Case Report
2016
March
Volume : 4
Issue : 1
Concurrent traumatic brain injury with aortic injury: Management dilemmas
Maulik Vaja, Manas Kumar Panigrahi, Rajendra Kumar Jain P, Ann Campos
Pdf Page Numbers :- 22-25
Maulik Vaja1*, Manas Kumar Panigrahi1, Rajendra Kumar Jain P2 and Ann Campos3
1Department of Neurosurgery, Krishna Institute of Medical Sciences, Secunderabad, Telangana, India
2Department of Cardiology, Krishna Institute of Medical Sciences, Secunderabad, Telangana, India
3Department of Anaesthesia and Critical Care, Krishna Institute of Medical Sciences, Secunderabad, Telangana, India
*Corresponding author: Dr. Maulik Vaja, Department of Neurosurgery, Krishna Institute of Medical Sciences, Secunderabad, Telangana, India. Email: maulik.vaja@yahoo.com
Received 12 October 2015; Revised 20 November 2015; Accepted 2 December 2015; Published 16 December 2015
Citation: Vaja M, Panigrahi MK, Jain RK, Campos A. Concurrent traumatic brain injury with aortic injury: Management dilemmas. J Med Sci Res. 2016; 4(1):22-25. DOI: http://dx.doi.org/10.17727/JMSR.2016/4-007
Copyright: © 2016 Vaja M, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Occurrence of concurrent traumatic brain injury and aortic injury is rare and potentially fatal trauma pattern. The incidence of traumatic brain injury associated with aortic injury is likely to be underestimated because many patients with this pathology die prior to hospital admission or imaging study. Even after diagnosis, there are difficulties in managing such a patient as different approaches are required to treat each of them.
Case report: A 68-year-old man with head injury and blunt chest injury was operated. He had right frontotemporal subarachnoid haemorrhage with fracture of left temporal bone with hemopneumothorax and multiple rib fractures on the left side of the chest. Patient was evaluated with plain CT scan and CT angiogram of brain. Contrast enhanced CT scan of chest revealed rupture of the arch of aorta. Head injury was managed conservatively and emergency aortic stent grafting was done.
Discussion and conclusion: Aortic injury may be missed, so the emergency physician should have high index of suspicion while dealing with polytrauma patient instead of just focussing on head injury. Head injury and aortic injury occurring together need different treatment methods which can have conflict. (A) In aortic injury, maintaining a lower systolic blood pressure is essential to prevent further haemorrhage. On the contrary blood pressure should be maintained at normal level for adequate cerebral perfusion in head injury. (B) Sedation required for aortic injury can interfere with the clinical assessment of a patient with traumatic brain injury. (C) Anticoagulants used in the treatment of aortic injury are usually contraindicated in head injury. The treatment needs a team approach by neurosurgeon, endovascular cardiologist, cardiac surgeon, emergency physician, and critical care intensivist etc., to manage patients of traumatic brain injury with aortic injury.
Keywords: Traumatic brain injury; aortic injury; fatal combination
Full Text
Occurrence of concurrent traumatic brain injury and aortic injury is rare and potentially fatal trauma pattern. The incidence of traumatic brain injury associated with aortic injury is likely to be underestimated because many patients with this pathology die prior to hospital admission or imaging study [1]. In a country like India most of the patients may not reach in time a hospital, to be diagnosed and treated. Because traumatic brain injury is the leading cause of death in all trauma patients, and aortic injury is the second most common cause of death in newer studies [2, 3], many clinicians believe that the traumatic brain injury/aortic injury represents an unsurvivable condition. Aortic injury alone carried a mortality rate of 80% in 1958 [1].
With improvement in transportation and medical facilities, more patients with aortic injury are likely to reach hospitals. It is important that we look out for aortic injury in all cases of trauma. Unless we suspect we may not be able to manage appropriately. It is possible that in some cases with head injury the mortality might have been due to aortic injury but attributed to head injury itself. Head injury and aortic injury occurring together need different treatment methods, which can have conflict [4]. In aortic injury, maintaining a lower systolic blood pressure, cardiac output, and heart rate are essential to prevent further problems [5]. Generally we avoid hypotension to maintain cerebral perfusion pressure in head injury to prevent secondary brain damage [3, 6].
