Full Text
Introduction
Unifocal sclerotic bone lesions are either symptomatic or asymptomatic. Evaluation of the lesion is important in the diagnosis and management of these lesions. The radiological characteristics are described in detail so that a final diagnosis can be made [1-3]. A sclerotic bone lesion radiologically may appear as homogenous and dense lesion. The entire lesion may not be sclerotic but if three fourths of the lesion is sclerotic, it can be called as a sclerotic lesion. The etiology of this lesion is varied and various lesions are listed below (Table 1).
Table 1: Etiology - The differential diagnosis of a solitary sclerotic bone lesion is heavily influenced by the age of the patient, and includes.
|
· Bone island
· Enostosis
· Fibrous dysplasia
· Post traumatic/ stress, callus
· Inflammatory/ infection
· Sclerosing osteomyelitis
· Osteoma
· Osteoid osteoma
· Osteoblastoma
· Osteosarcoma
· Enchondroma
· Healed fibrous lesions
· Ewing's sarcoma
· Lymphoma
· Plasmacytoma
· Paget's disease
· Healed brown tumors
|
The first modality that detects the sclerotic lesion is by conventional radiology. Computerized tomography (CT), magnetic resonance imaging (MRI), radionucliec scan and positron emission tomography (PET) CT are advanced technics that help to pinpoint the final diagnosis. Ultimately, histopathology report is necessary.
Unifocal sclerotic lesions with discussion on imaging - Congenital/ developmental bone island
A bone island, also known as an enostosis, is a focus of compact bone located in cancellous bone (Figure 1a-i). This is a benign entity that is usually found incidentally on imaging studies; however, the bone island may mimic a more sinister process, such as an osteoblastic metastasis (for example, from prostate cancer). Bone islands demonstrate characteristic radiographic findings. In the correct clinical context, findings on radiographs are considered diagnostic. However, if the lesion is large or demonstrates increased scintigraphic activity, or if the patient is symptomatic or has a history of malignancy, clinical follow-up and/or biopsy may be warranted.
Bone islands typically appear as sclerotic, round-to-ovoid intramedullary foci. The long axis of the bone island is aligned parallel to the long axis of the bone [4-6].

Figure 1a-c: (a) Bone island in calcaneum. (b, c): Giant bone Island in lower end of tibia.
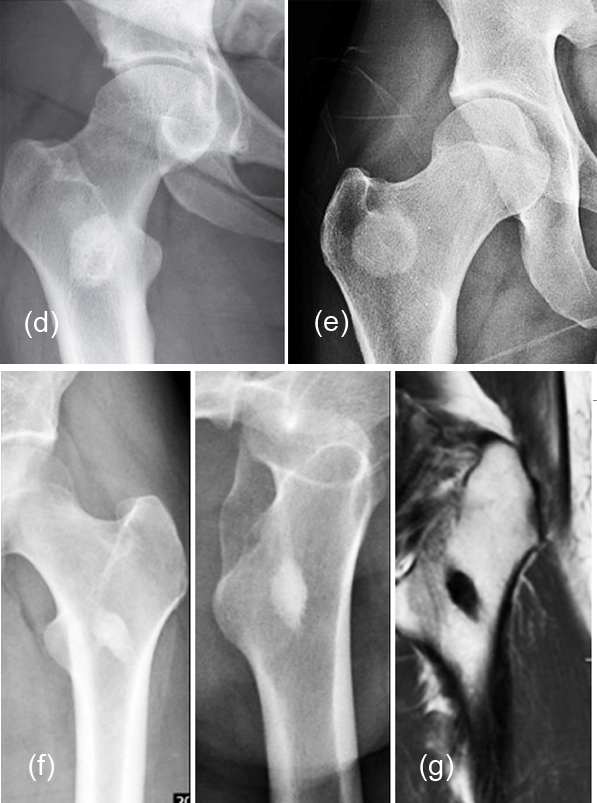
Figure 1d-g: (d,e,f) Bone Islands in different patients, (g) MRI.

Figure 1h, i: Growing bone island in a 2 year period.
Enostosis
An enostosis is a small area of compact bone within the cancellous bone. They are commonly seen as incidental findings on radiographs or CT scans. They are typically very small and do not cause any symptoms (Figure 2a, b). Their radiodensity is generally similar to cortical bone. Most of the authors treat enostosis as same as bone island. However, enostosis is linear, oblong, and close to the endosteum [3, 4].
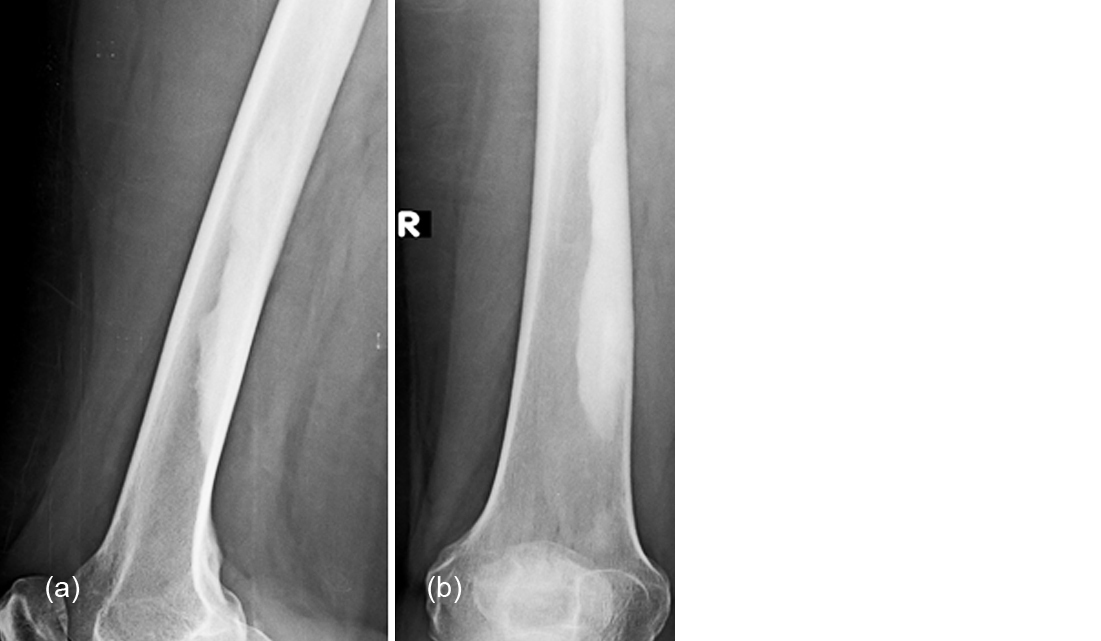
Figure 2a, b: Enostosis, lower end of femur.
