Original Research
2014
June
Volume : 2
Issue : 2
Quality assurance of modern image guided 3D-conformal radiotherapy treatments
Krishnamurthy K, Anandagiri Babu A, Prasad PBLD, Kavi Arasu K
Pdf Page Numbers :- 57-61
Krishnamurthy K1,*, Anandagiri Babu A1, Prasad PBLD1 and Kavi Arasu K1
1Department of Radiation Oncology, Advanced Cancer Centre, Krishna Institute of Medical Sciences, Secunderabad-500003, AP., India.
*Corresponding author: Dr. K. Krishnamurthy, 1Department of Radiation Oncology, Advanced Cancer Centre, Krishna Institute of Medical Sciences, Secunderabad-500003, AP., India. Email: kammarikm@yahoo.co.in
Received 18 January 2014; Revised 6 March 2014; Accepted 14 March 2014
Citation: Krishnamurthy K, Anandagiri Babu A, Prasad PBLD, Kavi Arasu K (2014) Quality assurance of modern image guided 3D-conformal radiotherapy treatments. J Med Sci Res 2(2):57-61. DOI: http://dx.doi.org/10.17727/JMSR.2014/2-011
Copyright: © 2014 Krishnamurthy K et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: To describe the Quality Assurance (QA) methods of modern Three-dimensional conformal radiotherapy (3DCRT) treatments such as image guided Intensity-modulated radiation therapy (IMRT), RapidArc, Stereotactic radiosurgery (SRS)/ Stereotactic fractionated radiation (SRT) to ensure quality of treatments delivered to cancer patients.
Materials and methods: 3D-RFA and Ionisation chambers were used for the machine specific QA. Imatrixx-2D array with locally fabricated phantom and another locally fabricated spherical phantom with ionization chambers is used for relative and absolute QA respectively. Electronic Portal Imaging Devices and Epiqa software is used for the QA with portal dosimetry. Varians Eclipse and Brainlab’s Iplan treatment planning systems were used for treatment plans and dose calculations. For relative dosimetry the planar dose matrices are analysed using global Gamma Index criteria of 3mm distance to agreement (DTA) and 3% dose difference. The QA of Machines and patient treatments were carried out using national and international protocols.
Results: The maximum deviations of percentage of dose points in which γ>1 are 1.98 in relative dosimetric QA and 1.5 for absolute QA in the delivery of IMRT, RapidArc and SRS/SRT treatments. The mean deviations and Standard deviation (SD) values are less in portal dosimetry than that of phantom studies in relative dosimetry and all the absolute dose deviations are less than that of relative dose deviations.
Conclusion: The results of machine specific QA as well as relative and absolute dosimetric QA of patient treatments are well within the acceptable limits of values mentioned in the national and international protocols. The study ensures the accuracy and quality of the treatments delivered to the patients at our oncology center.
Keywords: Quality assurance, RapidArc, Portal dosimetry, Gamma index, Image guided radiotherapy
Full Text
Introduction
Machine specific and patient specific quality assurance of radiotherapy treatment is an essential part of clinical practice to know the quality of radiotherapy given to patients. Implementation of a comprehensive quality assurance program evaluates the tolerance limits and ensures adequate level of quality of treatment delivered to patients. The image guided IMRT, RapidArc and intensity-modulated stereotactic radiosurgery (IMSRS)/ SRT treatments are known as modern and novel techniques in which either fixed or rotational fields are used in the treatments. During the delivery of these treatments the multileaf collimators (MLC’s) move dynamically while the gantry may either fixed or rotated continuously with different dose rates [1]. In view of potential sources of errors as well as inaccuracies are involved in various stages of implementation of these treatments, the World Health Organisation (WHO) [2] emphasized the need for QA for execution of radiotherapy. With advent of these latest treatment delivery techniques, recent clinical reviews recommended accuracies within ±3.5 in dose delivery [3]. The complex nature of these modern treatments needs a precise machine and patient specific QA to verify whether the intended dose is delivered as planned in each treatment and ensure accurate treatment. Various methods involved and results obtained in the quality assurance procedures of modern radiotherapy treatment delivery are reported by various authors [4-10]. In our clinical setup to carryout machine specific QA and pre treatment patient specific QA, we have used various types of dosimetric QA equipment for a retrospective study. In this study measurements are performed using; 1) Linac mounted EPIDs (aS-1000) with Portal dose prediction and Epiqa (GLAaS) software, 2) Imatrixx-2D array (IBA Dosimetry Gmbh, Germany) with locally fabricated acrylic phantom and Omnipro ImRT software and 3) A locally fabricated acrylic Spherical phantom with Ionisation chambers (IBA Dosimetry Gmbh, Germany). The purpose of this study is to validate our treatments with different QA methods and check the accuracy of the treatments delivered to the patients. This paper highlights and provides information regarding the QA procedures followed and results obtained in the delivery of the modern radiotherapy treatments.
