostosis – Single, multiple
- Ollier’s enchondromatosis
- Chondromyxoid fibroma
- Chondroblastoma
- Trevor’s
Enchondroma: It is a benign expanding cartilaginous neoplasm that is usually solitary in intramedullary bone. The typical rings and arcs of calcification may not be present all the time. However, punctuate or micro nodular calcification may be seen sometimes [6]. Endosteal scalloping is a characteristic feature (Figure 5a-d). The primary significant factors of enchondromas are related to their complications, most notably pathologic fracture (Figure 5e-h). A small incidence of malignant transformation is noted, which may be associated with a pathologic fracture (Figure 5i-k). It is not infrequent to realize that a radiologically benign enchondroma showing a low grade chondrosarcomatous change histologically.
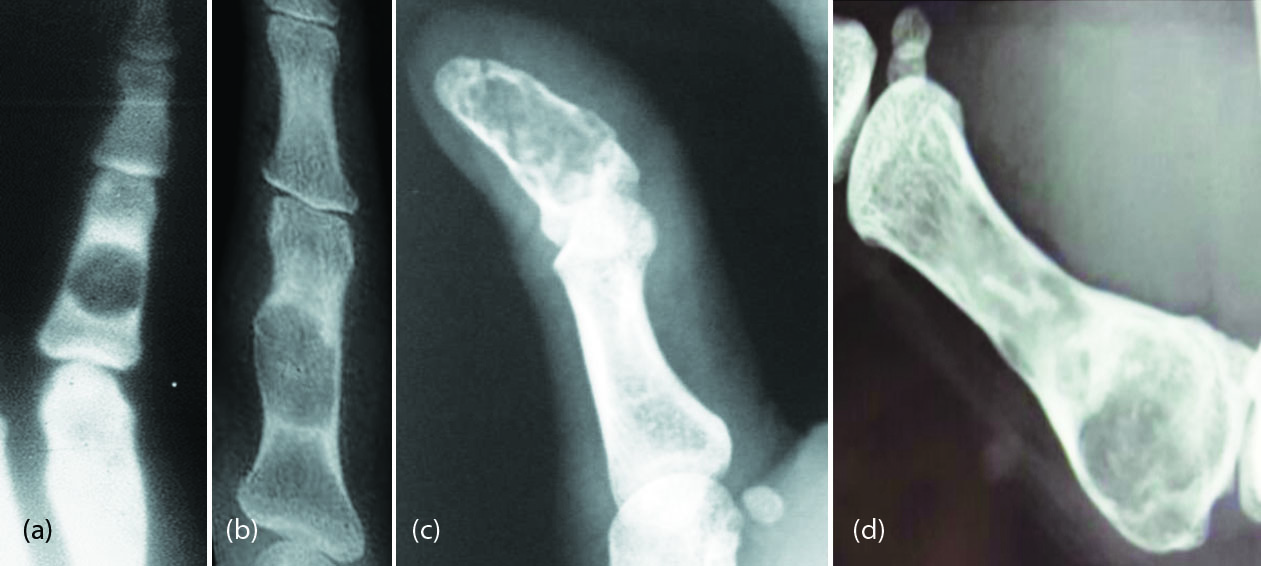
Figure 5a-d: Enchondroma spectrum; (a-c) phalanges, (d) metacarpal.