Fibrous dysplasia
Fibrous dysplasia (FD) is a developmental disorder with replacement of the osseous part with fibrous tissue. Three major forms are described but unifocal sclerotic FD is quite rare. Often biopsy is required to make a final diagnosis. Skull and facial bones are the most common sites. Polyostotic involvement should be ruled out before it is called to be unifocal [7, 8]. Radiologically, solitary sclerotic area is noted with a ground glass type of matrix (Figure 3a-c). The margins are well outlined without any soft tissue swelling or periosteal reaction.
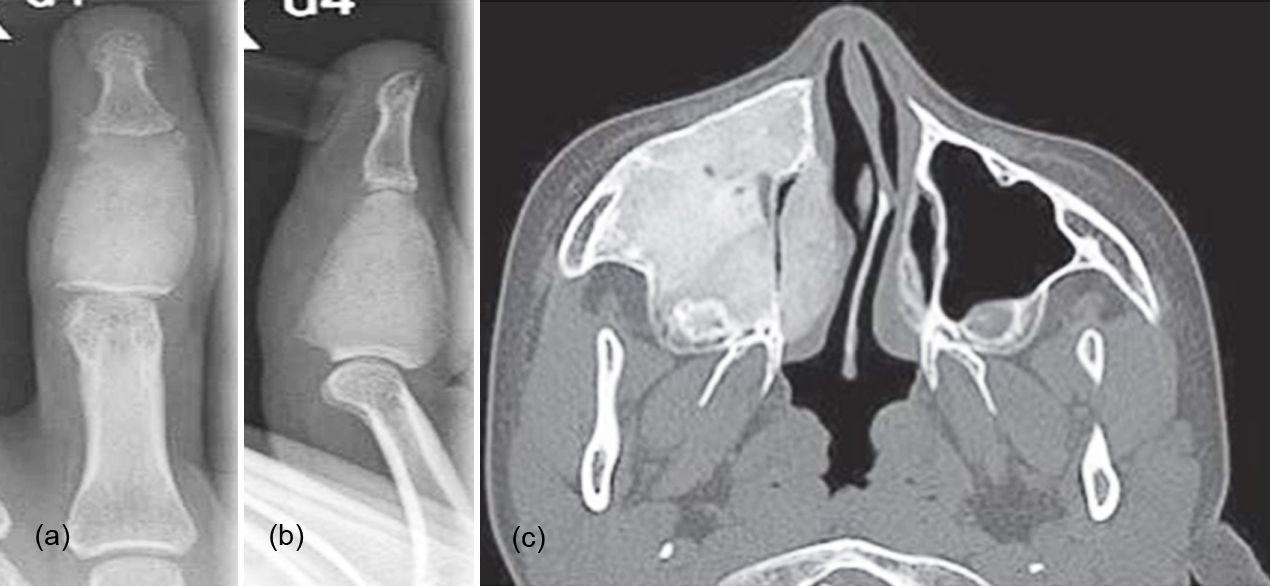
Figure 3: (a, b) Fibrous dysplasia involving the middle phalanx of the middle finger, (c) Maxilla.
Post traumatic/ Stress
Healed fractures may show dense sclerotic lesion simulating osteoid osteoma. Hypercallosis is noted in some clinical conditions such as osteogenesis imperfecta, and neurological disorders. History of trauma is essential to make a diagnosis. Bone grafts may also show unifocal sclerotic lesion during healing stage and history is essential to make a diagnosis (Figure 4a-e). Stress lesions including fractures show sclerosis subsequent to healing. Stress and ischemic lesions produce sclerosis (Figure 4f) [9, 10]. Stress lesions need not show the fracture line all the time even with CT. Radionuclide scan identifies the lesion.
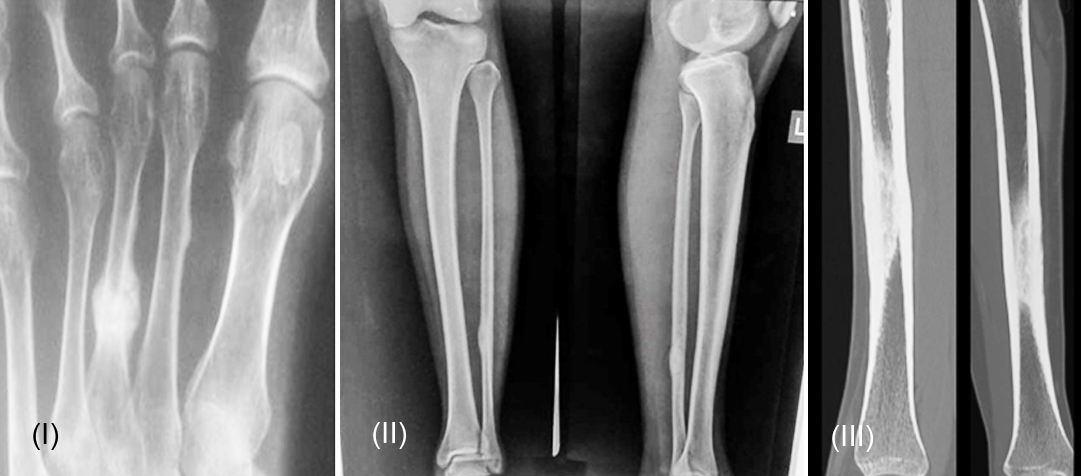
Figure 4a: (i) Healing fracture 3rd metatarsal with callus; (ii, iii) Healed stress fracture.

Figure 4b-g: (b, c) Healed stress fracture in typical location. (d, e): Freibergs disease dense 2nd metatarsal head. (f): Stress lesion tibia. (g): Post op, excessive callus.
Osteonecrosis - Avascular necrosis
It often occurs in the articular ends of the long bones and there are many causes. Head of the femur is the most common site. Avascular necrosis may be the result of the following:
• Injury / Fracture
• Damage to blood vessels
• Long-term use of drugs, such as corticosteroids
• Excessive, long-term use of alcohol
• Specific chronic medical conditions
• Radiation
Radiologically several grades are observed depending upon the stage of the disease. In the final stage sclerosis is predominant (Figure 4f).