Materials and methods
The details of dosimetric QA equipment used and procedures of measurements done are given in the following sections.
A) Machine specific QA with 3D-RFA and Ionisation chambers: The daily, weekly, monthly, quarterly, half yearly and annual QA of the machines is carried out using the 3 dimensional Radiation Field Analyser(RFA) and various types of Ionisation chambers as per the protocols of the Institute, which are formed on the basis of the national and international protocols. The equipment used for these QA tests are shown in figure 1.
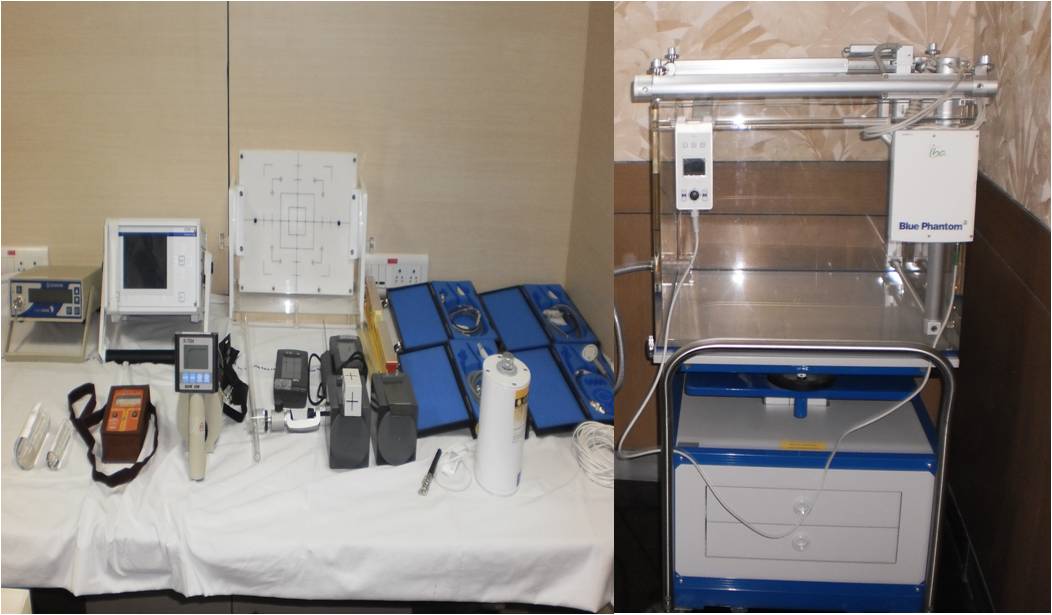
Figure 1: Dosimetric equipment used in Machine Specific Quality Assurance.
B) Portal dose prediction with EPID: Forty five verification plans each of fifteen IMRT, RapidArc and SRS/SRT treatments were created using portal dose prediction software and delivered them on the Linac mounted Electronic Portal Imaging Device (EPID). The EPID is a flat panel detector with 1024 x 768 amorphous silicon detectors of size 0.39 x 0.39 mm2. The setup of a typical RapidArc treatment delivery on EPID without keeping any phantom in between is shown in figure 2. The treatment planning system (TPS) calculated and EPID measured planar dose matrices are analysed with Epiqa software and compared the results.
