Full Text
As compared with the past, the current medical practice ignores the usefulness of taking skull radiographs. Radiographs of the skull may not contribute to the diagnosis of brain injury, bleeding or other space occupying lesions in the brain. Intracranial calcifications may give a clue to brain disorders, but this paper does not include all brain lesions. Conventional radiographs of the skull play a major role in arriving at the final diagnosis of many systemic disorders. Antero posterior and lateral views are taken routinely. Advanced imaging like computed tomography (CT) and magnetic resonance imaging (MRI) may not be always necessary. However, clinical history and radiographs of the other skeletal areas are very important in arriving at a final diagnosis. The main objective of this paper is to deal with osseous portions of the calvarium and to study the abnormalities which may contribute to the final diagnosis. Systemic disorders, congenital/ developmental abnormalities are included in the Table 1 and 2.
Table 1: Systemic disorders.
- Congenital/ Developmental
- Inflammatory
- Infections/ Infestations
- Hemopoietic
- Metabolic and endocrinal
- Neoplastic – metastasis and myeloma
- Toxic
- Miscellaneous
Table 2: Congenital/ developmental abnormalities.
- Osteopetrosis
- Pycnodysostosis
- Camurati engelmann dysplasia
- Craniometaphyseal dysplasia – Pyle’s
- Craniocleidodysostosis
- Fibrous dysplasia
- Osteogensis imperfecta
- Phacomatosis
- Mucopolysaccharidosis
- Craniostenosis
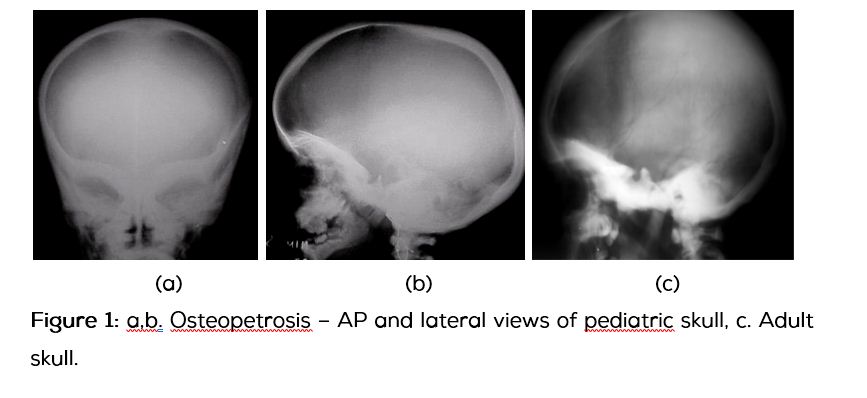
Osteopetrosis (Marble bone disease) is also called Albers-schonberg disease which results from defective osteoclasts. Radiologically, bones are sclerotic and thick, but weak and brittle. Two separate sub types exists. One, infantile autosomal recessive osteopetrosis and two, benign adult autosomal dominant osteopetrosis.
Common radiological findings
The calvarium is dense and thick (more at the base) with narrowing of neural foramina. The paranasal sinuses are under developed (Figure 1a,b,c).
Pycnodysostosis
It is a rare autosomal recessive bone dysplasia characterized by osteosclerosis and short stature and is also known as Toulouse-Lautrec syndrome. It is due to genetic deficiency in cathepsin K, which is essential for normal osteoclast function.
Common radiological findings
The features include frontal bossing, Wormian bones, mid line defects and obtuse angle of the mandible (Figure 2a,b).
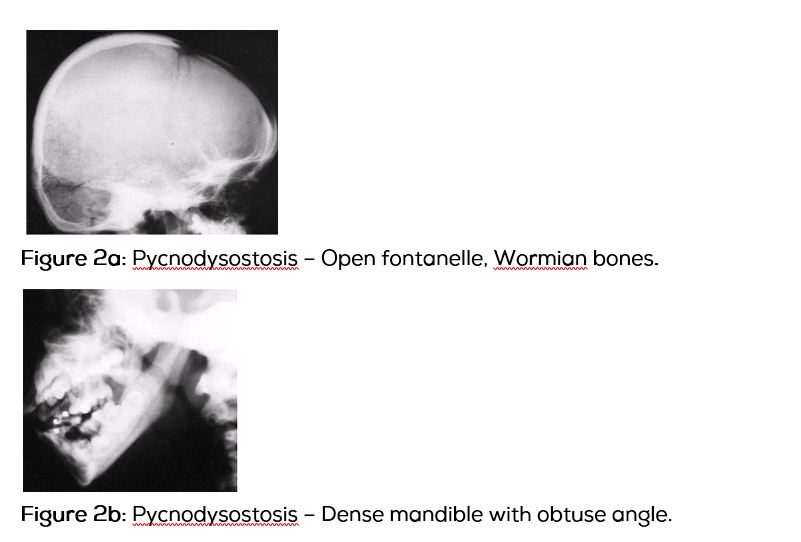
Figure 2a: Pycnodysostosis – Open fontanelle, Wormian bones.
Figure 2b: Pycnodysostosis – Dense mandible with obtuse angle.
Camurati engelmann dysplasia
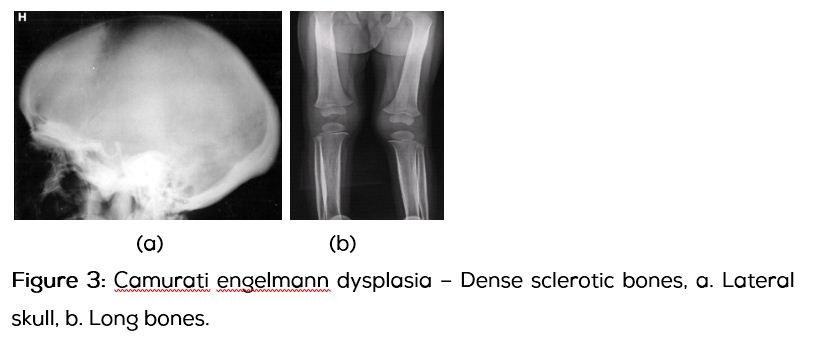
It is a progressive diaphyseal dysplasia with sclerotic dense diaphyses of long bones. The skull bones are also sclerotic (Figure 3a). However, from the radiographs of the skull one cannot diagnose this entity and radiographs of long bones are necessary (Figure 3b).
At this juncture, a differential diagnosis of diffuse sclerosis of calvarial bones (Table 3) may be of help.