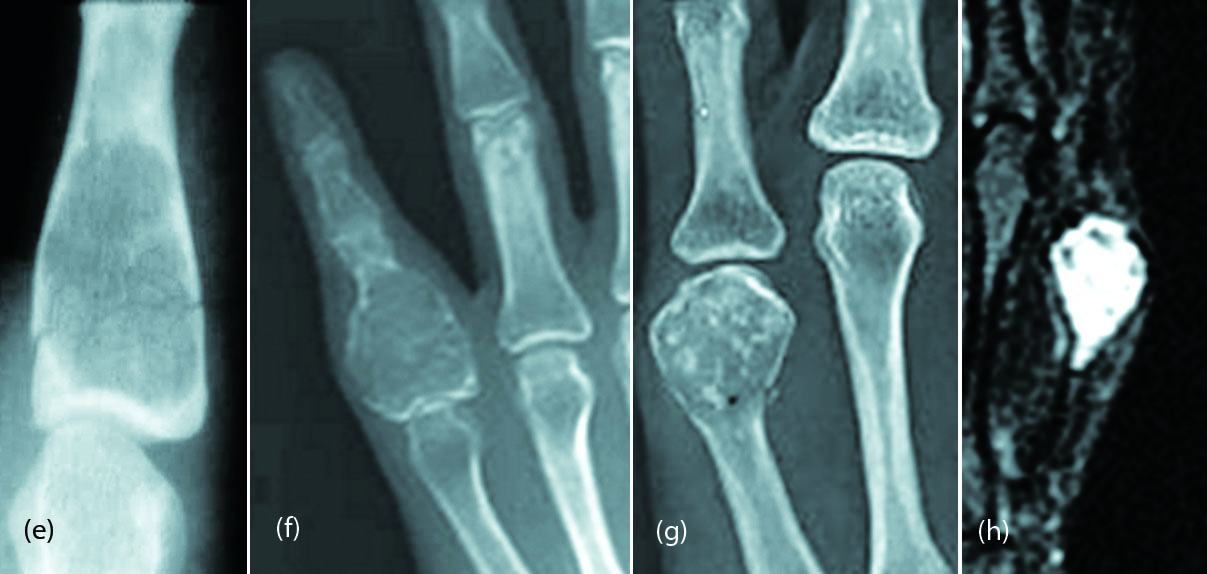
Figure 5e-h: Enchondroma with a fracture; (h) MRI of the same.
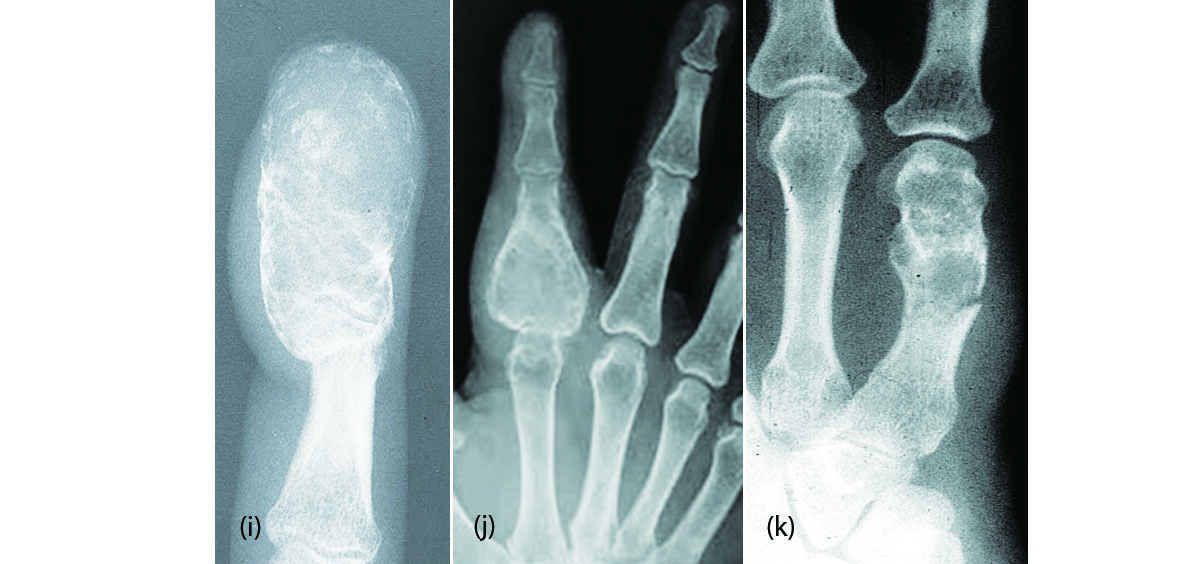
Figure 5i-k: Enchondroma with malignant transformation.
Enchondroma protuberans: It is a rare tumor that arises from an intramedullary enchondroma with an exophytic growth pattern (Figure 5l,m).

Figure 5l,m: Enchondroma protruberans 4th metacarpal; (m) MRI of the same.
Periosteal chondroma: It is also called ‘Juxtacortical chondroma’ and is a chondromatous lesion arising from the periosteum. It may grow into the medullary cavity. A characteristic cortical hook, similar to the hook noted in gout indicates the cartilaginous nature (Figure 6a-e). MRI is rarely necessary. Nodular calcification may be noted in the matrix (Figure 6c,f).