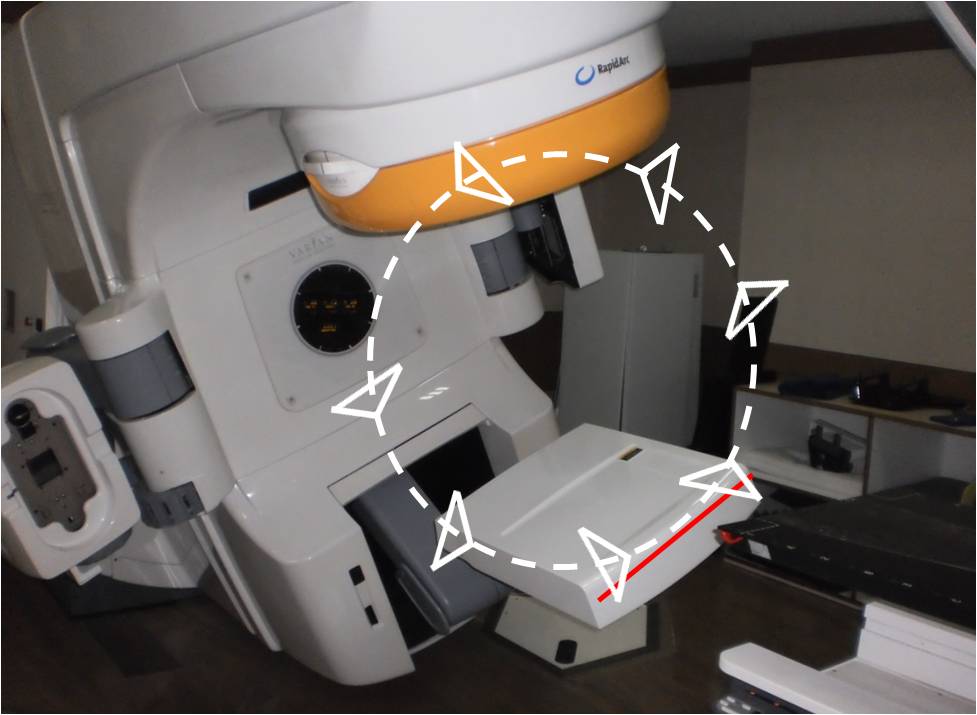
Figure 2: RapicArc verification plan delivery method on EPID in portal dosimetry.
C) Imatrixx evolution-2D array with locally fabricated phantom: Forty five verification plans each of fifteen IMRT, RapidArc, SRS/SRT were created and delivered on the IBA-Imatrixx-2D array embedded Phantom. The IBA-Imatrixx-2D array contains 1024 air vented pixel ionization chambers of size 4.5 (dia) x 5 (h) mm with a volume of 0.08cm3. The setup for measurement of a verification plan on the phantom is shown in figure 3. Omnipro ImRT software is used to compare and analyse the TPS calculated and phantom measured dose planes.

Figure 3: Setup arrangement of Imatrixx-2D array phantom for relative dosimetry
D) Acrylic Spherical Phantom with ionization chambers: All the 45 verification plans were delivered on the locally fabricated Spherical phantom. The CC-13 and CC-01 Ionisation chambers were used to measure the absolute doses. The measurement setup is showed in Figure 4. The TPS calculated and measured doses were compared and the results were shown in Table 1.

Figure 4: Setup arrangement of Spherical phantom for absolute dosimetry
Results
The calculated and measured planar relative dose distributions and absolute central axis (CAX) point doses are compared with profiles/isodose matching methods using their respective software’s. The 3mm DTA and 3% dose difference for the global Gamma Index (γ≤1) and 97 % data pass criteria is used for the analysis and the results obtained were presented. The planar dose evaluation of a typical RapidArc plan done with portal dose prediction and Epiqa software is shown in figure 5. The evaluation of planar dose matrix of another typical RapidArc plan done with Imatrixx-2D array phantom and Omnipro Imrt software is shown in figure 6.
The planar dose evaluation of a verification plan with the percentage of points falling outside of passing criteria(3% & 3mm) which are defined by γ>1 of 45 patients along with maximum, mean and SD values obtained from the analysis is shown in table 1. The mean and SD values are less in portal dosimetry than that of Imatrixx-2D array phantom studies in relative dosimetry. All the forty five treatments have shown less dose deviations in absolute dosimetric measurements than that of relative dosimetry.