Table 3: Differential diagnosis of diffuse sclerosis of calvarial bones.
Developmental
- Osteopetrosis
- Pycnodystosis
- Camurati engelmann – Progressive diaphyseal dysplasia
- Pyle’s disease - Craniometaphyseal dysplasia
- Van buchem’s disease
- Idiopathic hypercalcemia
- Fibrous dysplasia
- Hyperphosphatemia
- Cyanotic heart disease
- Hemopoietic
Other causes
- Hemolytic anaemia
- Mastocytosis
- Myelofibrosis
- Hyper/ hypoparathyroidism
- Renal osteodystrophy with secondary hyperparathyroidism
- Dilantin therapy
- Fluorosis
- Paget’s disease
Craniometaphyseal dysplasia
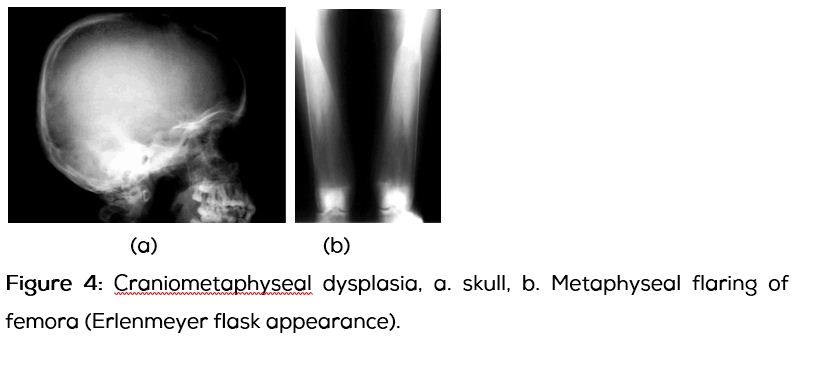
Basic cranium with flaring of metaphyseal ends of long bones (Figure 4a,b).
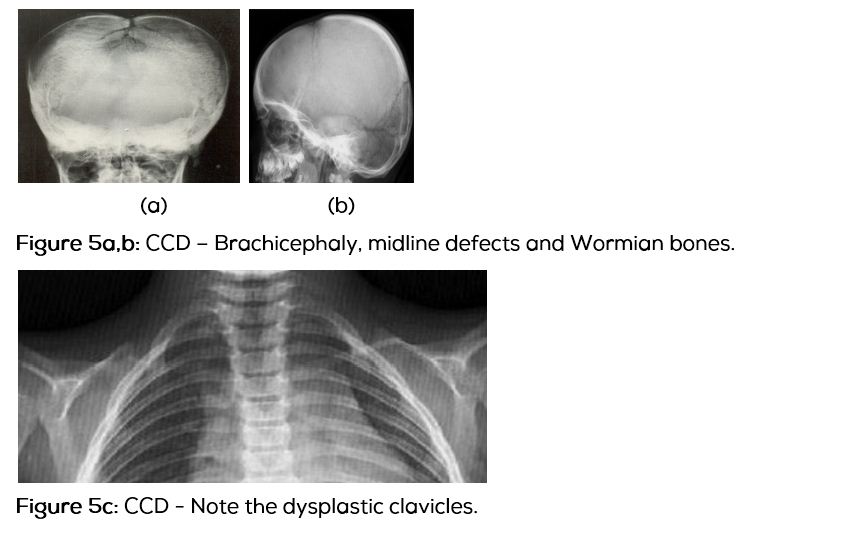
Craniocleidodysostosis (CCD)
It is a developmental dysplasia. The radiological characteristics of the skull include open fontanel, midline defects and Wormian bones. Radiological examination of the clavicles confirms the diagnosis as there is dysplasia of calvicles (Figure 5a,b,c).
Fibrous dysplasia (FD)
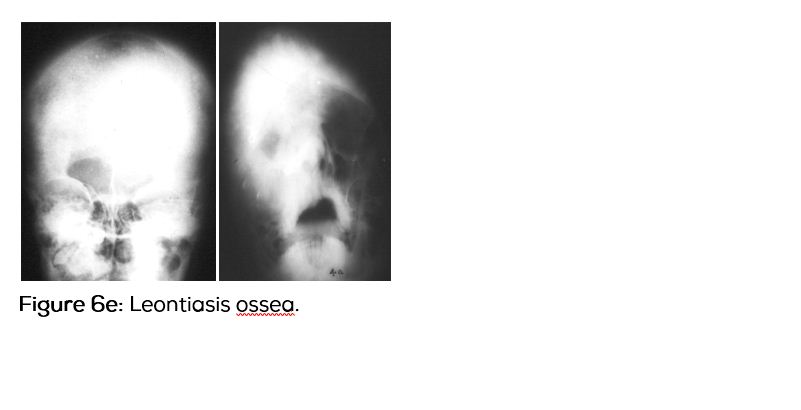
It is developmental aberration with fibrous replacement of the normal bone. It may be monostotic, polyostotic or a part of Albright syndrome. Radiological findings of craniofacial fibrous dysplasia include expanded outer table with little effect on inner table. Three types of radiological appearances have been described. One is purely lytic, the second purely sclerotic and the third is mixed sclerotic and lytic changes. Sclerotic changes are mainly in the basicranium and face. A lytic area surrounded by dense sclerosis is the skull bones, is typical of a “blister” appearance.
In the valut, the outer table is expanded with a lytic lesion in the centre. This is called a “bone blister” (Figure 6a,b,c,d). When the skull and facial bones are extensively involved with sclerosis, it is described as Leontiasis ossea (Figure 6e).
Osteogenesis imperfecta (OI) congenita & tarda (eight types of congenital forms)
There are four major types, which are I - Mild, Blue sclera; II - Perinatal, Lethal; III – Uncommon, Severe; IV – Uncommon, Resembles 1.
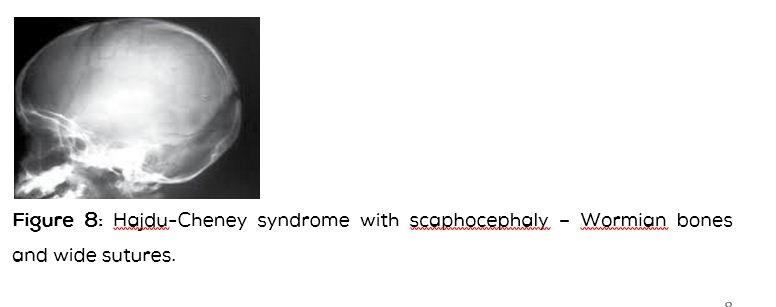
Radiological features include a variable spectrum. Intrauterine recognition by ultrasound is known. Radiological features include fractures, lucent bones, unossified skull bones with Wormian bones in Table 4 (Figure 7). Basilar impression is often noted.
