Review
2019
December
Volume : 7
Issue : 4
Imaging spectrum of osteogenesis imperfecta – Pictorial essay
Subbarao Kakarla
Pdf Page Numbers :- 109-114
Subbarao Kakarla1,*
1Chairman, KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India
*Corresponding author: Prof. Kakarla Subbarao, MS, D.Sc. (HON), FRCR, FACR, FICP, FSASMA, FCCP, FICR, FCGP, Chairman, KIMS Foundation and Research Centre, Minister Road, Secunderabad - 500003, Telangana, India. Email: subbaraokakarla25@gmail.com
Received 2 July 2019; Revised 28 August 2019; Accepted 6 September 2019; Published 16 September 2019
Citation: Kakarla S. Imaging spectrum of osteogenesis imperfecta – Pictorial essay. J Med Sci Res. 2019; 7(4):109-114. DOI: http://dx.doi.org/10.17727/JMSR.2019/7-19
Copyright: © 2019 Kakarla S et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Osteogenesis imperfecta (OI) is a rare genetic disorder caused by the disturbance in the synthesis of Type I Collagen and is divided into several types. Severe form of OI, mainly type II can be diagnosed in utero by ultrasonography during the second trimester of pregnancy. All the other types viz. Type I to Type VIII are diagnosed by conventional radiography. Many authors have classified these into several types. This essay is not meant for a comprehensive review of these types. The main features include fractures, gracile bones, kypho scoliosis, deformities, and wormian bones in skull. These radiologic features are described pictorially.
Keywords: Osteogenesis Imperfecta; fragile bones; multiple fractures; osteopenia; pseudoarthrosis; wormian bones; hyperplastic callus
Full Text
Introduction
Osteogenesis imperfecta (OI) is a genetic disorder and is also known as fragilitas ossium. Armand, in 1716, reported a case of brittle bones of a new born infant. This is said to be the first recorded observation of this condition [1]. It is familial with an autosomal dominant mode of inheritance in many cases. Very few cases are reported to have autosomal recessive mode of inheritance. The quality and quantity of bone is diminished. The skeletal manifestations include a spectrum of findings including osteopenia, multiple fractures, wormian bones in skull, gracile and thinning of bones, bending deformities which are all described with the aid of radiographic images in the following paragraphs. This article deals with 8 types of OI and some of these are quite rare. Great confusion exists in the past and continues to exist in contemporary literature with reference to the classification of brittle and soft bones.
Imaging features & discussion (Figures 1-13)
The literature is replete with genetic causes and clinical basis of the diagnosis. The estimated incidence is approximately 1 in every 12,000-15,000 births. Osteogenesis imperfecta is the result of a mutation in one of the two genes that carry instructions for making type 1 collagen. Mutations in the COL1A1 and COL1A2 genes, which encode the α2 and α2 polypeptide chains 7, are responsible for more than 90% of all cases. The patient is generally referred for fractures or suspected OI with Blue Sclera. The imaging features although are classical of OI, it is impossible to correlate them with the types that have been described in the literature [3, 15-17]. Biphosphonate therapy [19, 20] is the choice in the treatment of OI. Corrections of deformities are done by surgery. The classical radiological features are listed in Table 1.
Table 1: Radiological findings.
|
· Osteopenia
· Multiple fractures
· Poorly mineralized skull (wormian bones) [4]
· Basilar impression [5]
· Otosclerosis
· Ribbon bones
· Hypercallosis
· Pseudoarthrosis
· Popcorn calcifications [12-14]
· Calcification of interosseous membrane - forearm
· Deformed pelvis – Protrusio acetabulum [8]
· Spondylolysis and spondylolisthesis [6, 7]
|
There are several synonyms for OI. These are listed in Table 2.
Table 2: Synonyms of OI.
|
· Van der Hoeve syndrome
· Trias fragilitas ossium
· Eddowe”s syndrome
· Osteopsathyrosis ideopathica of lobstein
· Ekman-Lobstein disease
· Osteogenesis imperfecta congenita
· Osteogenesis Type III lethalis
· Brittle bone disease
|
Classification by Sillence and Glorieux [2] is listed in Table 3.