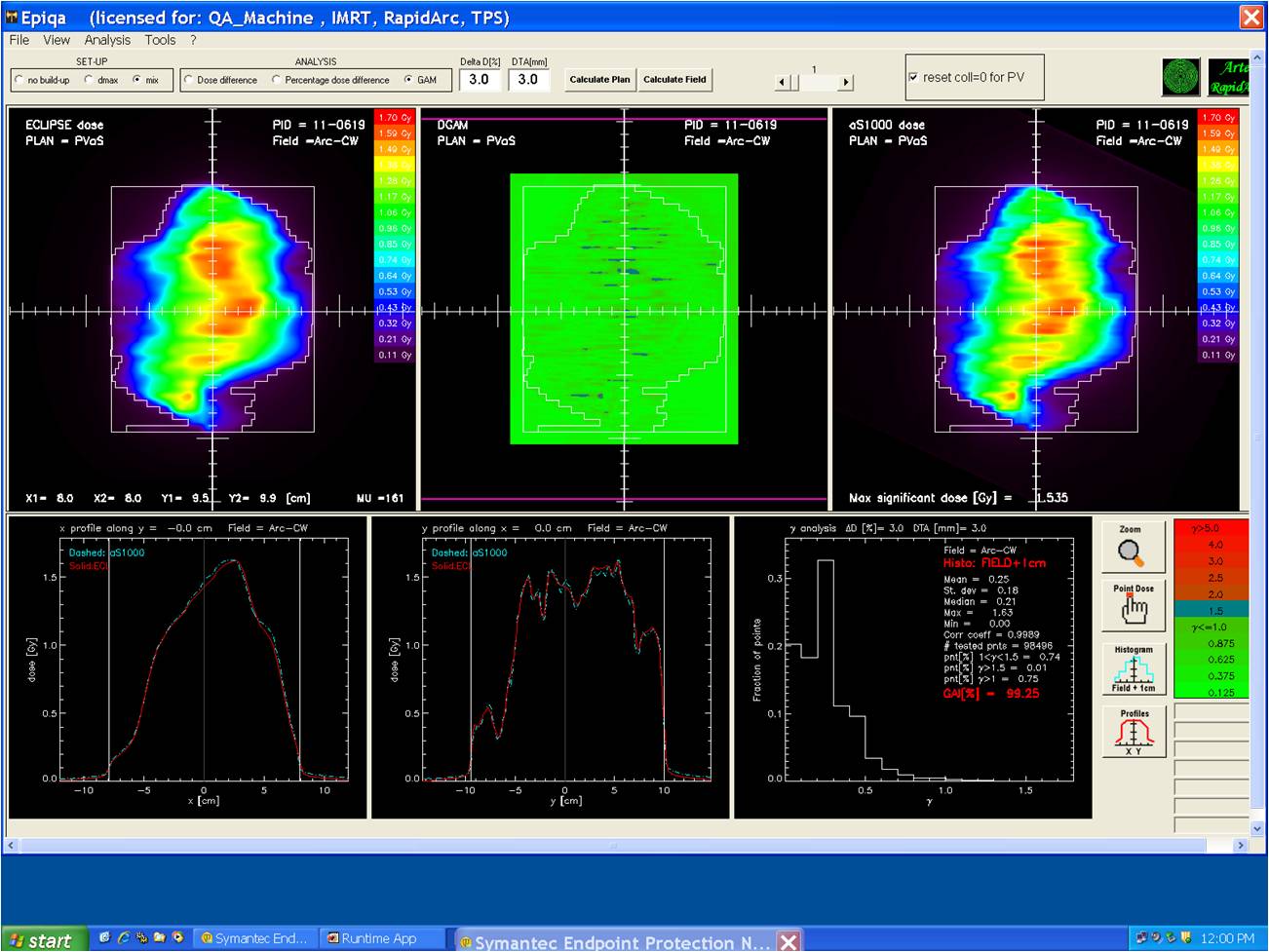
Figure 5: Comparision of calculated and measured planar dose distributions of a typical RapidArc plan with Portal dosimetry
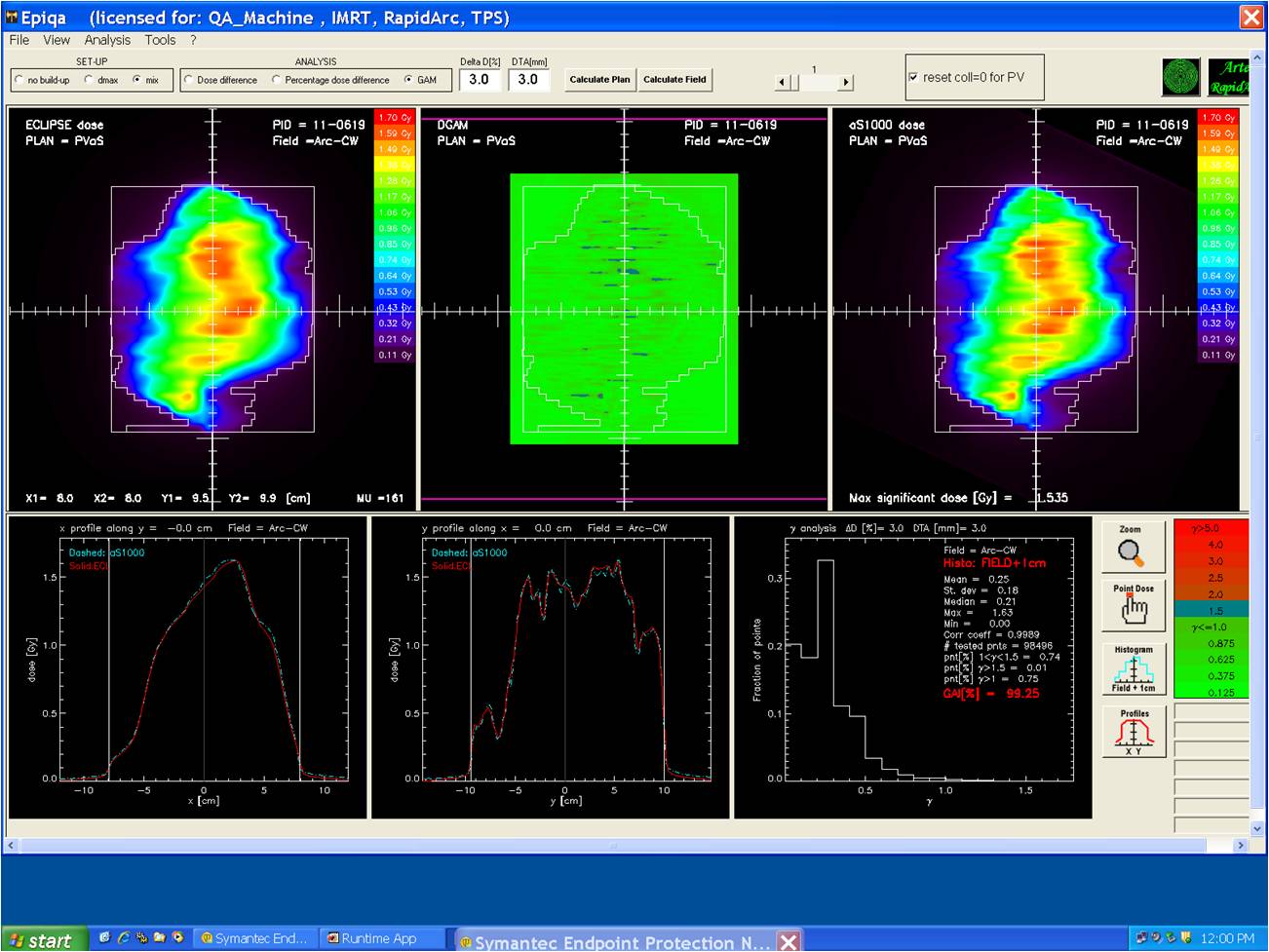
Figure 6: Comparison of calculated and measured planar dose distributions of a typical RapidArc plan with Imatrixx-2D array phantom.
Table 1: Percentage of dose deviations for 45 verification plans of three dosimetric systems
|
Verification
Plan No.