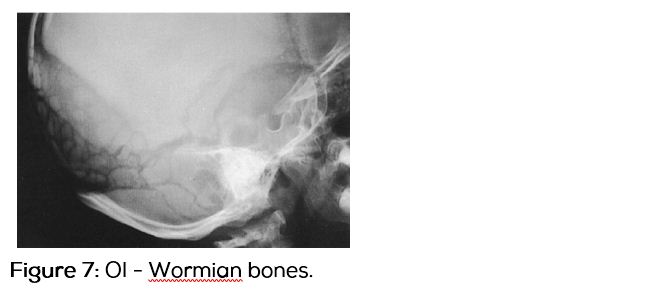
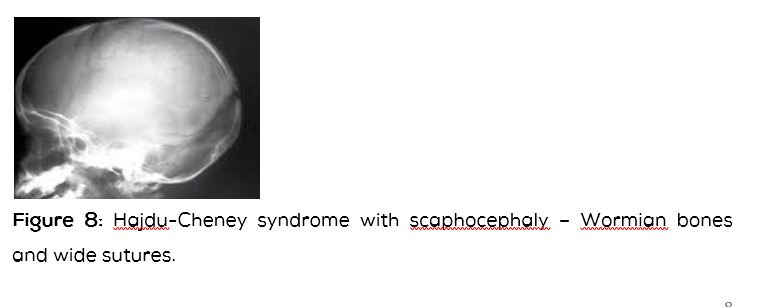
Table 4: Differential diagnosis of Wormian bones.
- Osteogenesis imperfecta
- Cleidocranial dysostosis
- Pycnodysostosis
- Cretinism
- Rickets
- Hajdu–Cheney syndrome (Figure 8)
Phacomatoses
These are neuro-oculo-cutaneous syndromes and neurocutaneous disorders. These are multisystem disorders that have characteristic central nervous system, ocular and cutaneous lesions of variable severity. The osseous system may also be involved in some of these (Table 5).
Table 5: Some of the disorders.
|
Ø Tuberous sclerosis
Ø Neurofibromatosis
Ø Cystic angiomatosis
Ø Sturgeweber syndrome
Ø Turcot syndrome
Ø Gardener syndrome
|
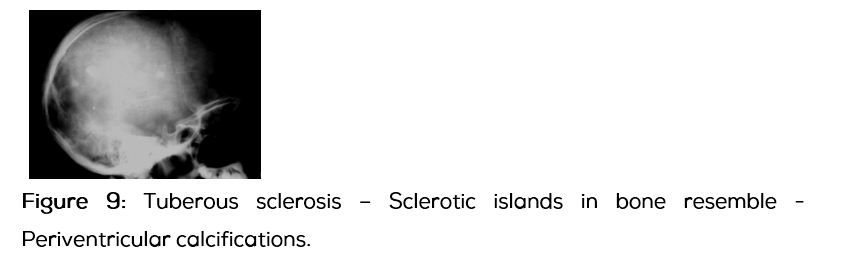
Tuberous sclerosis (Epiloia)
The clinical triad includes sebaceous cysts over the face, seizures and mental deficiency of the brain. Skull radiographs often overlap the intracranial calcifications due to gliosis (Figure 9).
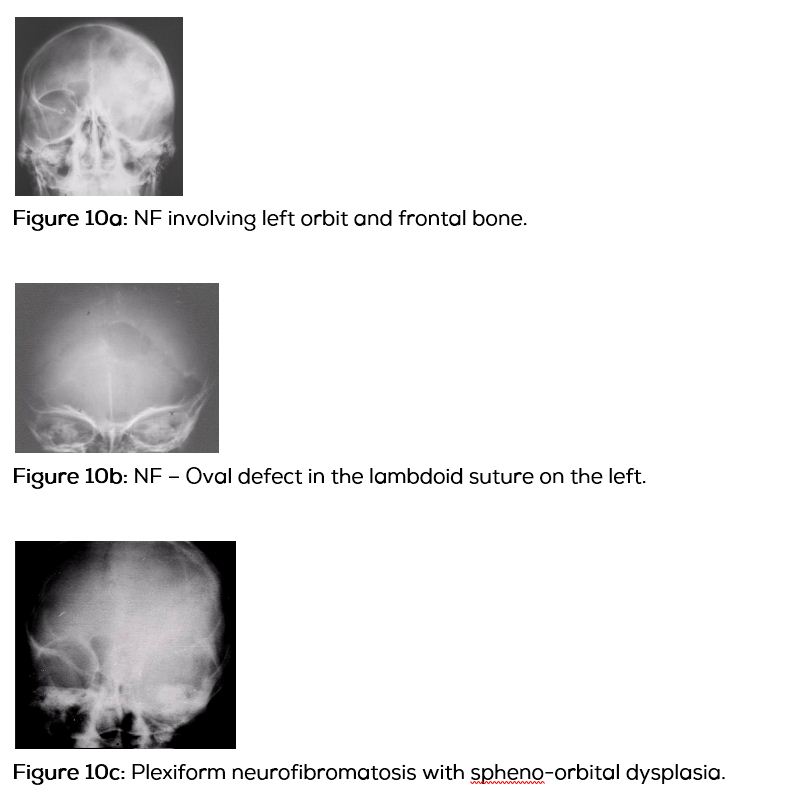
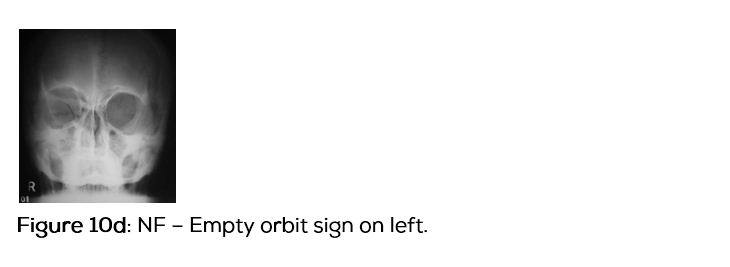
Neurofibromatosis (NF)
This is one of the neurocutaneous syndromes and eight different types have been described. Out of these, NF1 and NF2 are important.