Sedation advocated in aortic injury interferes with assessment of consciousness level (Glasgow Coma Scale) in head injury. Periodic CT scans for assessing the progression of head injury may not be possible in hemodynamically unstable aortic injury patients. Anticoagulants in the treatment of aortic injury are usually contraindicated in head injury.
Case report
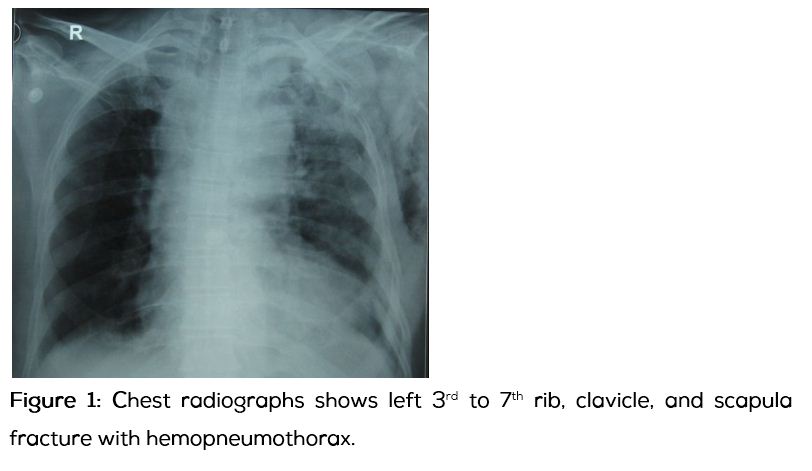
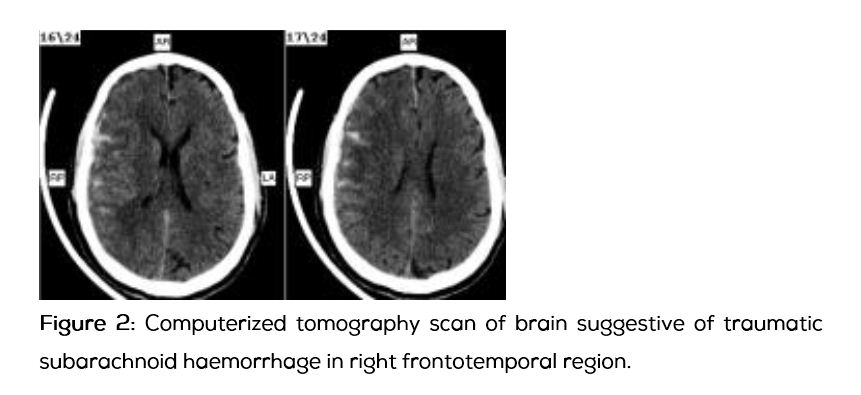
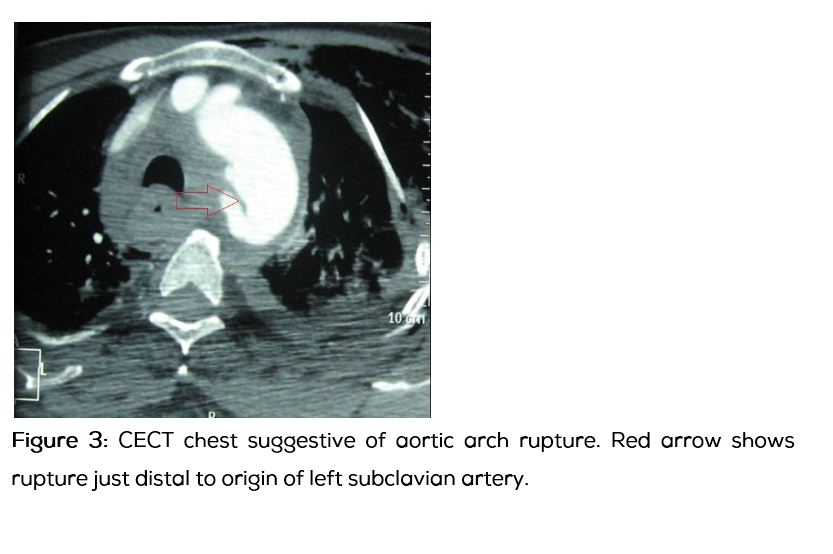
A 68-year-old male patient who was a known case of hypertension was brought to the emergency department within 4 hours of a road accident. He had a vomiting, bleeding from left ear, and pain on the left side of his chest. On examination he had a normal pulse rate and blood pressure was 150/80. He had tenderness and subcutaneous emphysema over the left side of his chest with crepitations over left clavicle and scapular region. Air entry was decreased on the left side of chest. Oxygen saturation in peripheral blood vessels was 88%, which improved with oxygenation through mask. He had normal heart sounds with normal peripheral pulses. The patient was confused and drowsy with a Glasgow Coma Scale of 13/15. There was no other neurological deficit. All routine blood investigations were normal with haemoglobin 13 gram per decilitre, normal electrolytes. Chest x-ray showed pneumothorax and fractures of 3rd to 7th ribs, clavicle and scapula on left side (Figure 1). CT scan of the brain showed right frontotemporal subarachnoid haemorrhage with fracture of left petrous temporal bone (Figure 2). CECT scan of chest showed rupture of aorta into mediastinum (Figure 3). CT angiogram of the brain revealed no vascular abnormality.