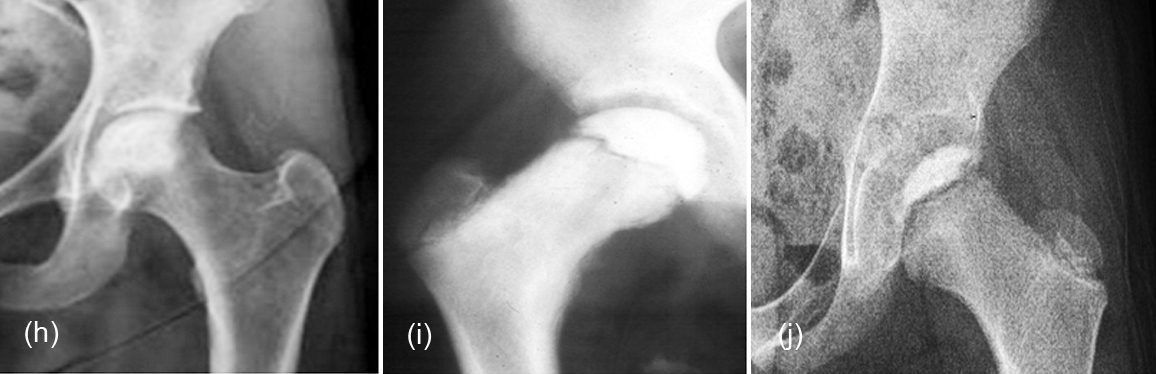
Figure 4h-j: (h) Avascular necrosis femoral head, (I, j) Legg-Calve-Perthes.
Inflammatory/ Infection
Inflammatory lesions such as Langerhans cell histiocytosis and sarcoidosis may produce sclerotic lesions. Langerhans cell histiocytosis (LCH) represents a spectrum of rare disorders characterised by idiopathic infiltration and accumulation of abnormal histiocytes. It may be unifocal or multifocal [11]. When it is unifocal it is called eosinophilic granuloma. In the healed phase of a single lesion, sclerosis is noted which may be mistaken for other lesions. Osteomyelitis of Garre’s type presents as sclerotic lesion and so also does healed osteomyelitis.
LCH is a nonspecific granulomatous lesion and generally gives lytic and mixed type of bone lesions. Eosinophilic granuloma can be unifocal but sclerotic appearance is extremely rare except when it is healed.
Bone infections – Osteomyelitis
Except in Garre’s type of osteomyelitis, unifocal sclerotic lesion is not seen in osteomyelitis, whether acute or chronic.
Sclerosing osteomyelitis of Garré
In 1893 Garre described a peculiar form of chronic low grade, diffuse, non-purulent osteomyelitis characterized by a striking absence of viable pathogens on attempted tissue culture. Radiologically the bone involved is uniformally densed with or without minimal periosteal reaction [12]. It can be diaphyseal or metaphyseal (Figure 5a-d).
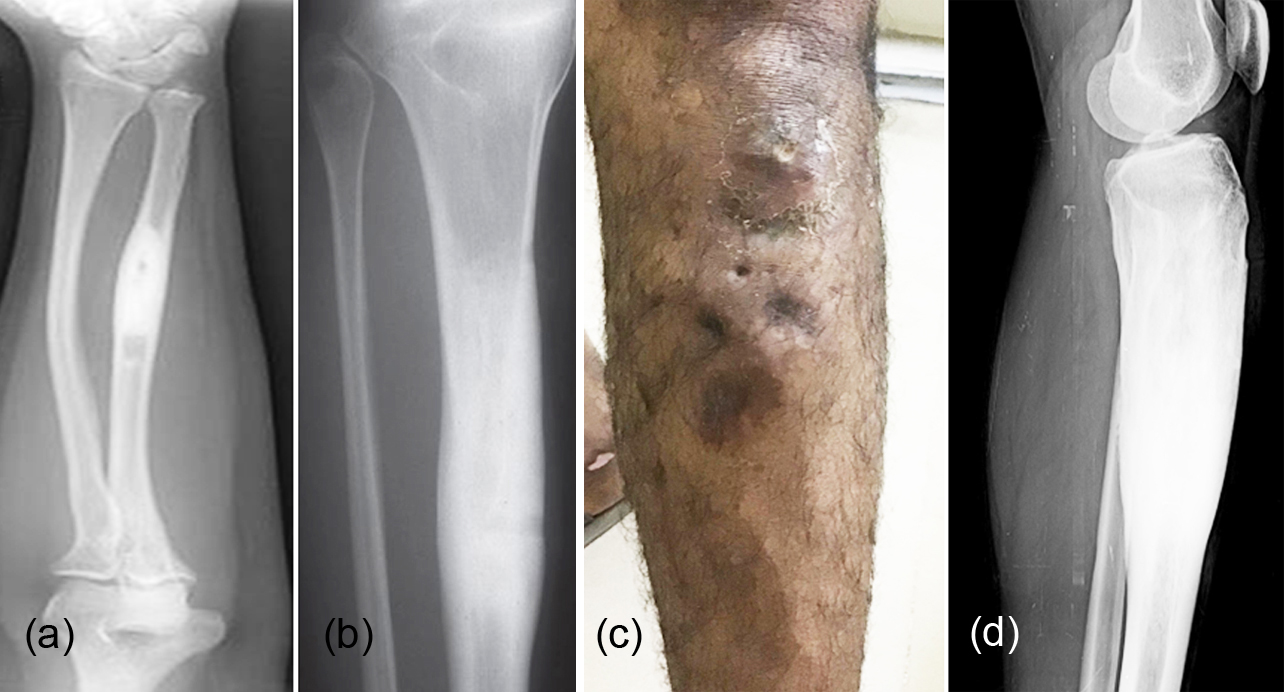
Figure 5: (a, b) Sclerosing osteomyelitis of Garre involving (a) mid shaft of radius, (b) mid shaft of tibia. (c, d): Garre’s type of osteomyelitis involving the proximal shaft of tibia, (c) clinical, (d) radiograph.
Idiopathic – Condensing osteitis, Osteitis condensans ilii
Condensing osteitis of the clavicle is a benign, often painful disorder, marked by bony sclerosis at the sternal end of the clavicle. Sclerosis of the inferomedial part of the medial end of the clavicle is noted (Figure 6a) [13].
Osteitis condensans ilii (OCI) is a benign cause of axial low back pain. Although no clear etiology has been identified, the prevailing theory is that mechanical strain affects the auricular portion of the ilium and causes premature arthritis. The location of the sclerosis has been traditionally confined to the ilium and may give the false impression of sacro-iliac joint involvement (Figure 6b) [14].