Radiological findings of the skull in NF1 include macrocranium, asymmetrical skull, empty orbit and lambdoidal sutural defect etc. The findings are mainly due to mesenchymal dysplasia rather than neurofibromata (Figure 10a,b,c,d).
Neurofibromatosis: Comparison between NF-1 and NF-2 (Table 6).
Table 6: Comparison between NF-1 and NF-2.
|
NF - 1
|
NF – 2
|
|
1. Von Recklinghausen’s disease
|
1. Bilateral acoustic schwannomas
|
|
2. 1/4000 (represents 90% of NF cases)
|
2. 1/150,000 (<10% of NF cases)
|
|
3. Chromosome 17
|
3. Chromosome 22
|
|
4. Prominent skin manifestations
|
4. Minimal skin changes
|
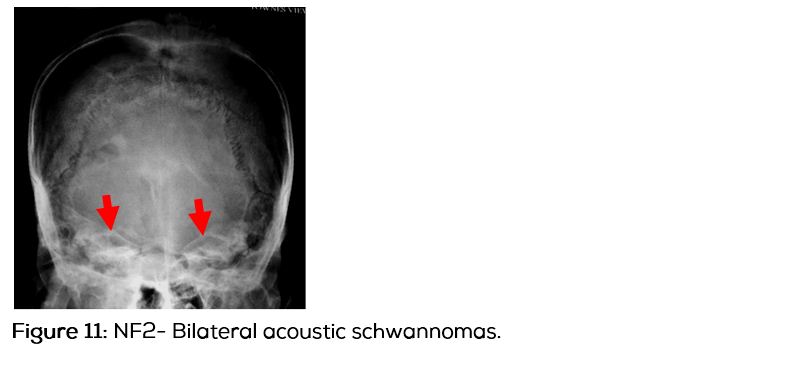
In NF2, bilateral acoustic schwannomas are common (Figure 11).
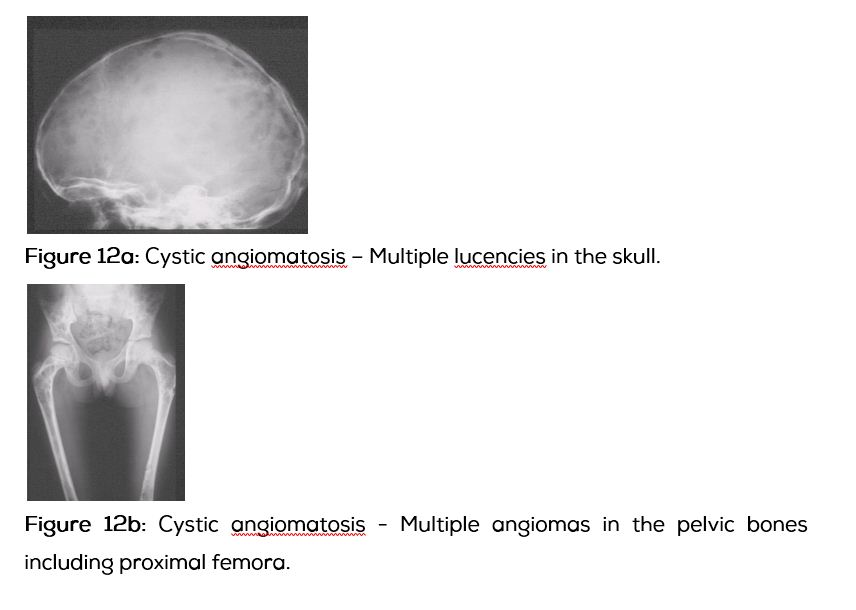
Cystic angiomatosis
In this entity, endothelial lined spaces representing lytic areas are seen throughout the skeleton. These may be vascular, lymphatic or both. Multilocular cystic lesions are noted predominantly in the axial skeleton. In the skull, multiple lucent areas are seen. With the suspicion radiographs of other bones are taken to confirm the diagnosis (Figure 12a,b).
Other entities of Phacomatosis do not have significant changes in the skull.
Mucopolysaccharidosis (MPS)
This is a group of lysosomal disorders with absence of specific enzymes in each entity. A specific diagnosis based on the skull findings may be difficult. However, in Hurler syndrome a “J” shaped sella is a prominent feature along with frontal bossing scaphocephaly and calvarial thickening (Figure 13a,b). Hand and spine radiographs confirm the diagnosis.
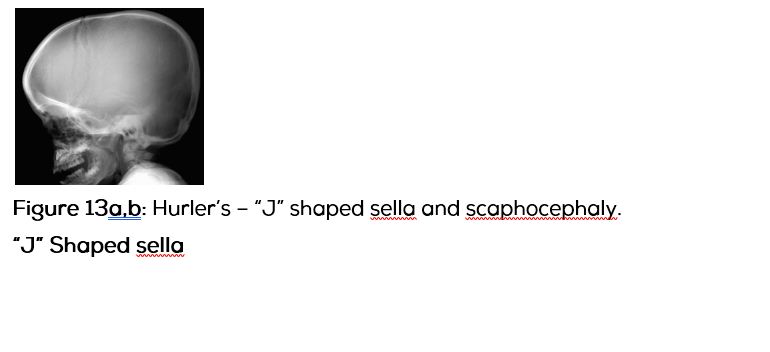
J shaped sella-flattened tuberculum sellae with a prominent sulcus chiasmaticus.
Causes of J-shaped sella: Normal variant in 5% of normal children; Optic chiasm glioma-if chiasmatic sulcus is markedly depressed (w or omega shaped sella), tumour may be bilateral; Chronic hydrocephalus-due to downward pressure of an enlarged third ventricle; Mucopolysaccharidosis-Hurler syndrome; Achondroplasia-Neurofibromatosis-sphenoid dysplasia.
Craniostenosis are primary (Due to premature closure of the sutures) and secondary (causes), secondary craniostenosis are listed i. Metabolic-Rickets, hyperthyroidism, hypophosphatasia; ii. Inborn errors of metabolism-MPS syndromes; iii. Hematalogical-sickle cell anaemia,thalassemia, spherocytosis; iv. Malformations of brain-microcephaly, holoprosencephaly; v. Iatrogenic-shunted hydrocephalus.