Table 3: Classification by Sillence and Glorieux [2].
|
1. Type I (Mild)
· Autosomal dominant, most common, mild to moderate
· Fractures, minor deformities
· Almost natural stature
· Blue sclerae
· “Dentinogenesis imperfecta”may be present
2. Type II (Lethal)
· Autosomal recessive, lethal form.
· Fractures in utero
· Death before birth (respiratory deficiency)
3. Type III (Severe)
· Autosomal recessive, progressively deforming, compatible
· Fractures, kyphoscoliosis, major deformities
· Very small stature
· Triangular face; variable color of sclerae
· “Dentinogenesis Imperfecta”is frequent
4. Type IV (Moderate)
· Autosomal dominant, mildest, best prognosi
· Fractures
· Small stature
· Variable color of sclerae
· “Dentinogenesis imperfecta” may be present
|
Type V, VI, and VII have been added to the original classification system (no type I Collagen mutation, but abnormal bone on microscopy and similar phenotype). They are listed in Table 4.
Table 4: Original classification system (Type V, VI, and VII).
|
Type V [11]
· Fractures, Hyperplastic callus [9, 10], interosseous membrane ossification, metaphyseal dense lines
· Normal color of sclerae
· No “Dentinogenesis imperfecta”
Type VI
· Looser striations mimicking fractures
· No wormian bones
Type VII
· Fractures, coxa vara
· Normal color of sclerae
The imaging features are illustrated from head to foot.
|
Type I is mild and shows few features radiologically and is supported clinically by blue sclera (Picture 1).
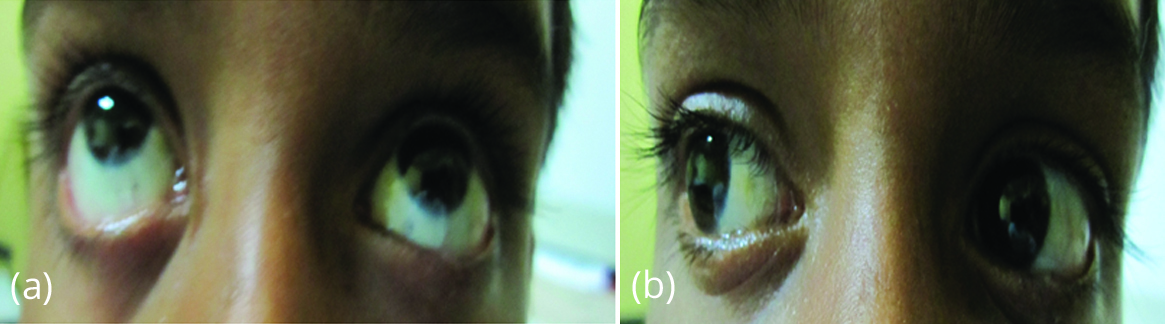
Picture 1: Blue sclera.
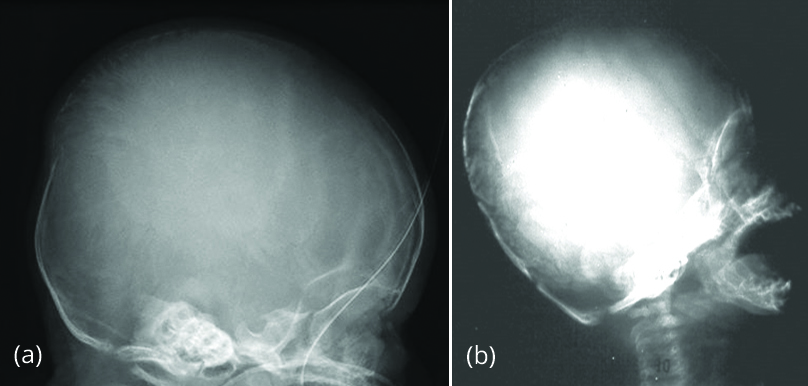
Figure 1: (a) Wormian bones [4], (b) basilar impression [5].