Figure 6a-e: Periosteal chondroma; (c) MRI of the same; (f) 24F, periosteal chondroma.
Exostosis (Osteochondroma): Isolated osteochondroma is rare in the bones of the hand (Figure 7a,b). A subungual exostosis may be occasionally encountered [6] (Figure 7c). However, in multiple exostoses bones of the hand may also be involved (Figure 7d).

Figure 7a,b: Exostosis of the distal phalanx; (c) Subungual exostosis; (d) Multiple exostoses in both hands.
Ollier’s disease: In Ollier disease, two types have been described. One is multiple enchondromas which often appear to be larger than they do in other conditions. Because enchondromas occur in young patients and can be large, growth of the affected limbs may be adversely affected, and pathologic fractures may occur (Figure 8a-d). Second type is Ollier’s dyschondroplasia where the appearance of linear lucencies, in which the chondrocytes appear to line up in a vertical orientation along the length of the bone. These lesions may be unilateral or bilateral and may shorten the bones (Figure 8e).
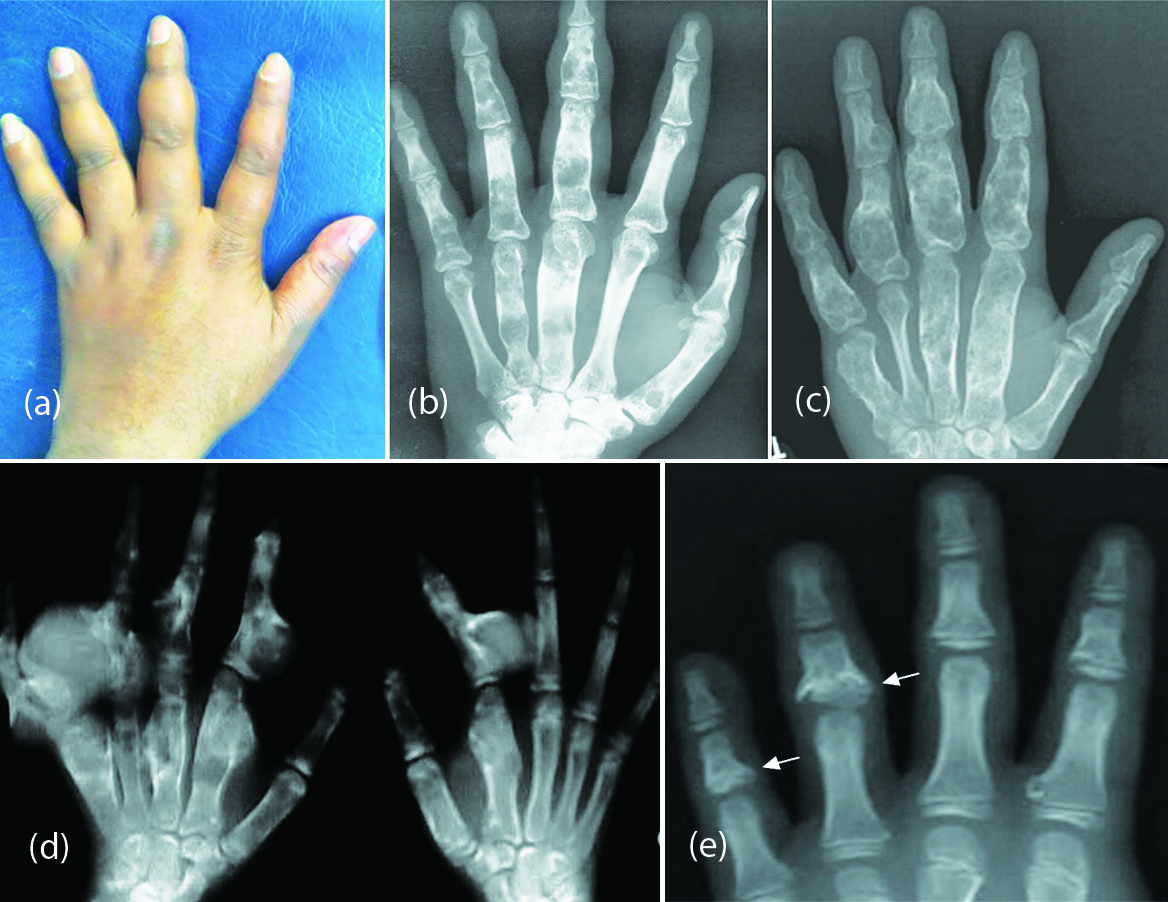
Figure 8: (a-d) Multiple enchondromatosis (Ollier disease); (e) Olliers dyschondroplasia involving the middle phalanges.