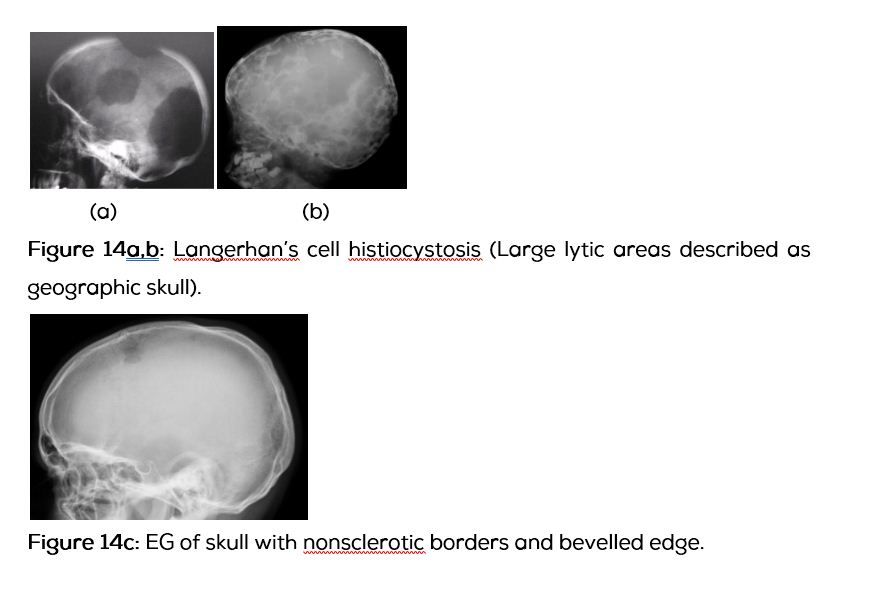
Inflammatory lesions
Inflammatory lesions involving the skull include Langerhan’s cell Histiocystosis and sarcoidosis. Langerhan’s cell histiocytosis consist of three groups, which are 1. Letterer Siwe’s disease seen in infants; 2. Hand-Schuller-Christian (HSC) disease seen in children and young adults; 3. Eosinophilic granuloma encountered at any age. Radiographic findings in the skull include large lytic areas described as geographical skull are noted in HSC disease (Figure 14a,b). In eosinophilic granuloma which can be encountered at any age solitary or multiple lytic areas are noted. Often it shows a bevelled edge due to unequal involvement of the outer and inner cortices of the skull (Figure 14c).
Sarcoidosis
Involvement of the skull bones is rare in sarcoidosis. However, multiple non-specific lytic lesions are noted.
Infections
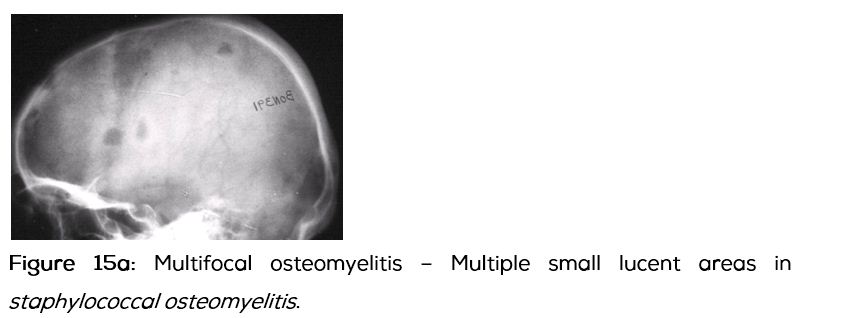
Systemic infections involving the skull are quite rare. Pyogenic bacterial osteomyelitis, unifocal or multifocal may manifest as lytic lesions. Clinical findings clinch the diagnosis. The common organism is staphylococcus (Figure 15a).
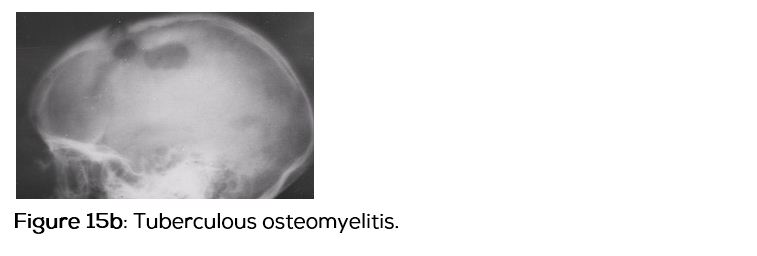
Tuberculous osteomyelitis of the skull is also rare. It generally involves frontal and parietal bones. A draining sinus may often be noted. Radiologically, there are no specific characteristics (Figure 15b).
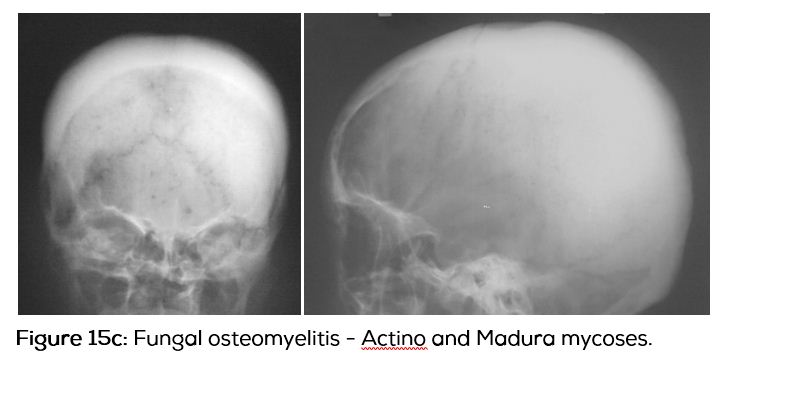
Fungal infections of the skull generally produce diffuse osteosclerosis with very little lytic changes (Figure 15c).
Parasitic infestations
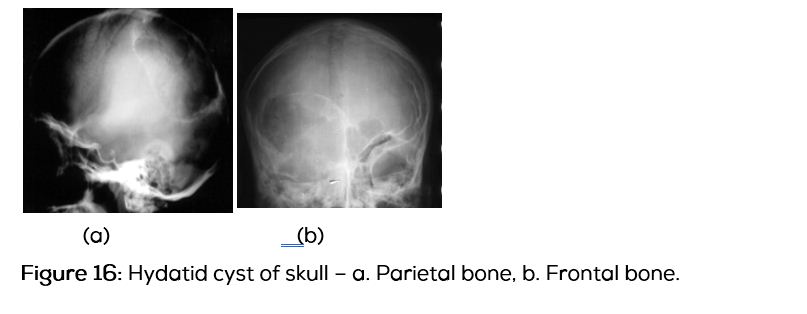
Echinococcus (hydatid) infestations involving the skull are quite rare. However, if correlated with the findings noted in the liver, lung and kidneys, the diagnosis is possible. Radiologically, a sharply defined, expanding and lytic area is often a common finding (Figure 16a,b).