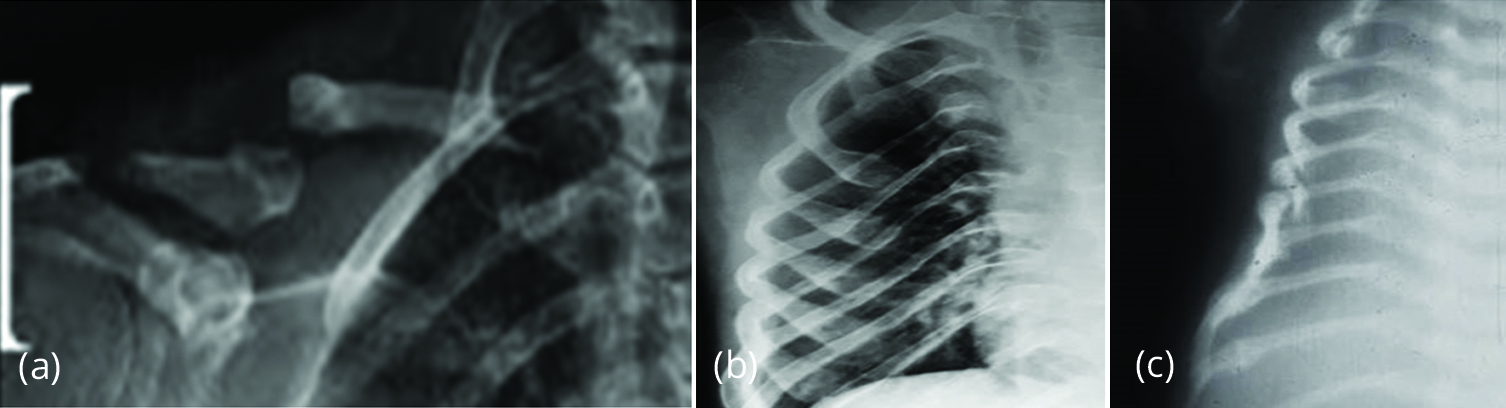
Figure 2: (a) Pseudoarthrosis clavicle, (b) Ribbon like thin ribs, (c) multiple fractures.

Figure 3: (a) Compression fractures of vertebrae and healing fractures of ribs at Costo vertebral junctions. (b) Compression fractures of vertebrae, (c) Spondylolisthesis L5-S1 [6, 7].
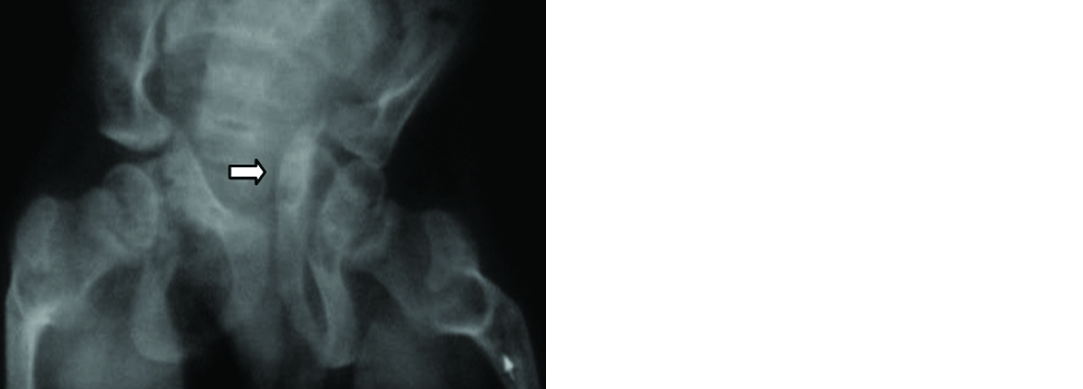
Figure 4: Deformed pelvis and protrusio acetabulae [8].