Maffucci syndrome: In Maffucci syndrome, multiple enchondromata with associated soft-tissue hemangiomas are seen. Soft-tissue hemangiomas typically have numerous rounded calcifications with central lucencies, which are consistent with phleboliths on plain radiograph (Figure 9b).
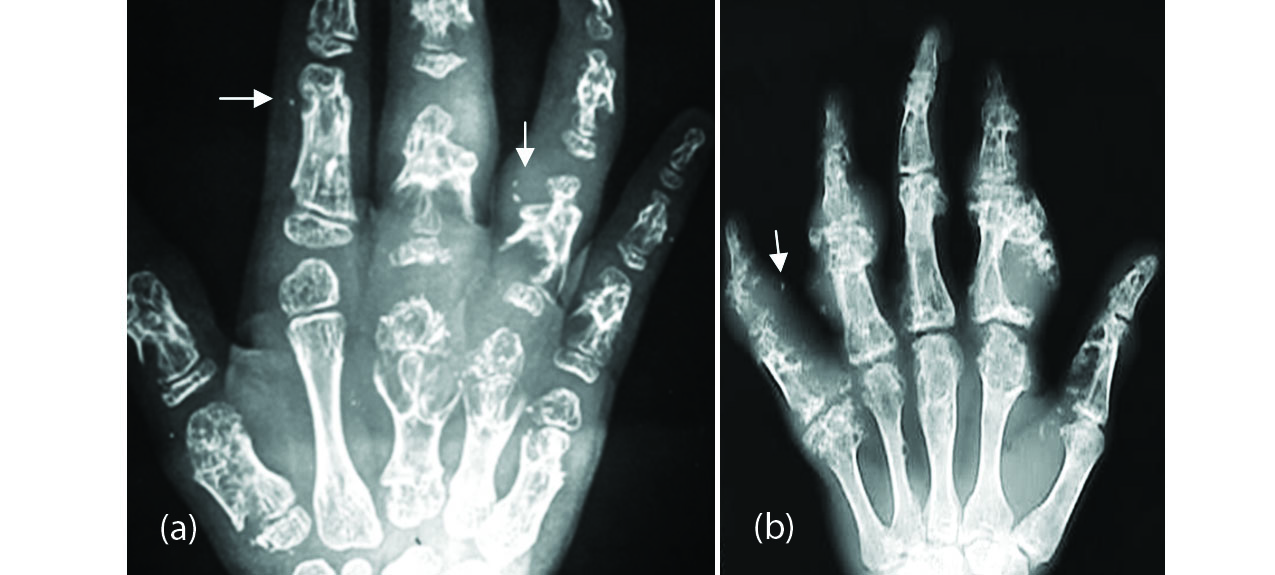
Figure 9: Mafucci syndrome; Note the phleboliths and enchondromata.
Metachondromatosis: Enchondromas and associated osteochondromas are noted, which differ from conventional osteochondromas in that they point toward rather than away from the joint (Figure 10). Metachondromatosis is the only one that is hereditary, which is by autosomal dominant transmission.

Figure 10: Metachondromatosis, multiple enchondromas and osteochondroma-like lesions.
Chondromyxoid fibroma: It is very rare as compared with other cartilaginous lesions. Although it is listed under cartilaginous tumor, calcification is rarely seen on radiographs. It is a lytic, eccentric and expanding lesion with lobulation and surrounding sclerosis (Figure 11).

Figure 11: 20M, chondromyxoid fibroma.
Chondroblastoma: Chondroblastoma of the hand bones has been reported. However, we have not encountered in our series.
Trevor’s: It is also called dysplasia epiphysealis hemimelica (DEH). It is a rare cartilaginous lesion arising from the epiphysis or ossification centre. It may involve the adjacent bone and generally has an unilateral distribution (Figure 12).