Metabolic disorders
Common metabolic disorders that may involve the skull include nutritional rickets, hypophosphatasia and hyperphosphatasia.
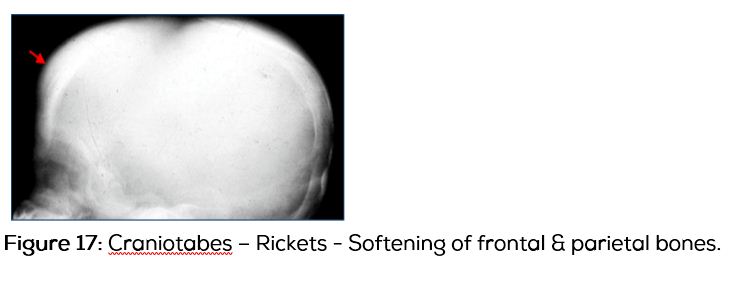
Rickets due to vitamin “D” deficiency is still encountered in certain areas. Although, growing ends of bones are affected, skull also may show features of rickets, mainly in the frontal bone (Figure 17).
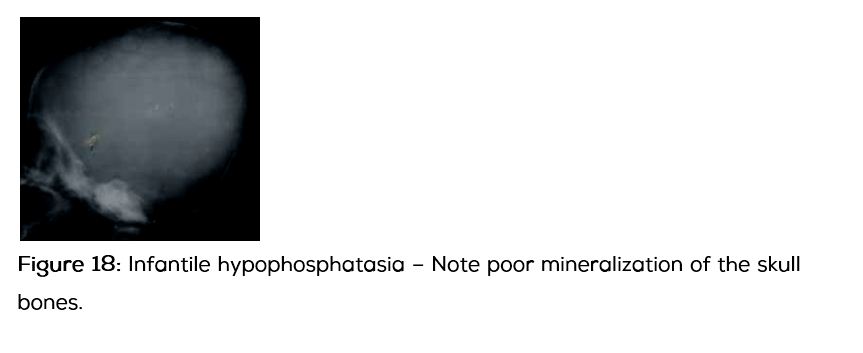
Hypophosphatasia
It is a heritable autosomal recessive disorders of bone metabolism. In the infantile form, radiograph of the skull shows deficient mineralization (Figure 18). Later in childhood, craniostenosis may be noted.
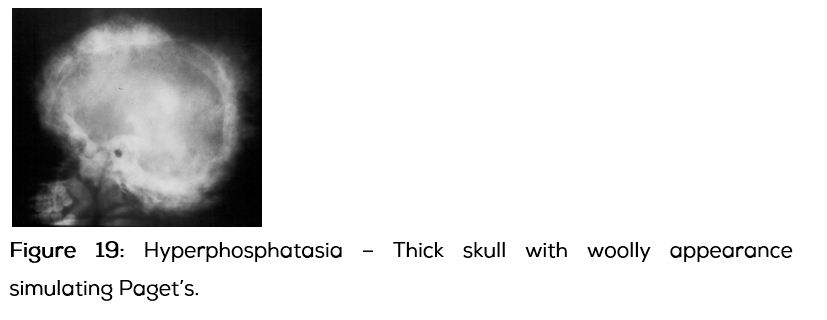
Hereditary hyperphosphatasia - autosomal recessive
This is due to failure to replace immature woven bone with mature lamellar bone. Mabry syndrome - Mental retardation with hyperphosphatasia. Although the entire skeleton may be involved the skull radiographs are characteristic with thickening and spherecial areas of bone sclerosis resembling Paget disease (Figure 19).
Endocrinal influences on skull radiographs
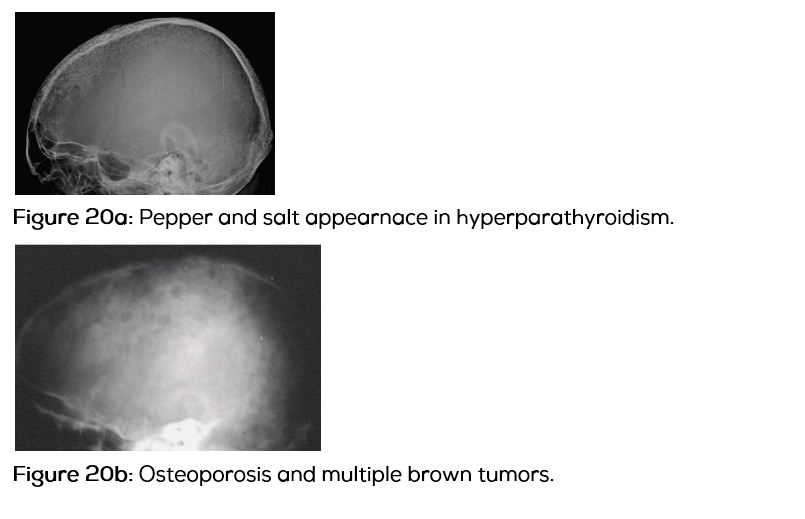
Hyperparathyroidism: This may be benign adenoma or carcinoma of the parathyroids resulting in hyperparathyroidism. Clinically and radiologically characteristic features are noted. In the skull, osteoporosis with pepper and salt appearance is a common feature (Figure 20a). Occasionally, lytic areas of varying size may be noted (Figure 20b).
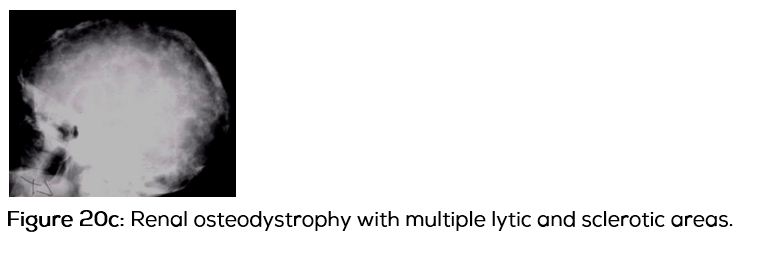
Renal osteodystrophy as the name denotes is due to chronic renal insufficiency resulting in the radiological changes, which are osteoporosis, osteomalacia, osteosclerosis, soft tissue calcifications, and secondary hyperparathyroidism.
