Full Text
Introduction
On 31 December 2019, the World Health Organization (WHO) China Country Office was informed of cases of pneumonia of unknown aetiology (unknown cause) detected in Wuhan City, Hubei Province of China. The virus has been renamed by WHO as SARS-CoV-2 [1].
The first case in India was reported on January 30, 2020, 100th case on March 17, 1000th case on 30 March, and 10,000th case on 14 April and total cases were 24,642 and 779 deaths with a case fatality rate of 3.2% [2]. Maharashtra has reported the highest number of cases in India with 6817 total cases and 310 total deaths on 25th April with a mortality of 4.4% [3].
Training of human resources is immensely important as the disease is new for everyone and impact of the disease in shorter duration has increased the need of trained man power to cope the pandemic. With this view, Government of India initiated Integrated Government Online Training (iGOT) [4] platform for training of human resources. iGOT training was imparted to all doctors, residents according to the guidelines of government of India in our institute. The present study was conducted with an aim to evaluate the knowledge of doctors regarding COVID-19 and emphasize on need of such trainings for capacity building.
Methodology
The present study was an across sectional observational study carried out in a duration of two months from April 2020 to May 2020. In view of pandemic of COVID-19, iGOT [4] platform for training of human resources regarding COVID-19. IGOT training was imparted to all resident doctors, in the tertiary care hospital according to the guidelines of government of India. All the resident doctors attended training (Total 88) participated in the study. The questions at the end of each session were included in the Google questionnaire of the study. Questionnaire included total 53 questions including areas of general precautions by public, infection prevention and control in hospital settings, rational use of PPE, donning doffing procedures, laboratory testing, management of COVID-19, in ANC & PNC and paediatric care during COVID-19, dead body management, disinfection [4].
All delegates attending the training (Total 88) were invited to join a social media group. A social media group was utilised to circulate the iGOT questionnaire prepared using Google forms, to all delegates. Total 88 resident doctors participated in the study. Confidentiality of participants was maintained. No prospective disadvantages or ethical issues were foreseen as the study was only questionnaire based observational study. Such a survey of educational practices is exempt from ethics committee review as per the Indian Council of Medical Research (ICMR) guidelines. Percentages and bar diagram were the statistical methods [5] used to analyze and represent the data.
Results
Total 88 participants were studied. Results obtained from study are described below.
Knowledge regarding disinfection and precautions to be taken at hospital settings showed that, only 51.2% participants correctly answered that airborne precautions are required to be taken at triage areas. Only 60% delegates knew that service corridor and dedicated lift is required for transport of COVID-19 patients. Designated nursing officer should look after biomedical hazard symbol on room doors of suspect wards was known to 62.5% delegates. Approximately 15% delegates didn’t know that, management of laundry, management of food services and management of utensils is a part of environmental cleaning and disinfection. Cleaning dust from furniture is not a part of cleaning guidelines was correctly answered by 71.4% delegates. While 19% delegates wrongly believed that use of biohazard bags is not a part of guidelines. 9.5 % delegates didn’t know that wiping surfaces is a part of cleaning guidelines. 31.3% delegates could not correctly answer the sequence of donning and doffing.
The study showed that, 95.3% participants knew all routes of transmission while 4.7% didn’t know that not wearing recommended PPE and direct physical contact with COVID-19 patient can also transmit the disease. 93% delegates answered correctly regarding discharge policy of patients. 22.6% delegates were unaware that home quarantine for 14 days is advised after discharge of COVID-19 patient.

Figure 1: Level of knowledge regarding laboratory testing of COVID-19 (n=88).
63% participants knew that rapid antibody testing is used to find exposure to COVID-19. Testing can be done only in ICMR recommended public and private labs were correctly answered by 84.7% participants. Only 50.6% participants were aware that senders address, contact number, packaging list or proforma invoice, airway bill or value equivalence document are the required documents to be sent along with sample. Correct sequence of packaging the sample is primary container, followed by secondary container followed by zip lock pouch followed by plastic container in the card board box. Only 62% participants answered it correctly. 99% participants were knowing about the criteria by ICMR for COVID-19 testing, after training.