|
Imatrixx-2D array Phantom
Relative Dosimetry
|
Portal Dosimetry
with EPID
Relative Dosimetry
|
Acrylic Spherical
Phantom
Absolute Dosimetry
|
|
% of planar dose deviations
(γ>1)
|
% of planar dose deviations
(γ>1)
|
% of CAX dose
deviations
|
|
IMRT Plans
|
Rapid-Arc Plans
|
SRS/ SRT Plans
|
IMRT Plans
|
Rapid-Arc Plans
|
SRS/ SRT Plans
|
IMRT Plans
|
Rapid-Arc Plans
|
SRS/ SRT Plans
|
|
1
|
1.82
|
1.52
|
1.22
|
1.67
|
1.25
|
1.55
|
1.30
|
1.10
|
0.80
|
|
2
|
1.54
|
1.15
|
1.90
|
1.19
|
1.15
|
1.30
|
1.20
|
0.75
|
1.10
|
|
3
|
1.20
|
1.75
|
1.12
|
1.46
|
1.75
|
1.70
|
1.10
|
0.85
|
0.90
|
|
4
|
1.87
|
1.90
|
1.40
|
1.35
|
1.32
|
1.10
|
0.90
|
1.50
|
0.80
|
|
5
|
1.78
|
1.25
|
1.50
|
1.650
|
1.54
|
1.94
|
1.20
|
1.22
|
1.30
|
|
6
|
1.75
|
1.15
|
1.20
|
1.80
|
1.25
|
1.30
|
1.30
|
1.10
|
1.30
|
|
7
|
1.51
|
1.65
|
1.90
|
1.61
|
1.12
|
1.45
|
1.20
|
1.32
|
1.20
|
|
8
|
1.80
|
1.95
|
1.76
|
1.74
|
1.72
|
1.56
|
1.40
|
0.75
|
0.80
|
|
9
|
1.20
|
1.35
|
1.89
|
1.58
|
1.05
|
1.74
|
1.20
|
0.85
|
1.20
|
|
10
|
1.90
|
1.40
|
1.90
|
1.42
|
1.64
|
1.72
|
1.10
|
1.14
|
0.90
|
|
11
|
1.25
|
1.35
|
1.75
|
1.10
|
1.76
|
1.71
|
0.80
|
1.32
|
1.40
|
|
12
|
1.65
|
1.84
|
1.94
|
1.18
|
1.54
|
1.40
|
1.20
|
1.28
|
0.80
|
|
13
|
1.45
|
1.38
|
1.36
|
1.20
|
1.42
|
1.02
|
0.90
|
1.28
|
1.30
|
|
14
|
1.85
|
1.45
|
1.25
|
1.76
|
1.22
|
1.54
|
1.40
|
1.14
|
1.40
|
|
15
|
1.98
|
1.72
|
1.49
|
1.27
|
1.34
|
1.32
|
1.25
|
1.18
|
0.95
|
|
Maximum
|
1.98
|
1.95
|
1.94
|
1.80
|
1.76
|
1.94
|
1.40
|
1.50
|
1.40
|
|
Mean
|
1.64
|
1.52
|
1.57
|
1.47
|
1.40
|
1.49
|
1.16
|
1.12
|
1.08
|
|
SD
|
0.25
|
0.26
|
0.29
|
0.23
|
0.23
|
0.25
|
0.17
|
0.22
|
0.23
|
Abbreviations: Gamma Index criteria= 3mm DTA and 3% dose difference; SD= standard deviation.
Discussion
A retrospective investigation on technical and QA data from the 45 treatment plans were performed to provide evidence about delivery features and accuracy of modern radiotherapy treatments. All the machine specific QA tests have passed the tolerance limits of the protocols. The forty five verification plans created for their quality assurance study have passed the gamma evaluation criteria. The results show that, overall, minimal differences exist between the methods. The portal dose prediction with EPID and Epiqa software method is a less time-and material consuming system and yet given minimal deviations. This may be due to the type and more number of closely placed detectors and accuracy of the EPID setup during the treatment delivery.
In the Imatrixx-2D Array phantom method, it requires gantry correction device known as inclinometer in rotational type RapidArc treatments for patient specific QA as reported by earlier authors [11, 12]. The density effect of locally fabricated acrylic phantom is not considered since the plan is both created and verified with the same phantom, which makes the interpretation of results quite straightforward. All the methods used for the measurements taken were subject to similar set-up uncertainties. We have used 2.5mm grid size in all verification plans calculations for the uniformity in the comparisons. The mean deviations and SD values are lower in the portal dosimetry compared to that of phantom studies in relative dosimetry. The measured absolute dose values at the central axis point of all the plans with the three methods are well in agreement with the TPS predicted values and the maximum deviation found was <1.5%.
The number of plans in which γ>1 values are less in portal dosimetry than that of phantom studies as shown in table 1. The less deviations in portal dosimetry is attributed to closely embedded chambers and their directional dependence in the EPID compared to that of the distance between the chambers placed in Imatrixx 2D-Array as reported in our earlier paper [13]. The present results of our portal dosimetry are comparable with the earlier reported values by others [14-16]. The present phantom studies dosimteric QA results are similar to the summaries provided by other groups using different phantoms and independent dosimetric tools [17-19].
Conclusions
The retrospective study on machine and patient specific quality assurance has shown the probable uncertainties and errors in dose delivery of modern radiotherapy treatments. The results revealed that all the dosimetric QA methods are suitable for the patient specific QA of IMRT, RapidArc and SRS/SRT treatments. The study confirmed that the observed deviations were well within the limits of international standards and ensured the high-level of confidence in the accuracy and quality of the treatments delivered at our oncology center. The study helped us in understanding various QA procedures and provide guidance to improve the work practices of the department.