Radiologically, the skull may show areas of osteosclerosis with brown tumors (Figure 20c).
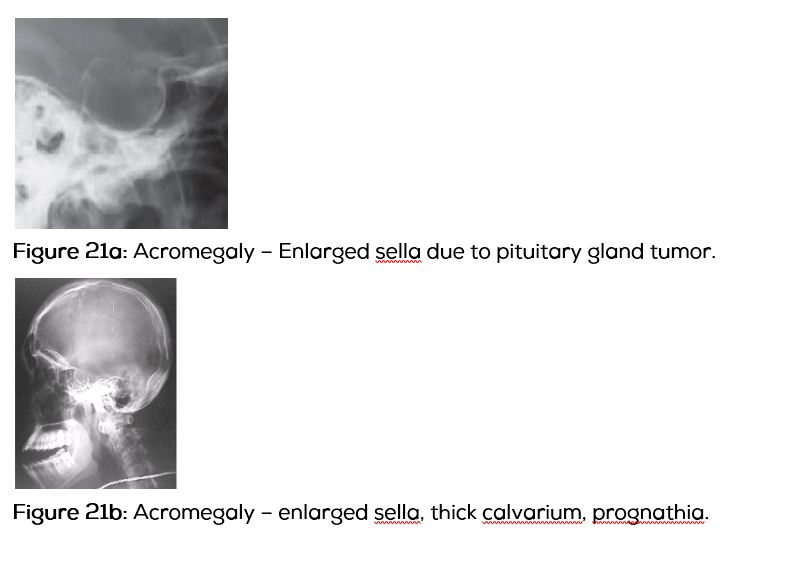
Next Endocrinal disorder that commonly affects the skull is hyperpituitarism, resulting in features of acromegaly. Radiologically, the sella is often enlarged. The calvarium bones are thick with prognathism (Figure 21a,b).
Enlarged sella – differential diagnosis: Empty sella syndrome; Intracranial hypertension; Pituitary tumours; Craniopharyngioma.
Small sella may be normal but below mentioned disorders may shows small sella: Normal variant; Hypopituitarism; Microcephaly; Myotonic dystrophy; Prader-willi-lambert syndrome; Cockayne syndrome; Dystrophia myotonica.
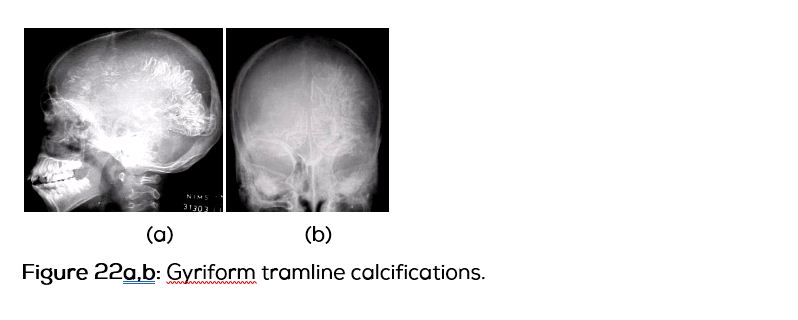
Sturge-Webber syndrome
This is due to leptomeningeal venous malformations with gyriform subpial tramline calcifications. It may be ipsilateral to facial nevus or bilateral. The hemi cranium on the affected side may be a little small in size. However, the intracranial calcifications are classical of this entity (Figure 22a,b).
Hemolytic anaemias
These are majorly of two types. One is thalassemia (Table 7) and the second sickle cell anemia.
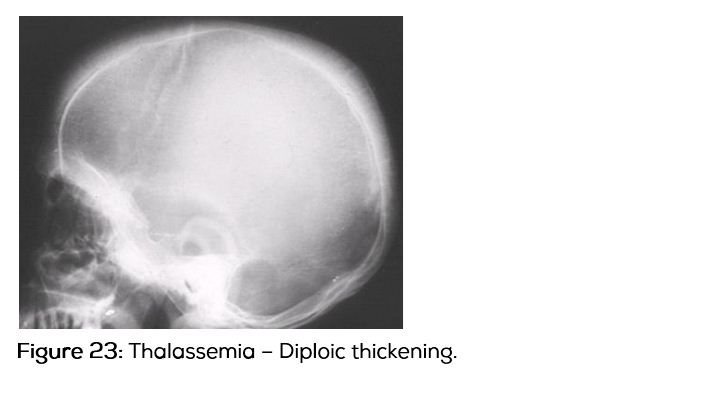
Table 7: Thalassemia skull – Radiological findings are mentioned.
|
Ø Widening of dipole (Figure 23)
Ø Thinning of outer table
Ø Obliteration of outer table
Ø Hypermedullosis
Ø “Hair on end” or “brush border”
Ø Obliteration of air sinuses
|
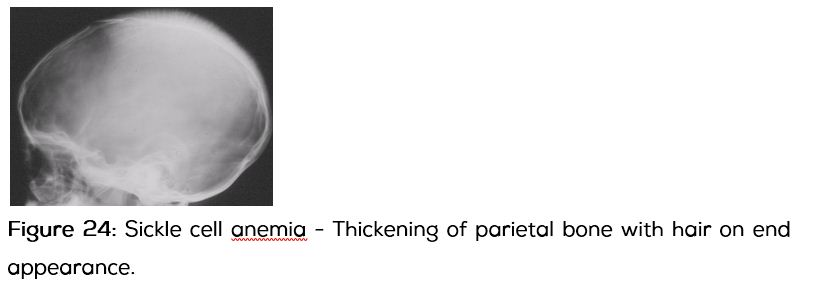
Sickle cell disease
Thickening of the diploe of skull bones is noted. But, the paranasal sinuses are not affected (Figure 24).