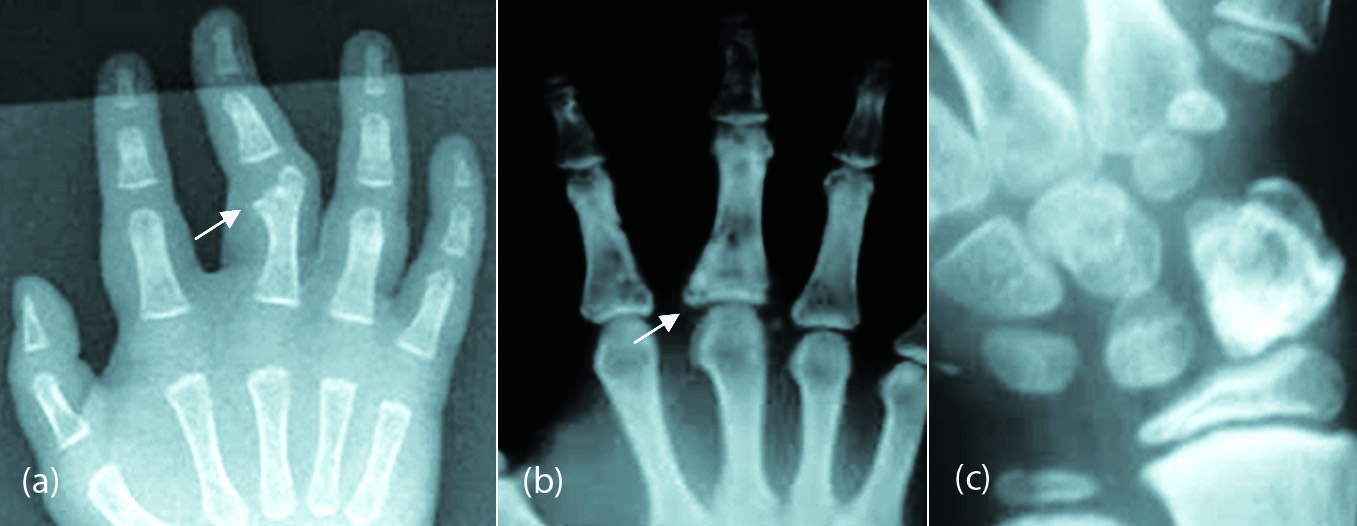
Figure 12: Trevor’s- (a) Proximal phalanx distally, (b) Proximal phalanx at the base, (c) Scaphoid.
Tumors of fibrous origin
- Non ossifying fibroma
- Fibroxanthoma
- Desmoplastic fibroma
- Cortical desmoid
These fibrous tumors are encountered in the long bones, but are rare in short bones. Vascular tumors of the hand bones are rare. However, glomus tumor is relatively common in the distal phalanges (Table 2).
Table 2: Vascular tumors.
|
|
Capillary
Cavernous
Venous
Arteriovenous malformation
|
|
|
|
|
|
|
|
|
Hemangioma: Radiological appearance of hemangioma is that of an expansile, lytic, fine lacy network or honey combing (Figure 13a-c). Radiating coarse linear strands diverging from center also may occur, simulating a sunray appearance. Angiogram demonstrates the type of hemangioma [7] (Figure 13d). Occasionally, hemangioma may produce reactive new bone and is sclerotic on radiographs (Figure 13e). On occasion it produces a multiloculated lytic lesion with a soft tissue swelling (Figure 13f).

Figure 13: (a,b) Hemangioma of proximal phalanx of ring finger, (c,d) Venous type of hemangioma of phalanx of index finger; (d) Venogram; (e) Sclerotic hemangioma.