Acknowledgements
We thank the MD & CEO of the Institute for the encouragement in this work and we extend our sincere thanks to all fellow Radiation Oncologists and Medical Physicists of the department, who has shown keen interest and extended their help in carrying out this study.
Conflict of interest
The authors declare that they have no conflict of interest.
References
1. LoSasso T, Chui CS, Ling CC. Comprehensive quality assurance for the delivery of intensity modulated radiotherapy with a multileaf collimator used in the dynamic mode. Med Phys. 2001; 28(11):2209-2219.
2. World Health Organistion (WHO). Quality assurance in radiotherapy. Geneva: WHO, 1988.
3. Wambersie A, Van Dam J, Hanks G et al. What accuracy is needed in dosimetry? IAEA-TECDOC 1994; 734:11-35.
4. Ezzell GA, Burmeister JW, Dogan N, LoSasso TJ, Mechalakos JG, et al. IMRT commissioning: multiple institution planning and dosimetry comparisons, a report from AAPM Task Group 119. Med Phys. 2009; 36(11):5359-73.
5. Klein EE, Joseph Hanley, John Bayouth et al. Task Group 142 Report: Quality assurance of medical linear accelerators. Med Phys. 2009; 36(9):4197–4212.
6. Yu CX, Tang G. Intensity-modulated arc therapy: principles, technologies and clinical implementation. Phys Med Biol. 2011; 56(5):R31-54
7. Van Esch A, Huyskens DP, Behrens CF, Samsoe E, Sjolin M, et al. Implementing RapidArc into clinical routine: a comprehensive program from machine QA to TPS validation and patient QA. Med Phys. 2011; 38(9):5146-5166.
8. Schreibmann E, Dhabaan A, Elder E, Fox T. Patient-specific quality assurance method for VMAT treatment delivery. Med Phys. 2009; 36(10):4530-4535.
9. Ravichandran R, Bhasi S, Binukumar JP, Davis CA. Need of patient-specific quality assurance and pre-treatment verification program for special plans in radiotherapy. J Med Phys. 2011; 36(3):181-183
10. Solberg TD, Balter JM, Benedict SH, Fraass BA, Kavanagh B, et al. Quality and safety considerations in stereotactic radiosurgery and stereotactic body radiation therapy: Executive summary. Pract Radiat Oncol. 2012; 2(1):2-9.
11. Herzen J, Todorovic M, Cremers F, Platz V, Albers D, et al. Dosimetric evaluation of a 2D pixel ionization chamber for implementation in clinical routine. Phys Med Biol. 2007; 52(4):1197-1208.
12. Wolfsberger LD, Wagar M, Nitsch P, Bhagwat MS, Zygmanski P. Angular dose dependence of Matrixx TM and its calibration. J Appl Clin Med Phys. 2010; 11(1):3057.
13. Krishna Murthy K, Anandagiribabu A, Prasad PBLD., Kaviarasu K. Patient specific quality assurance of RapidArc treatments: Portal prediction dosimetry compared with phantom studies. Biological Intervention and Imaging Journal 2012; 8.4:e28.
14. Nicolini G, Vanetti E, Clivio A, Fogliata A, Korreman S, et al. The GLAaS algorithm for portal dosimetry and quality assurance of RapidArc, an intensity modulated rotational therapy. Radiat Oncol. 2008; 3:24.
15. Fogliata A1, Clivio A, Fenoglietto P, Hrbacek J, Kloeck S et al. Quality assurance of RapidArc in clinical practice using portal dosimetry. Br J Radiol. 2011; 84(1002):534-545.
16. Iori M, Cagni E, Paiusco M, Munro P, Nahum AE. Dosimetric verification of IMAT delivery with a conventional EPID system and a commercial portal dose image prediction tool. Med Phys. 2010; 37(1):377-390.
17. Chandraraj V, Stathakis S, Manickam R, Esquivel C, Supe SS, et al. Comparison of four commercial devices for RapidArc and sliding window IMRT QA. J Appl Clin Med Phys. 2011; 12(2):3367.
18. Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010; 37(8):4078-4101.
19. Rowshanfarzad P, Sabet M, Barnes MP, O'Connor DJ, Greer PB. EPID-based verification of the MLC performance for dynamic IMRT and VMAT. Med Phys. 2012; 39(10):6192-6207.