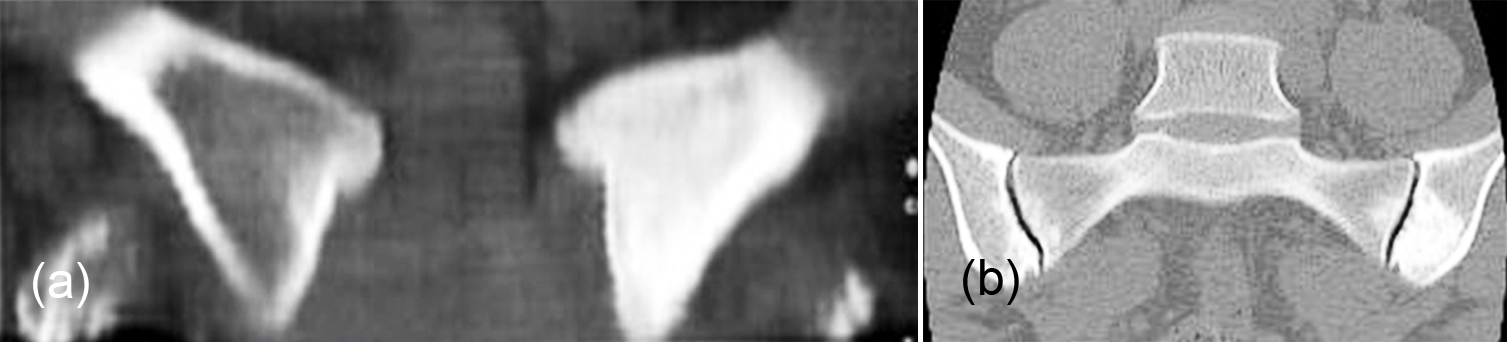
Figure 6: (a) Condensing osteitis of the left clavicle. (b): CT osteitis condensans ilii sclerosis of the inferior portion of the left iliac bone.
Neoplastic – Benign, malignant and metastatic
Benign bone lesions appearing as unifocal sclerotic lesion.
Osteoma
Osteoma is a benign bone tumor commonly encountered in skull and sinuses. Occasionally osteoma may be noted in the long bones also. These are painless benign tumors and the imaging characteristics vary from ivory dense to slightly trabeculated appearance [15].
Osteomas are frequently present in paranasal sinuses and occur in the frontal as well as the outer and inner tables of the skull (Figure 7a-c). Further imaging is not generally needed.
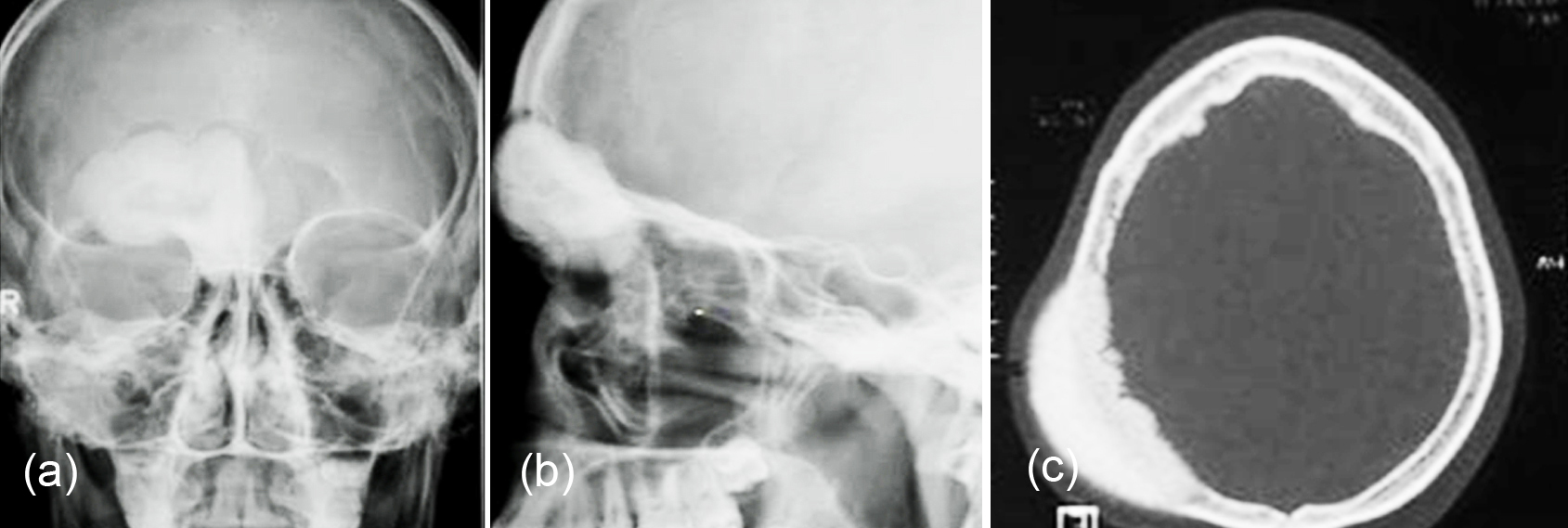
Figure 7: (a, b) Osteoma of the right frontal sinus. (c): CT osteoma of the skull.
Osteoid osteoma
Osteoid osteomas are benign bone-forming tumors that typically occur in children (Particularly adolescents). They have a characteristic lucent nidus less than 1.5 or 2 cm and surrounding osteosclerotic reaction, which classically causes night pain that is relieved by the use of salicylate analgesia, e.g. aspirin [16]. Although there is a lucent nidus in the lesion, it may be obscured by abundant reactive new bone (Figure 8a-e). CT/ MRI are essential to demonstrate the nidus (Figure 8f).

Figure 8: (a) Osteoid osteoma 3rd metacarpal. (b, c): Osteoid osteoma of the distal phalanx of the thumb, (d) thumb showing clubbing. (e): Osteoid osteoma femur, nidus is hidden by new bone. (f): CT Osteoid osteoma skull with nidus.
Osteoblastoma
Osteoblastoma has a nidus more than 2 cm in diameter and matrix may be heavily calcified (Figure 9a). The posterior elements of vertebra are commonly involved both in osteoid osteoma and osteoblastoma [17] (Figure 9b).