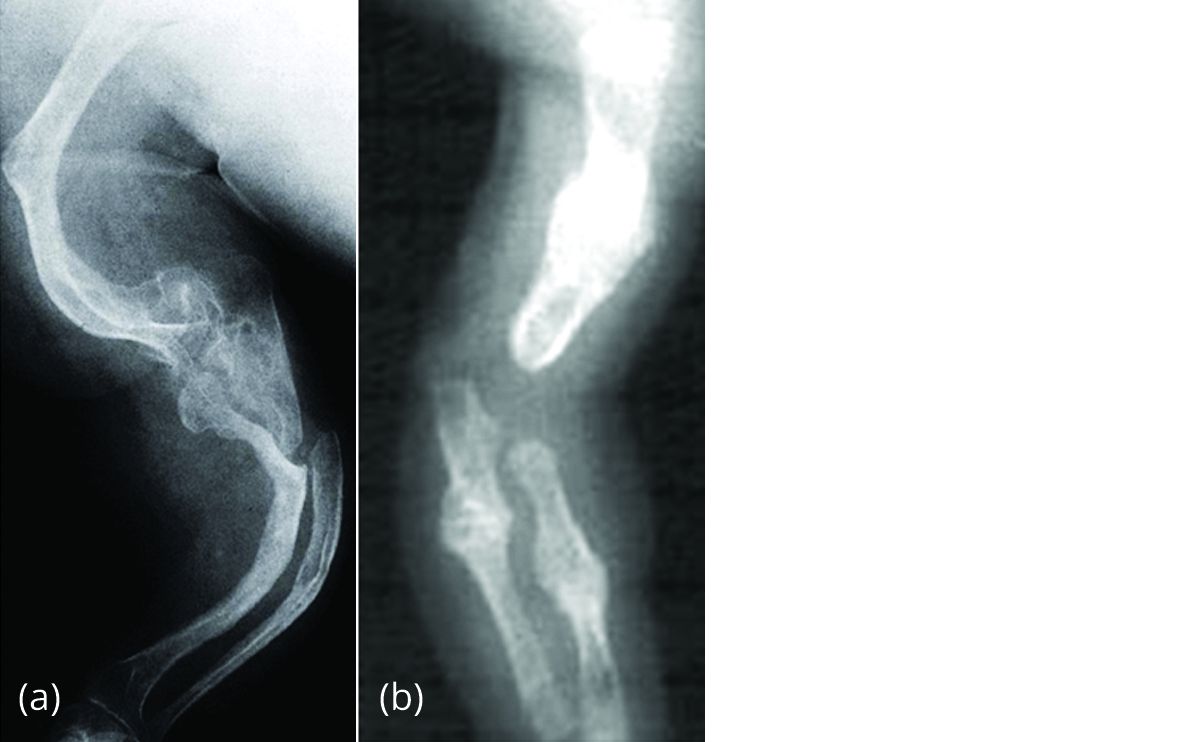
Figure 5a,b: Deformities and healing fractures of the bones of upper limb.

Figure 6a,b: Hypercallosis.

Figure 7a,b: Deformities and healed fractures of bones of forearm.

Figure 8a,b: Hypercallosis.

Figure 9a,b: Plastic bending of both femora.

Figure 10a,b: Pseudoarthrosis.
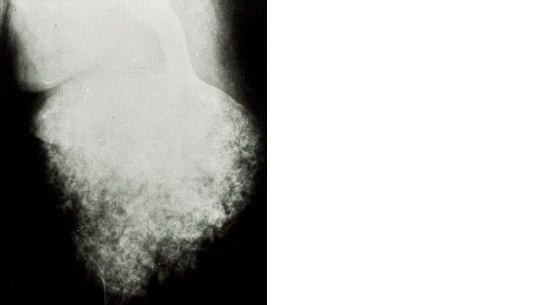
Figure 11: Popcorn calcifications [12-14].