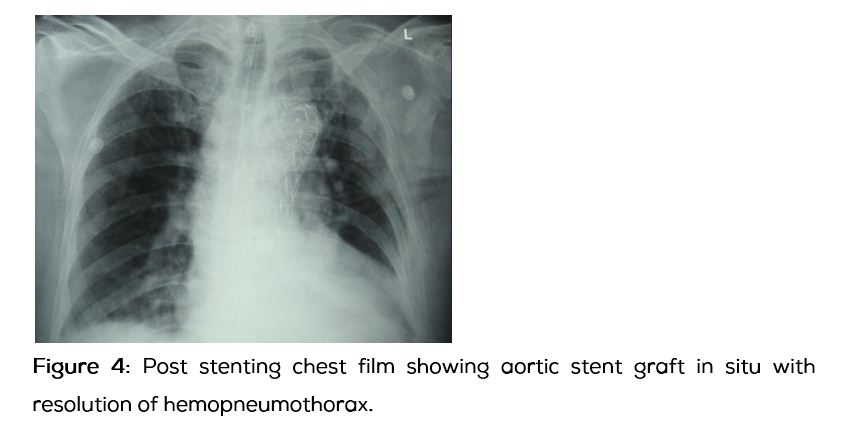
The head injury was treated conservatively and an aortic stenting (expandable metallic stent graft) was performed (Figure 4).
The patient showed steady improvement clinicoimageologically and was discharged after 12 days of hospital stay. He was fully conscious and without any neurovascular deficit. In view of aortic stenting, low dose aspirin was started at the time of discharge. On follow up he developed right hemispheric chronic subdural haematoma, which was managed surgically by burr hole evacuation. He did well and was discharged without any neurological deficits.
Discussion
Concurrent injury to brain and thoracic major vessels (aortic segments) are one the most critical combinations in polytrauma. Due to its lethal and rare occurrences few studies have been done [1, 7]. With developments in medical care and transportation facilities, emergency physicians are likely to encounter such patients and thus there is a need to evolve a strategy to successfully deal with such situations.
The patient we treated had aortic rupture at the isthmus of aortic arch, just distal to origin of left subclavian artery, which is the most common site of aortic injury in blunt chest trauma [8]. Ascending aorta and aortic arch injury are managed with endovascular treatment. While descending aortic injury is managed by surgical treatment [8].
Aortic injury being second most common cause of death due to trauma needs early diagnosis and treatment [2, 3]. Early detection requires CT scan of chest. So it should be a routine protocol to do CT scan of chest in all polytrauma patients with clinical evidence of chest injury, as some of the patients may have hemodynamic stability in spite of major thoracic vascular injury. Untreated aortic injuries can worsen with devastating consequences. The current standard of care is for strict control of blood pressure with deep sedation [5]. Maintenance of normal blood pressure is advocated for cerebral perfusion in case of traumatic brain injury. Deep sedation will mask the clinical picture of worsening of traumatic brain injury. Hemodynamic instability due to major thoracic vascular injury will restrict the mobility which is often required for radiological evaluation of traumatic brain injury.