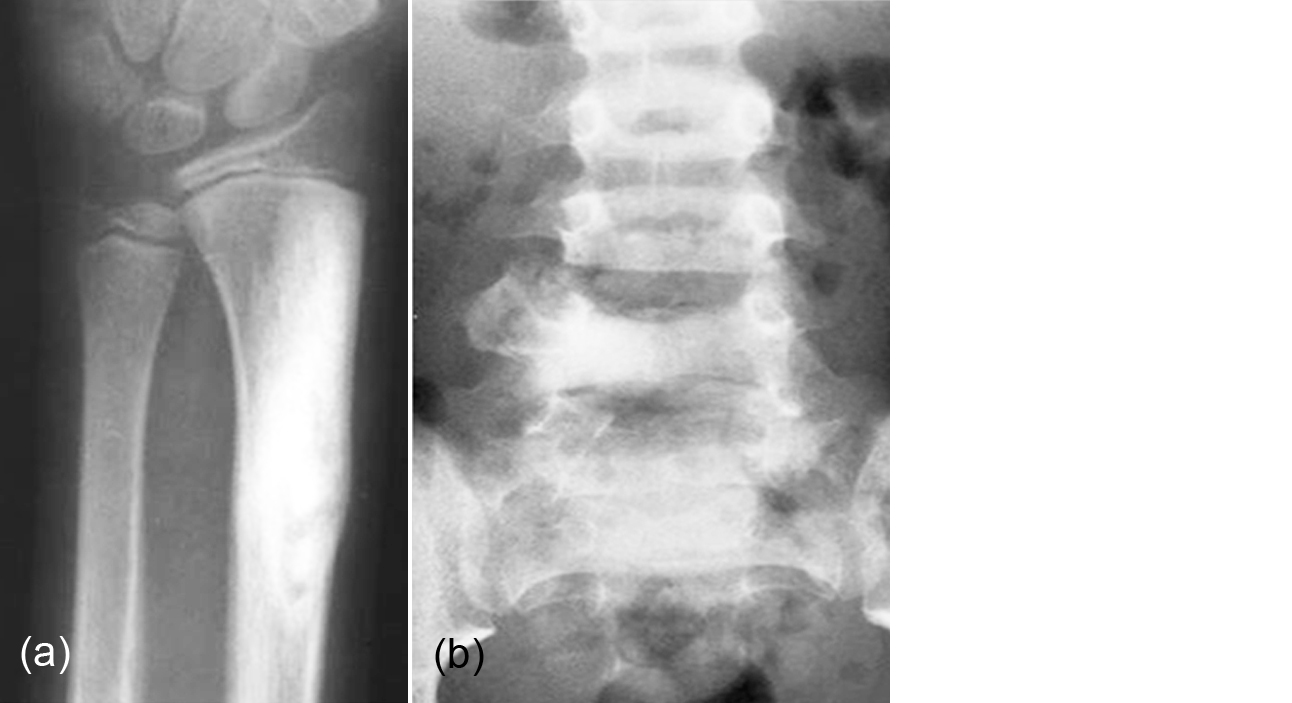
Figure 9: (a) Osteoblastoma involving the radius. (b): Osteoblastoma involving the right pedicle of L5.
Osteosarcoma
Osteosarcoma (OS) is a common primary malignant tumor of bone that produces osteoid matrix. Conventional OS is the most common subtype of OS and is readily identified at radiography as an intramedullary mass with immature cloudlike bone formation in the metaphyses of long bones. The most common radiographic appearance is expansile lytic bone lesion with coarsely thick or thin incomplete trabeculation (61% of cases). A dense sclerotic pattern is less common (<30% of cases). Variable rates of periosteal reaction (22%–50%) at radiography are also reported. Radiologically unifocal sclerotic lesion without periosteal new bone or soft tissue swelling is quite rare [18].
Malignant lesion of bone generally manifests as a predominantly sclerotic lesion except in telangiectatic osteosarcoma (Figure 10a, b).

Figure 10: (a) Osteosarcoma involving the proximal tibia. (b): Osteosarcoma involving the calcaneum.
Other malignant lesions of bone [2, 19]
Ewing’s sarcoma
Ewing’s sarcoma is a small cell sarcoma with heterogeneous appearance. A permeative lytic appearance with onion peel type of periosteal reaction is a common manifestation. However, purely sclerotic with ivory appearance also may be encountered (Figure 11a-c). In the latter instance differentiation from osteogenic sarcoma and lymphoma is difficult as all of them appear sclerotic.
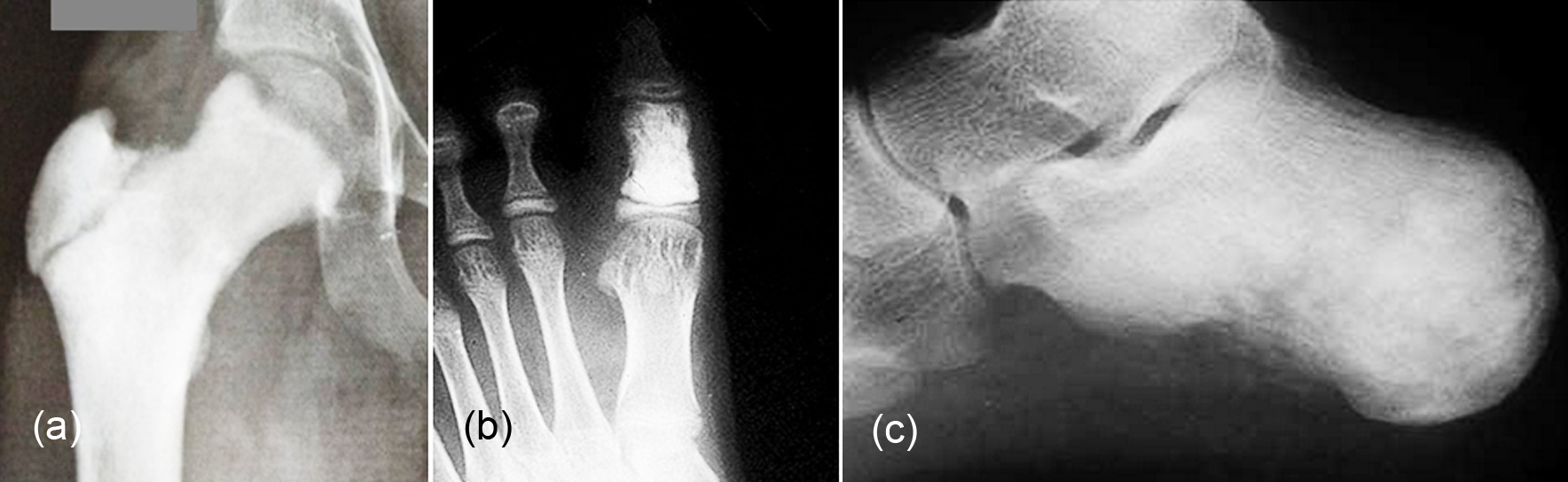
Figure 11: Ewing’s sarcoma involving (a) proximal femur, (b) proximal phalanx of great toe, and (c) calcaneum.