Knowledge regarding clinical picture of disease was better as 80% participants answered correctly questions related to this. Indication for use of lopinavir, ritonavir was correctly answered by 64.1% participants.
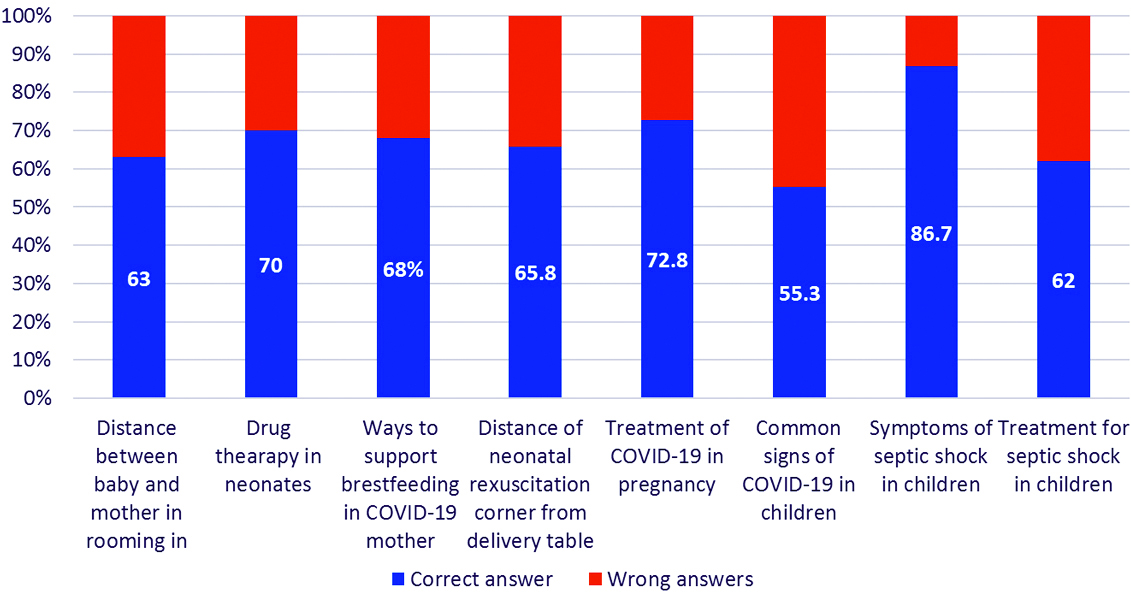
Figure 2: Level of knowledge regarding antenatal, postnatal and paediatric care in COVID-19 (n=88).
63% participants correctly told regarding distance between mother and child in PNC ward as >6 feet. 70% participants knew that HCQ, systemic corticosteroids, IVGs is not to be given in neonates. 89.5% participants correctly answered testing guidelines for neonates. Expressed milk, relactation, donor human milk can be used to support women with COVID-19 who are too unwell to breastfeed was known to 68% participants only. 65.8% participants correctly answered that at least 2-meter distance should be maintained between neonatal resuscitation and delivery table.
55.3% participants correctly answered persistent pain or pressure in chest as common sign of COVID-19 in children in severe disease. 86.7% participants correctly answered that bradycardia or tachycardia, weak pulse, hyperthermia or hypothermia is a clinical presentation of septic shock in COVID-19 positive children, while antimicrobial, vasopressor and fluid loading all are used as treatment of septic shock in COVID-19 positive children, was correctly answered by only 62% participants after iGOT training.
Discussion
Digital technology innovations are known to present the possibility of improving the efficacy of the health system response to an epidemic [6-8]. In the study carried out by Kamate et al., good knowledge scores were significantly associated with qualifications (p = 0.04) and years of practice (p = 0.02); good practice scores were associated with qualifications only (p = 0.03)[9].