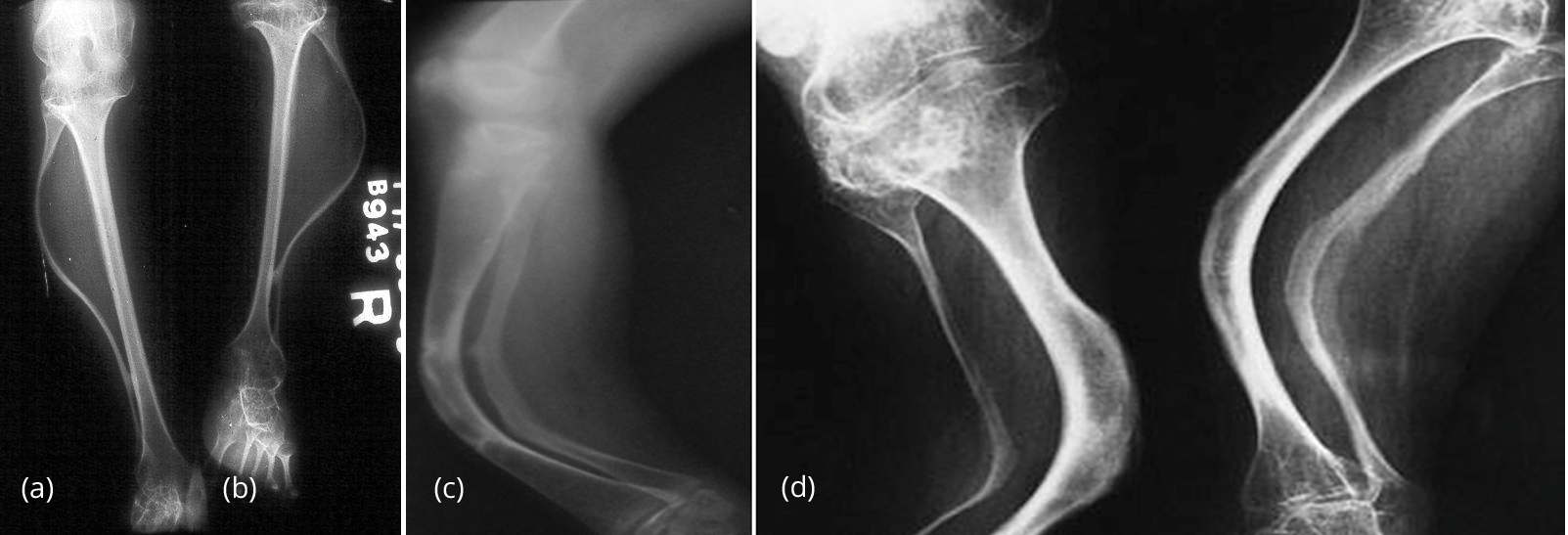
Figure 12: (a, b) Plastic bending of fibulae. (c, d): Plastic bending of both Tibia and Fibula.

Figure 13a,b,c: Bodygram with multiple fractures.
Bruck syndrome [18]
OI is associated with several syndromes including Bruck syndrome. It is a rare disorder characterized by association of OI and congenital joint contractures. They have white sclera. The fractures occur post natally and the contractures are the primary abnormality and not a complication of the fractures (Figure 14). Also has been reported Osteogenesis Sarcoma in association with OI.

Figure 14a,b: Bruck Syndrome with contractures of elbows.
Biphosphonate therapy has been introduced and proved to be effective in the treatment of OI (Figure 15). The proof of this is Zebra lines at the metaphyseal ends of long bones [19, 20].

Figure 15a,b: Bisphosphonate associated sclerotic bands - "Zebra lines".
Conclusion
Osteogenesis imperfecta is a rare congenital genetic disorder and several types of classifications have been described in the literature. The classical findings of OI include osteopenia, multiple fractures, poorly mineralized skull (wormian bones), ribbon bones, hypercallosis, pseudoarthrosis, popcorn calcifications, and spondlolisthesis. It is extremely difficult to categorize them into various types without clinical correlation and genetic testing.