Lymphoma
Hodgkin’s lymphoma or other lymphomas may present as an isolated ivory focus more commonly in the spine (Figure 12) [20].

Figure 12: Hodgkin type of Lymphoma showing Ivory vertebra of L2.
Plasmacytoma
Plasmacytoma is a unifocal lesion of multiple myeloma. Plasmacytoma presenting as a unifocal sclerotic lesion is quite rare. In Poem Syndrome multiple lesions are noted associated with other clinical findings [21].
Metastasis
Unifocal sclerotic metastasis is quite rare but the presence of other lesions must be ruled out before mentioning that it is unifocal. Radiologically no specific characteristic is noted (Figure 13a-c), although they may be lytic, expansile, sclerotic and mixed. A primary lesion in prostate, breast, GI and GU tracks must be identified to say it is unifocal metastasis [2]. A PET CT scan is quite useful in making a proper diagnosis and identify the extent of lesions.
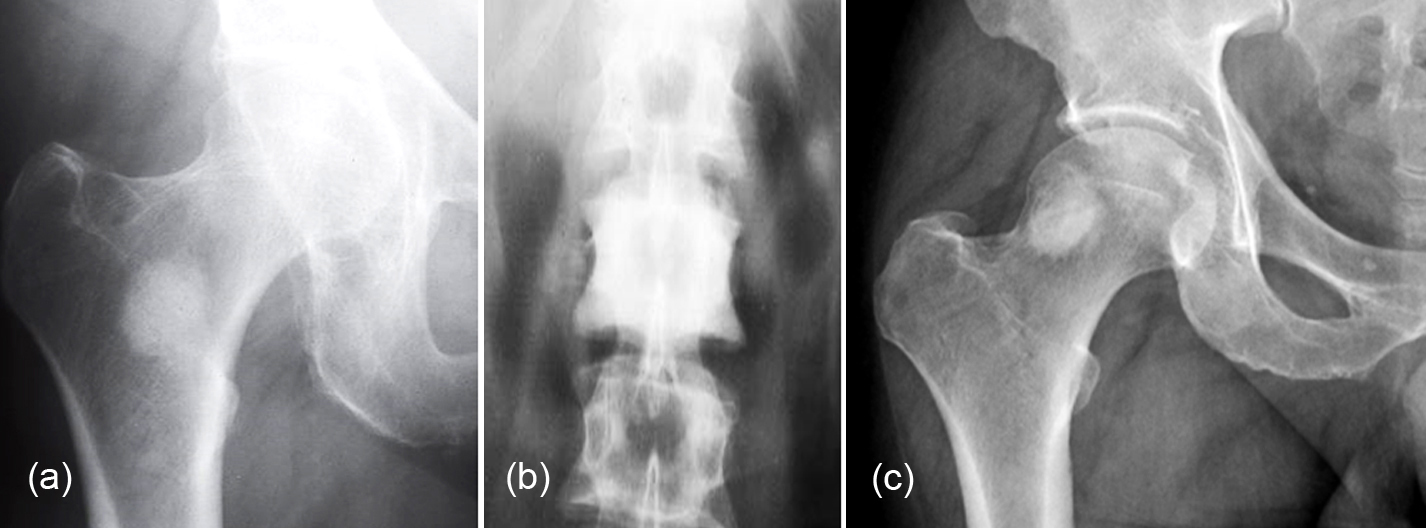
Figure 13: Metastasis from (a) Carcinoma breast, (b, c) Carcinoma of prostate.
Cartilaginous lesions
Enchondroma
The tumors arising from cartilage generally contain calcifications which are distinct with circular, arc like, nugget shapes. Occasionally a homogenous dense calcification is noted simulating a unifocal sclerotic lesion. Enchondroma when it is unifocal involves femur and other long tubular bones (Figure 14a, b). The hands are also common sites but heavy calcification is rare.
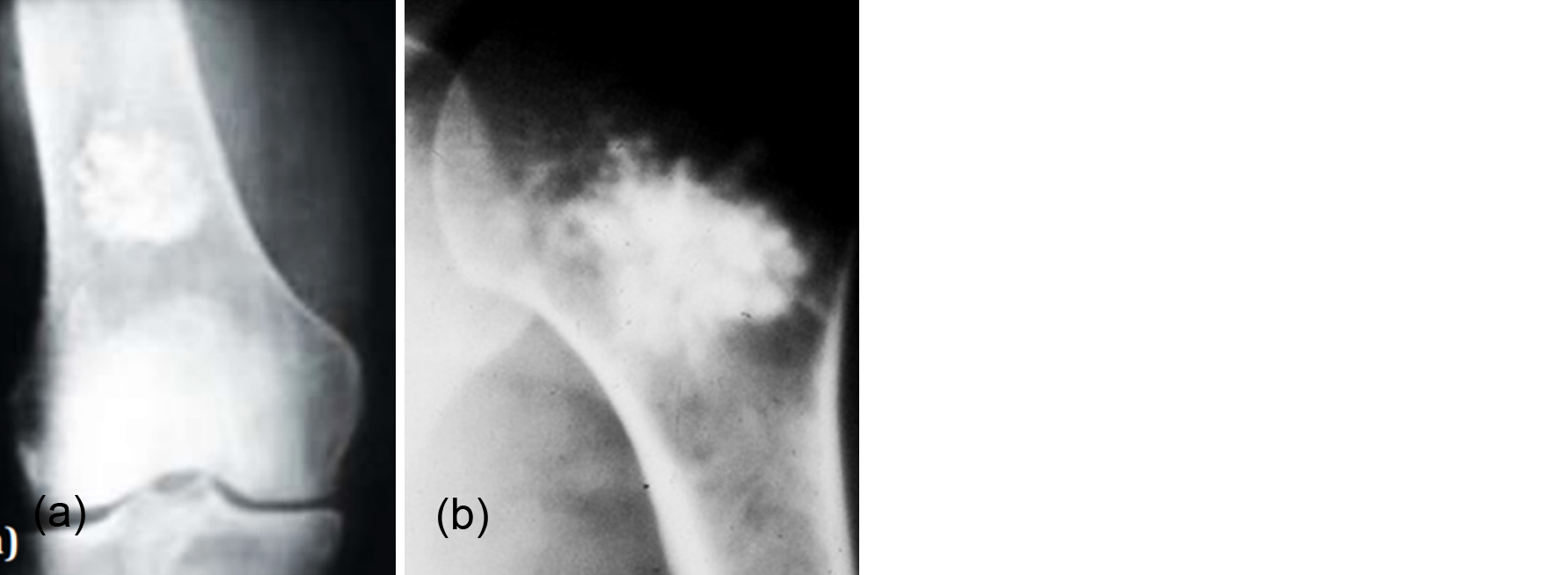
Figure 14: (a) Enchondroma lower end of femur. (b): Enchondroma of the humeral neck.