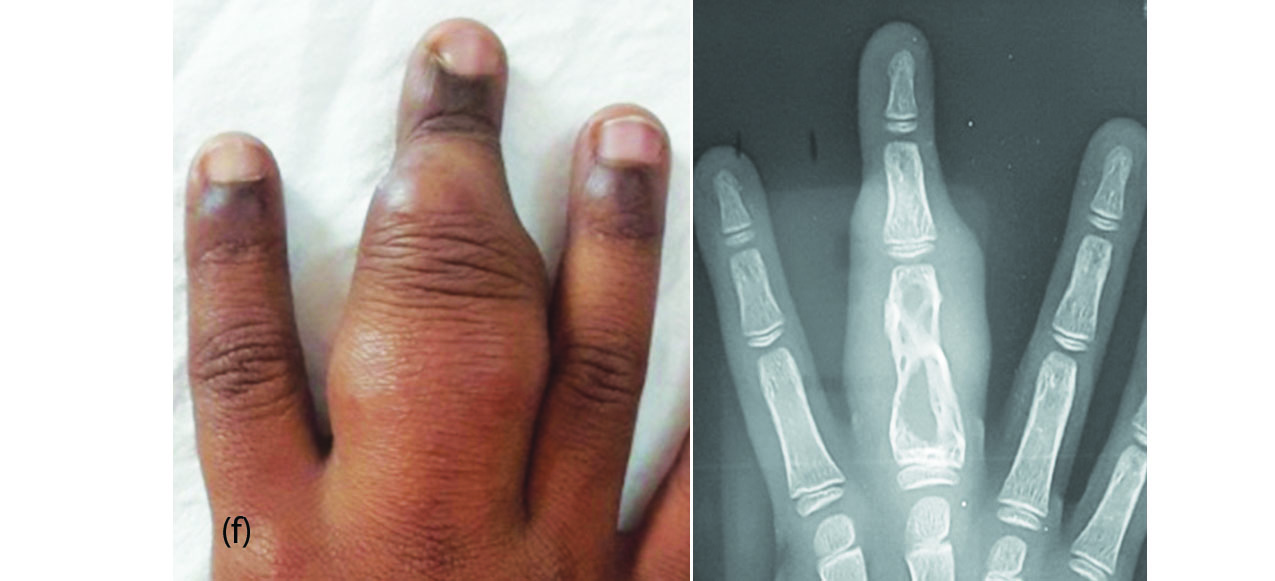
Figure 13f: Hemangioma involving the middle finger.
Cystic angiomatosis involves multiple sites of skeleton. Bones of the hands may also show hemangiomas. However, the radiological pattern is the same as solitary hemangioma.
Glomus tumor: It is a rare benign vascular tumor occurring in the terminal phalanx mostly of the fingers. Radiologically a lytic lesion is noted in the terminal phalanx with large soft tissue swelling (Figure 14a,b). In the differential diagnosis epidermoid inclusion cyst [8] may be considered. Epidermoid cysts also most commonly occur in the distal phalanges of the hands. A lucent lesion with surrounding sclerosis located in the distal phalanx is a classical finding (Figure 14c).
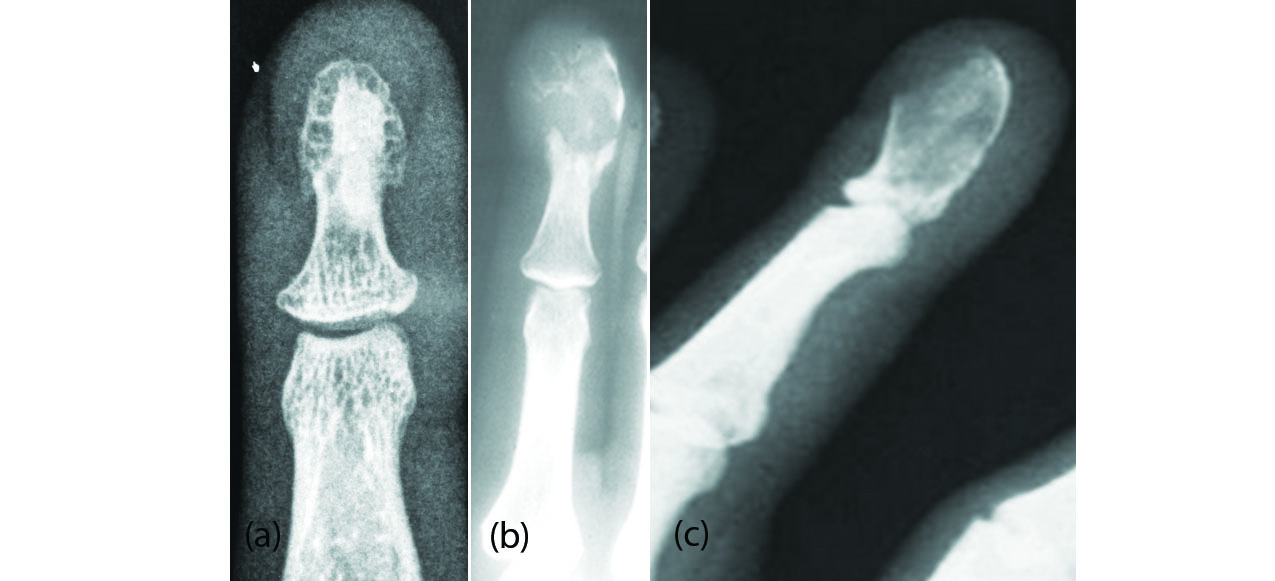
Figure 14: (a,b) Glomus tumor of the distal phalanx in two different patients; (c) epidermoid cyst.