The use of anticoagulation therapy during and after endovascular repair of aortic injury is another challenge in the management of simultaneous traumatic brain injury and aortic injury. In our patient we administered conventional heparin 3000 international unit with monitoring of activated clotting time during stenting. Low molecular weight heparin was administered as a prophylactic anticoagulant for 1 week, followed by conventional single oral antiplatelet medications. He developed right sided chronic subdural haematoma after few weeks. It is suggested that a follow-up CT scan of brain has to be performed within 4 to 6 hours of the initial imaging. If the intracranial lesions are stable and not exerting a significant amount of mass effect, then we may proceed with early endovascular repair of the aortic injury [7]. The lowest effective dosage of intravenous conventional heparin (3000 international unit) for stenting is recommended as considered appropriate by the vascular surgical service, and several patients in this series were successfully treated without intravenous heparin. In a small, randomized, controlled trial, Phalen et al., demonstrated that in low-risk traumatic brain injury, deep venous thrombosis prophylaxis with low molecular weight heparin may be started 24 hours after injury without increased intracranial haemorrhage when compared with placebo [9]. Also, in a large retrospective series by Norwood et al., 8.3% of intracranial haemorrhages showed progression after the initiation of low-molecular-weight heparin an average of 36 hours after blunt trauma injury [10].
Still there is no clear-cut criteria for lowest safe and effective dosage of anticoagulant, which can be used for endovascular and operative intervention for patient who have major vascular injury along with traumatic brain injury, so as not to worsen the head injury. We could not found any protocol for appropriate timing for radiological evaluation of brain injury after endovascular or operative treatment of major vascular injury.
Conclusion
High index of suspicion is required to detect aortic injury in all chest injury and polytrauma patients. However, with appropriate treatment, many patients with concurrent aortic injury and traumatic brain injury can survive long enough to be discharged home or to inpatient rehabilitation facilities. The treatment needs a team approach by neurosurgeon, endovascular cardiologist, cardiac surgeon, emergency physician, and critical care intensivist etc. to manage patients of traumatic brain injury with aortic injury.
Acknowledgements
Acknowledgements are due to Departments of Endocrinology, and Radiology, Krishna Institute of Medical Sciences (KIMS), Secunderabad.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Parmley LF, Mattingly TW, Manion WC, Jahnke EJ Jr. Non-penetrating traumatic injury of aorta. Circulation. 1958; 17(6):1086–1101.
2. Coronado VG, Xu L, Basavaraju SV, McGuire LC, Wald MM, et al. Surveillance for traumatic brain injury-related deaths--United States, 1997 – 2007. MMWR Surveill Summ. 2011; 60(5):1–32.
3. Harris T, Davenport R, Hurst T, Hunt P, Fotheringham T, et al. Improving outcome in severe trauma: what’s new in ABC? Imaging, bleeding and brain injury. Postgrad Med J. 2012; 88(1044):595–603.
4. Hong MS, Feezor RJ, Lee WA, Nelson PR. The advent of thoracic endovascular aortic repair is associated with broadened treatment eligibility and decreased overall mortality in traumatic thoracic aortic injury. J Vasc Surg. 2011; 53(1):36–43.
5. Mosquera VX, Marini M, Lopez-perez JM, Muñiz-Garcia J, Herrera JM, et al. Role of conservative management in traumatic aortic injury: comparison of long term results of conservative, surgical and endovascular treatment. J Thorac cardiovasc surg. 2011; 142(3):614–621.
6. Andrews PJ, Sleeman DH, Statham PF, McQuatt A, Corruble V, et al. Predicting recovery in patient suffering from traumatic brain injury by using admission variables and physiological data: a comparison between decision tree analysis and logistic regression. J Neurosurg. 2001; 97(2):326–336.
7. Kitagawa RS, Van Haren RM, Yokobori S, Cohen D, Beckerman SR, et al. Management of simultaneous traumatic brain injury and aortic injury. J Neurosurg. 2013; 119(2):324–331.
8. Lawlor DK, Ott M, Forbes TL, Kribs S, Harris KA, et al. Endovascular management of traumatic thoracic aortic injuries. Can J Surg. 2005; 48(4):293–297.
9. Phalen HA, Wolf SE, Norwood SH, Aldy K, Brakenridge SC, et al. A randomized, double-blinded, placebo controlled pilot trial of anticoagulation in low-risk traumatic brain injury: The Delayed Versus Early Enoxaparin Prophylaxis I (DEEP I) study. J Trauma Acute Care Surg. 2012; 73(6):1434–1441.
10. Norwood SH, Berne JD, Rowe SA, Villarreal DH, Ledlie JT. Early venous thrombo-embolism prophylaxis with Enoxaparin in patients with blunt traumatic brain injury. J Trauma. 2008; 65(5):1021–1027.