Acknowledgements
NIMS, KIMS, KREST Museum, Hyderabad.
Conflict of interest
Author declares no conflict of interest.
References
[1] Bickel WH, Ghormley RK, Camp JD. Osteogenesis Imperfecta. Accessed from: https://doi.org/10.1148/40.2.145
[2] Glorieux FH. Osteogenesis Imperfecta. Best Pract Res Clin Rheumatol. 2008; 22(1):85-100.
[3] Wikipedia. Osteogenesis imperfecta. Accessed from: http://en.wikipedia.org/wiki/Osteogenesis_imperfecta
[4] Semler O, Cheung MS, Glorieux GH, Rauch F. Wormian bones in Osteogenesis Imperfecta: correlation to clinical findings and genotype. Am J Med Genet A. 2010; 152A:1681–1687.
[5] Charnas LR, Marini JC. Communicating Hydrocephalus, basilar invagination, and other neurologic features in Osteogenesis Imperfecta. Neurology. 1993; 43(12):2603–2608.
[6] Ivo R, Feuderer S, Eysel P. Spondylolisthesis caused by extreme pedicle elongation in Osteogenesis Imperfecta. Eur Spine J. 2007; 10:1636–1640.
[7] Htaz D, Esposito PW. Schroeder B, Burke B, Lutz R, et al. The incidence of Spondylolysis and Spondylolisthesis in children with Osteogenesis Imperfecta. J Pediatr Orthop. 2011; 31(6):655–660.
[8] Violas P, Fassier F, Hamdy R, Duhaime M, Glorieux FH. Acetabular protrusion in osteogenesis imperfecta. J Pediatr Orthop. 2002; 22(5):622–635.
[9] Dobrocky, Seidl G, Grill F. MRI and CT features of hyperplastic callus in osteogenesis imperfecta tarda. Eur Radiol. 1999; 9(4):665–668.
[10] Cheung MS, Azouz EM, Glorieux FH, Rauch F. Hyperplastic callus formation in Osteogenesis Imperfecta type V: follow-up of three generations over ten years. Skeletal Radiol. 2008; 37(5):465–467.
[11] Hui PK, Tung JY, Lam WW, Chau MT. Osteogenesis Imperfecta type V. Skeletal Radiol. 2011; 40(12):1633.
[12] Obafemi AA, Bulas DI, Troendle J, Marini JC. Popcorn calcification in Osteogenesis Imperfecta: incidence, progression, and molecular correlation. Am J Med Genet A. 2008: 146A(21):2725-2732.
[13] Snoeckx A, Vanhoenacker FM, Parizel PM. Popcorn calcifications in Osteogenesis Imperfecta. JBR-BTR. 2008; 91(4):176.
[14] Goldman AB, Davidson D, Pavlov H, Bullough PG. "Popcorn" calcifications: a prognostic sign in Osteogenesis Imperfecta. Radiology. 1980; 136(2): 351–158.
[15] Greenspan A. Orthopedic imaging, a practical approach. Lippincott Williams & Wilkins. 2004; ISBN: 0781750067.
[16] Renaud A, Aucourt J, Weill J, Bigot J, Dieux A, et al. Radiographic features of osteogenesis imperfect. Insights Imaging. 2013; 4(4):417–429.
[17] Imaging in Osteogenesis Imperfecta. Accessed from: https://emedicine.medscape.com/article/411919-overview
[18] Viljoen D, Versfeld G, Beighton P. Osteogenesis imperfecta with congenital joint contractures (Bruck Syndrome). Clin Genet. 1989; 36(2):122–126.
[19] Dwan K, Phillipi CA, Steiner RD, Basel D. Bisphosphonate therapy for osteogenesis imperfecta. Cochrane Database Syst Rev. 2014; 23(7):CD005088.
[20] Grisson LE, Harcke HT. Radiographic features of biphosphonates therapy in pediatric patients. Pediatr Radiol. 2003; 33(4):226–229.