Healed fibrous lesions
Fibrous lesions of bone are generally not dense but healed non ossifying fibroma may show as a unifocal sclerotic lesion (Figure 15a-d). When they are limited to cortex and endosteum they may simulate enostosis (Figure 15e).
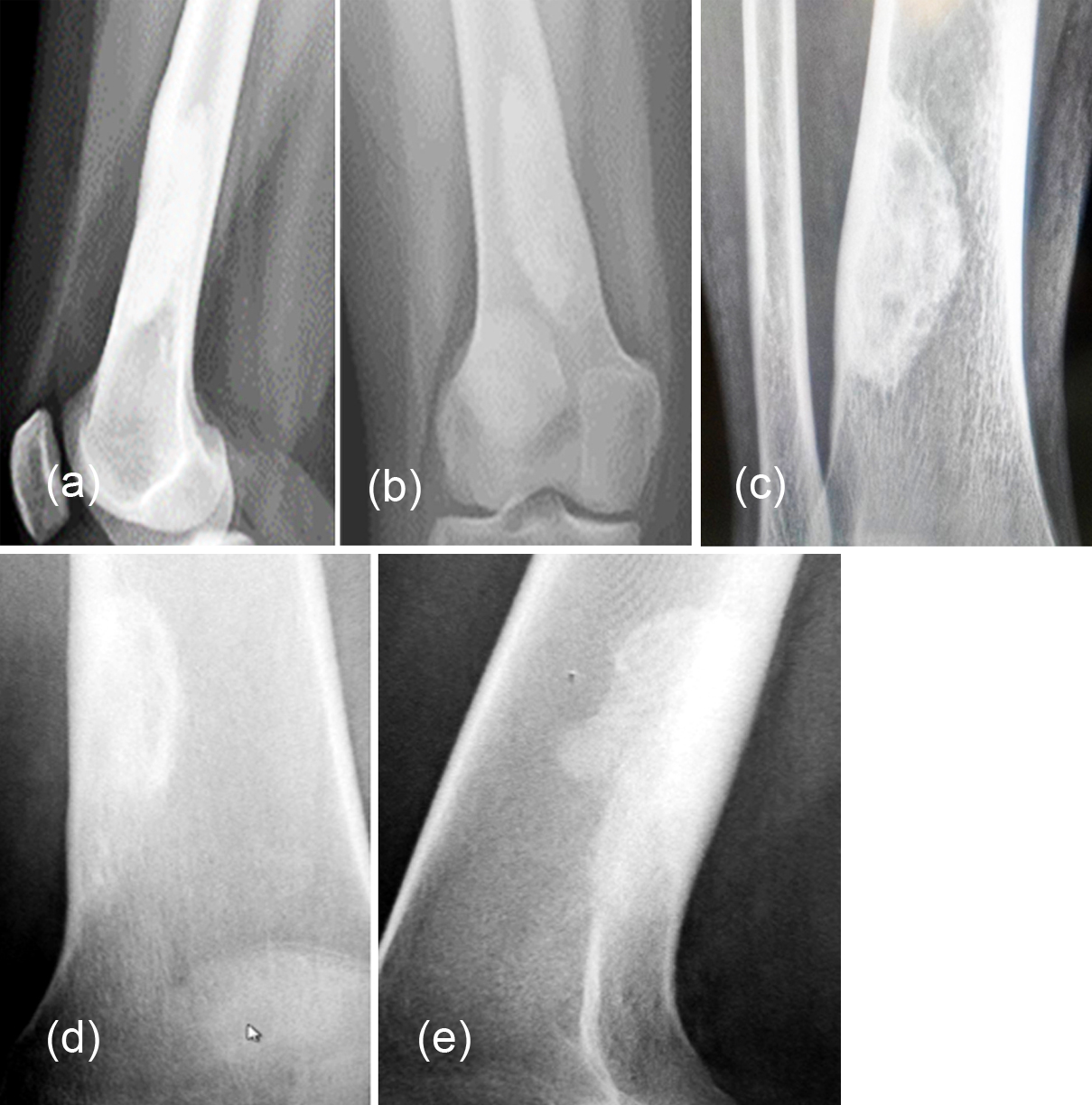
Figure 15: (a, b) Healed non ossifying fibroma. (c): Healing non ossifying fibroma lower end of tibia. (d, e): Healed non ossifying fibroma lower end of femur simulating enostosis.
Miscellaneous
Paget’s disease
Paget disease is rare but when present it may be lytic, lytic and sclerotic, and purely sclerotic. Radiologically a single Ivory vertebra is one of the manifestations of Paget (Figure 16a). Occasionally other single bones may be involved (Figure 16b) [22, 23].