In present study, 95.3% participants knew all routes of transmission but only 51.2% participants correctly answered that airborne precautions are required to be takenin hospital and triage area. Correct sequence of packaging was answered correctly by 62% participants only. Knowledge regarding clinical picture of disease was adequate as 80% participants answered correctly questions related to this. while in the study, named “Prevalent fears and inadequate understanding of COVID-19 among medical undergraduates in India: results of a web-based survey” carried out by Agarwal et al [10], Knowledge regarding the viral transmission (97.7%), clinical-radiologic features (72.1%), laboratory diagnosis (87%) and drugs being tried out to treat COVID-19 (95%), was adequate among most students however, the understanding of the incubation period (20%) and time to symptoms (4.8%) was less than satisfactory. In present study knowledge regarding laboratory diagnosis and management was less than study [10]. This stresses on the need of repeated training from experts in peripheral health care institutes for better patient care.
Most common source of information regarding recent guidelines and knowledge regarding COVID-19 was ICMR website, and 62% of total participants checked the website daily or once in two days in last two months. The findings were similar to the study carried out by Agarwal et al [10], which showed that 40.6% were not up-to-date on COVID-19, and most (78.9%) resorted to social media for information on COVID-19.
Present study has similar findings with studies which show knowledge deficit and insufficient awareness of the preventive and treatment strategies amid poor reading practices among students [11-12]. Present study was carried out at one health care institute only with the use of self-reported questionary. A large multicentric study is needed to understand preparedness of health professionals for the fight against COVID-19. This is also needed to understand implementation practices of ICMR, MOHFW guidelines in clinical practice by health care professionals regarding COVID-19 over wide regions in India.
Conclusion
More stress should be given in the training on precautions to be taken triage areas, sample collection and transfer, use of antiviral drugs and management in antenatal, postnatal and paediatric age group. The iGOT training was found very useful in doctors for capacity building for COVID-19 pandemic. This study emphasizes need of training regarding COVID-19 in every health care institution for capacity building.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Ministry of Health & Family Welfare Government of India, Containment Plan Novel Coronavirus Disease 2019 (COVID-19), March 2020. Available from: https://www.mohfw.gov.in/
[2] COVID-19 India and state wise status as on 24 Apr 2020 & 12 May 2020. Available from: https://www.mohfw.gov. in
[3] Tambe MP, Parande MA, Tapare VS, Borle PS, Lakde RN, et al. An epidemiological study of laboratory confirmed COVID-19 cases admitted in a tertiary care hospital of Pune, Maharashtra. Indian J Public Health. 2020; 64(Suppl):S183–S187.
[4] iGOT courses on DIKSH A platform on COVID-19 pandemic. Available form: https://diksha.gov.in/igot/explorecourse?gradeLevel=Doctor&appliedFilters=true
[5] Ethical Guidelines for Biomedical Research on Human Participants, Indian Council of Medical Research, New Delhi, 2006. Available at http://icmr.nic.in/ethical_guidelines.pdf
[6] Wood CS, Thomas MR, Budd J, Mashamba-Thompson TP, Herbst K, et al. Taking connected mobile-health diagnostics of infectious diseases to the field. Nature. 2019; 566(7745):467–474.
[7] World Health Organization. Digital technology for COVID-19 response. Geneva: WHO; 2020. Available from: https://www.who.int/news/item/03-04-2020-digital-technology-for-covid-19-response
[8] Reeves JJ, Hollandsworth HM, Torriani FJ, Taplitz R, Abeles S, et al. Rapid response to COVID-19: Health informatics support for outbreak management in an academic health system. J Am Med Inform Assoc. 2020; 27(6):853–859.
[9] Kamate SK, Sharma S, Thakar S, Srivastava D, Sengupta K, et al. Assessing knowledge, attitudes and practices of dental practitioners regarding the COVID-19 pandemic: a multinational study. Dent Med Probl. 2020; 57(1):11–17.
[10] Agarwal V, Gupta L, Davalbhakta S, Misra DP, Agarwal V, et al. Prevalent fears and inadequate understanding of COVID-19 among medical undergraduates in India: results of a web-based survey. J R Coll Physicians Edinb. 2020; 50(3):343–350.
[11] Gupta AS. Perception about social media use by rheumatology journals: Survey among the attendees of IRACON 2019. Ind J Rheumatol. 2020; 15(3):171–174.
[12] Goel a, Gupta L. Social Media in the Times of COVID-19. J of Clin Rheumatol. 2020; Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7437428/pdf/rhu-publish-ahead-of-print-10.1097.rhu.0000000000001508.pdf