Gorham disease: This is also known as vanishing bone lesion. Radiologically massive osteolysis of adjacent bones is noted without any sclerosis [9]. Generally, a single bone or multiple adjacent bones are affected (Figure 15).

Figure 15: Gorham disease involving carpals and metacarpals with extensive osteolysis.
Giant cell tumors
Giant cell tumour of the small bones of the hands and feet have also been described. Giant cell tumor is a most common benign tumor occurring at the ends of tubular bones [10]. It extends subarticularly with septae formation. The aggressive nature simulates malignant bone tumor. It occurs in the 3rd and 4th decades of life. They are mostly benign lytic lesions with a thin transitional zone without any matrix mineralization. No periosteal reaction is noted unless there is a fracture (Figure 16a-c). Sometimes it is difficult to differentiate this from aneurysmal bone cyst (ABC). Secondary ABC may be present in some of the giant cell tumors.
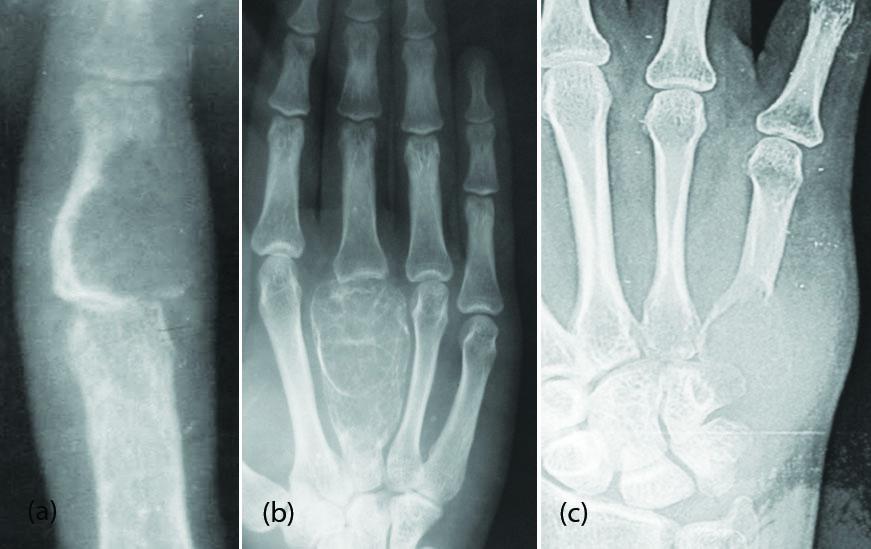
Figure 16: Giant cell tumor; (a) Middle phalanx, (b) 3rd metacarpal, (c) 5th metacarpal.
Aneurysmal bone cyst
It can be primary or secondary. Radiologically, it is an expanding osteolytic lesion with thinning of the cortex with a peripheral shell. The zone of transition is narrow but can be wide and aggressive (Figure 17a,b). The lesion may cross the growth plate in children [11]. Fluid fluid levels may be shown on CT/MRI [12]. These are often encountered in younger age groups.