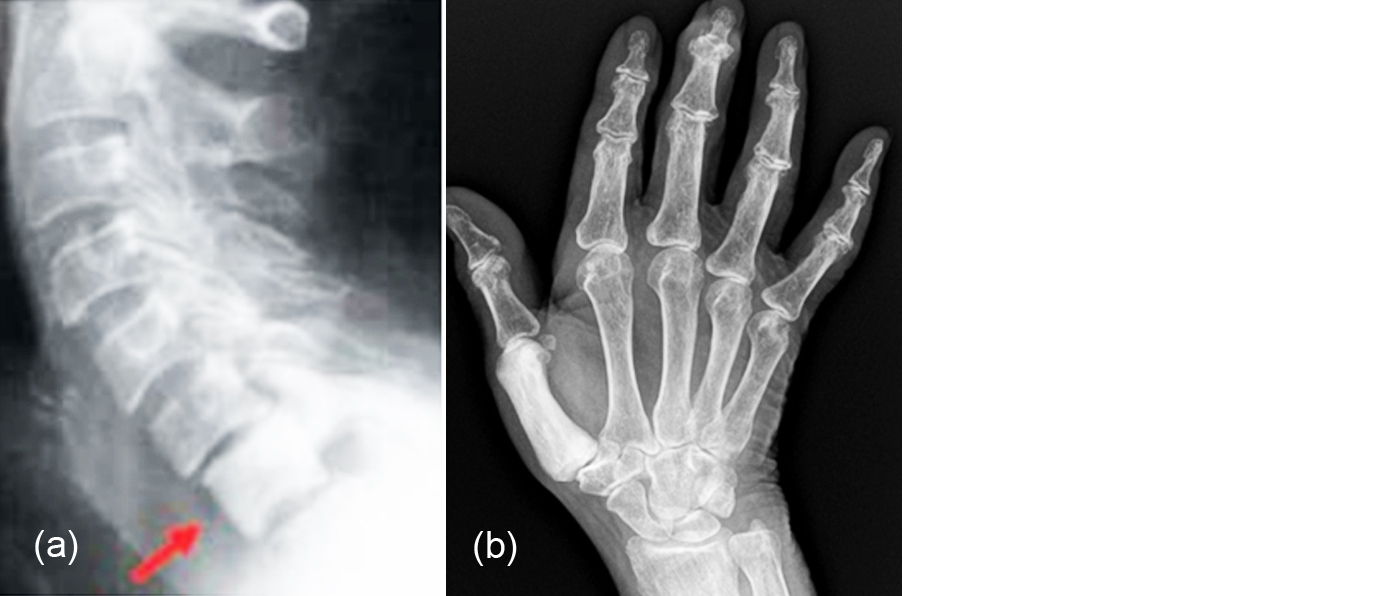
Figure 16: Paget disease involving (a) C7, (b) 1st metacarpal.
Healed brown tumors
Brown tumors of primary hyperparathyroidism may show sclerosis subsequent to parathyroidectomy (Figure 17ab). However, single brown tumor without other skeletal changes is quite rare [24].

Figure 17: (a) Brown tumor in hyperparathyroidism, (b) After parathyroid ectomy.
Conclusion
Unifocal sclerotic bone lesions constitute a wide spectrum of disorders. Conventional radiology is the initial imaging method and is best in making an early diagnosis. Radiological appearances of some of these lesions are similar but by analysis and with the help of clinical and laboratory studies, most of the lesions can be differentiated. Advanced imaging is quite unnecessary in most of the cases. However, the unifocality should be established by eliminating multiple lesions with the help of other imaging methods such as Spect CT and PET CT.
Acknowledgements
NIMS, KIMS, KREST Museum, Hyderabad, India.
Conflicts of interest
Author declares no conflicts of interest.
References
[1] Bell DJ, Niknejad MT. Focal sclerotic bony lesions (mnemonic). Accessed from: https://radiopaedia.org/articles/focal-sclerotic-bony-lesions-mnemonic
[2] Woude HJVD, Smithuis R. Sclerotic tumors. Accessed from: https://radiologyassistant.nl/musculoskeletal/bone-sclerotic-tumors-and-tumor-like-lesions
[3] Weerakkody Y, Gaillard F. Solitary sclerotic bone lesion. Accessed from: https://radiopaedia.org/articles/solitary-sclerotic-bone-lesion
[4] Greenspan A. Bone island (enostosis): current concept-A review. Skeletal Radiol. 1995; 24(2):111–115.
[5] Resnick D. Enostosis, hyperostosis, and periostitis. Bone and Joint Imaging. 2nd ed. Philadelphia, Pa: WB Saunders; 1996; pp.1211–1214.
[6] Gould CF, Ly JQ, Lattin GE, Beall DP, Sutcliffe JB. Bone tumor mimics: Avoiding misdiagnosis. Curr Probl Diagn Radiol. 2007; 36(3):124–141.
[7] Kransdorf MJ, Moser RP, Gilkey FW. Fibrous dysplasia. RadioGraphics 1990; 10:519–537.
[8] Kakarla S. Imaging in fibrous dysplasia, J Med Sci Res. 2013; 1(2):74–81.
[9] Carone L, Danesino GM, Pietrobono L, Corsico A, Bonardi M, et al. Bone healing: Radiology of normal and diseased bone. Accessed from: http://dx.doi.org/10.1594/ecr2017/C-1118
[10] Wilson ES, Katz FN. Stress fractures - An Analysis of 250 consecutive cases. Accessed from: https://doi.org/10.1148/92.3.481
[11] Kakarla S. Imaging of langerhans histiocytosis - Pictorial essay. J Med Sci Res. 2017; 5(1):33–39.
[12] Suma R, Vinay C, Shashikanth MC, Subba Reddy VV. Garre's sclerosing osteomyelitis. J Indian Soc Pedod Prev Dent. 2007; 25 Suppl:S30–S33.
[13] Greenspan A, Gerscovich E, Szabo RM, Matthews JG. Condensing osteitis of the clavicle: A rare but frequently misdiagnosed condition. AJR. 1991; 156:1011-1015.
[14] Mitra R. Osteitis condensans ilii. Rheumatol Int. 2010; 30(3):293–296.
[15] Bell DJ Gaillard F. Osteoma. Accessed from: https://radiopaedia.org/articles/osteoma
[16] Husseiny AE, Gaillard F. Osteoid osteoma. Accessed from: https://radiopaedia.org/articles/osteoid-osteoma
[17] Deng F, Weerakkody Y. Osteoblastoma. Accessed from: https://radiopaedia.org/articles/osteoblastoma
[18] Yarmish G, Klein MJ, Landa J, Lefkowitz RA, Hwang S. Imaging characteristics of primary osteosarcoma: nonconventional subtypes. Radiographics. 2010; 30(6):1653–1672.
[19] Mugera C, Suh KJ, Huisman TAGM, Weber K, Belzberg AJ, et al. Sclerotic lesions of the spine: MRI assessment. J Magn Reson Imaging. 2013; 38(6):1310–1324.
[21] Maruyama D, Watanabe T, Beppu Y, Kobayashi Y, Kim SW, et al. Primary bone lymphoma: A new and detailed characterization of 28 patients in a single-institution study. Jpn J Clin Oncol. 2007; 37(3):216–223.
[22] Voss SD, Murphey MD, Hall FM. Solitary osteosclerotic plasmacytoma: association with demyelinating polyneuropathy and amyloid deposition. Skeletal Radiol. 2001; 30(9):527–529.
[23] SMC, Gaillard F. Paget disease (bone). Accessed from: https://radiopaedia.org/articles/paget-disease-bone
[24] Kakarla S. Paget disease of skeleton – Pictorial essay. J Med Sci Res. 2014; 2(1):34–40.
[25] Xie C, Tsakok M, Taylor N, Partington K. Imaging of brown tumours: A pictorial review. Insights Imaging. 2019; 10:75.