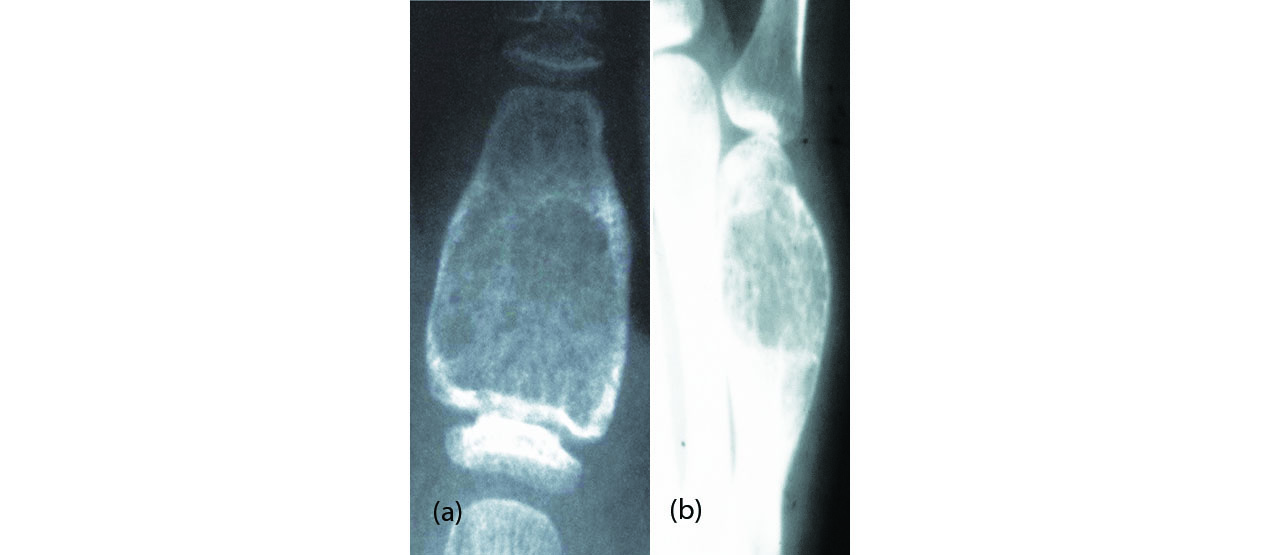
Figure 17: Aneurysmal bone cyst; (a) phalanx, (b) 5th metacarpal.
Conclusion
Benign tumors of the bones of the hands are very rare, although cartilaginous tumors are common. Other tumors of osseous nature and vascular origin are described with radiological characteristics. Giant cell tumors and aneurysmal bone cysts are also included. This pictorial essay deals mostly with conventional radiographs of the hands.
Acknowledgements
NIMS (Hyderabad), KIMS (Secunderabad) and KREST Museum (Hyderabad).
Conflicts of interest
Author declares no interests of conflicts.
References
[1] Samuel J Lin. Benign Hand Tumors; MedScape, Updted: May 17, 2017. Accessed from https://emedicine.medscape.com/article/1286448-overview
[2] Subbarao Kakarla. Benign tumors of bone, NJR. 2012; 2(1):1–12.
[3] Subbarao Kakarla. Benign cartilagenous lesions. J Med Sci Res. 2013; 1(1):29–36.
[4] Melamud K, Drapé JL, Hayashi D, Roemer FW, Zentner J, et al., Diagnostic imaging of benign and malignant osseous tumors of the fingers, musculoskeletal imaging; RSNA RadioGraphics. 2014; Vol.34, No.7.
[5] Plate AM, Lee SJ, Steiner G, Posner MA. Tumorlike lesions and benign tumors of the hand and wrist. J Am Acad Orthop Surg. 2003; 11(2):129–141.
[6] Campanelli A, Borradori L. Images in clinical medicine. Subungual exostosis. N. Engl. J. Med. 2008; 359(25):e31.
[7] Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, et al. From the archives of the AFIP. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics. 1995; 15(4):893–917.
[8] Greif EF. Intraosseous epidermoid cyst – probable; 2005-2018. Accessed from https://radiopaedia.org/cases/intraosseous-epidermoid-cyst-probable.
[9] Green HD, Mollica AJ, Karuza AS. Gorham's disease: a literature review and case reports. J Foot Ankle Surg. 1995; 34(5):435–441.
[10] Meena UK, Sharma YK, Saini N, Meena DS, Gahlot N. Giant cell tumours of hand bones: A report of two cases. J Hand Microsurg. 2015; 7(1):177–181.
[11] Crowe MM, Houdek MT, Moran SL, Kakar S. Aneurysmal bone cysts of the hand, wrist, and forearm. J Hand Surg Am. 2015; 40(10):2052–2057.
[12] Shooshtarizadeh T, Movahedinia S, Mostafavi H, Jamshidi K, Sami SH. Aneurysmal bone cyst: An analysis of 38 cases and report of four unusual surface ones. Arch Bone Jt Surg. 2016; 4(2):166–172.