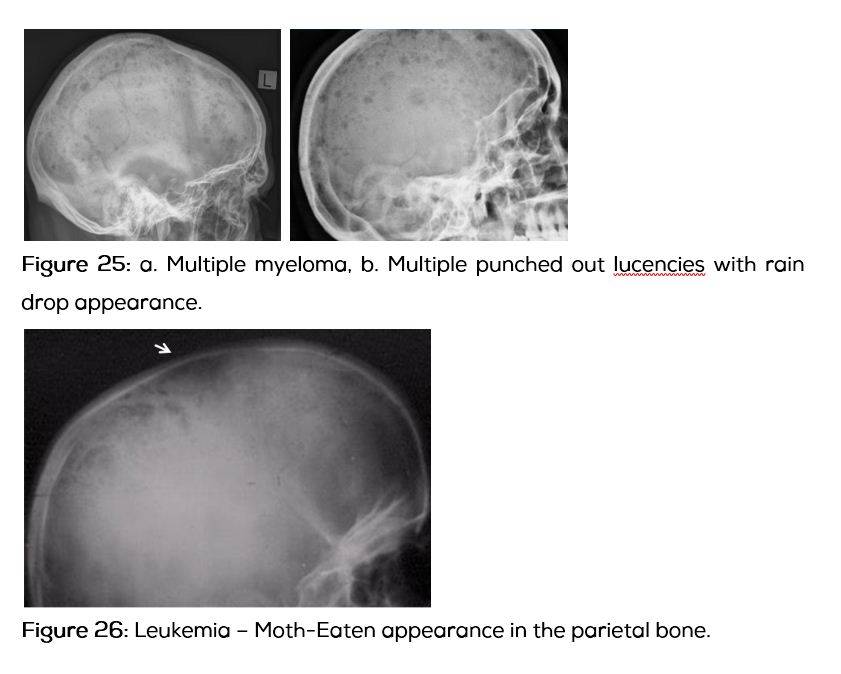
Calvarial lesions – Neoplastic malignant
Multiple myeloma (Figure 25a,b). Variable pattern of osteolysis including punched out areas are noted.
Leukaemia (Figure 26) – Osteoporosis with Moth-Eaten appearance is noted.
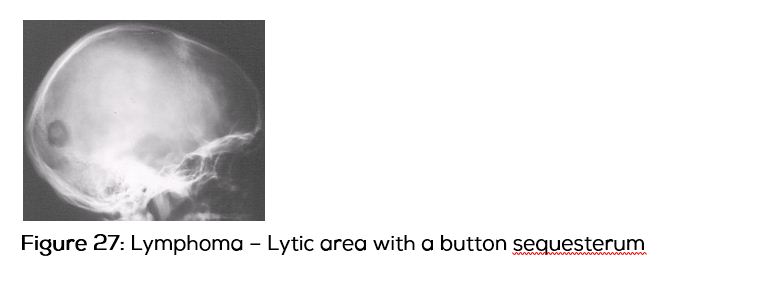
Lymphoma (Figure 27) – Rare mixed osteolytic and sclerotic lesions are noted.
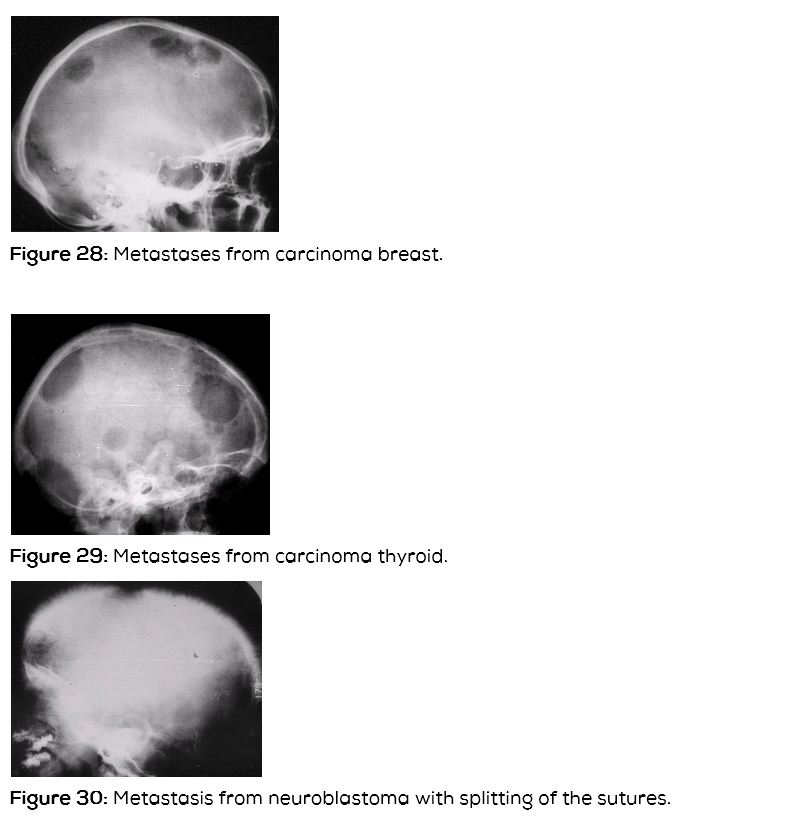
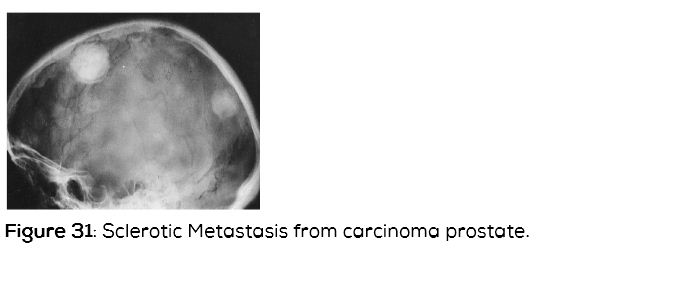
Metastases
Ø 10% of all metastatic lesions affect the calvaria
Ø 90% -- lytic lesions (Figure 28)
Ø Blastic lesions < 10%
Ø Lytic- Tyroid and breast (Figure 29)
Ø Mixed – breast and GI malignancies
Ø Neuroblastoma - Mixed lesions (Figure 30)
Ø Blastic- Prostate and carcinoid (Figure 31)
Toxic
Ø Fluorosis
Ø Lead poisoning
Ø Hypervitaminosis D
Fluorosis – 1932 caused by the following factors. The most common cause is endemic water intake which contains exceeding amounts of fluorine.
Ingestion
Ø Water
Ø Food
Ø Tonic
Ø Wine
Ø Therapy
Inhalation
Ø Industrial - Cryolite, Al, Glass, Enamel
Ø Fertilizer - Superphosphate
Ø Addiction - Methoxyfluorane
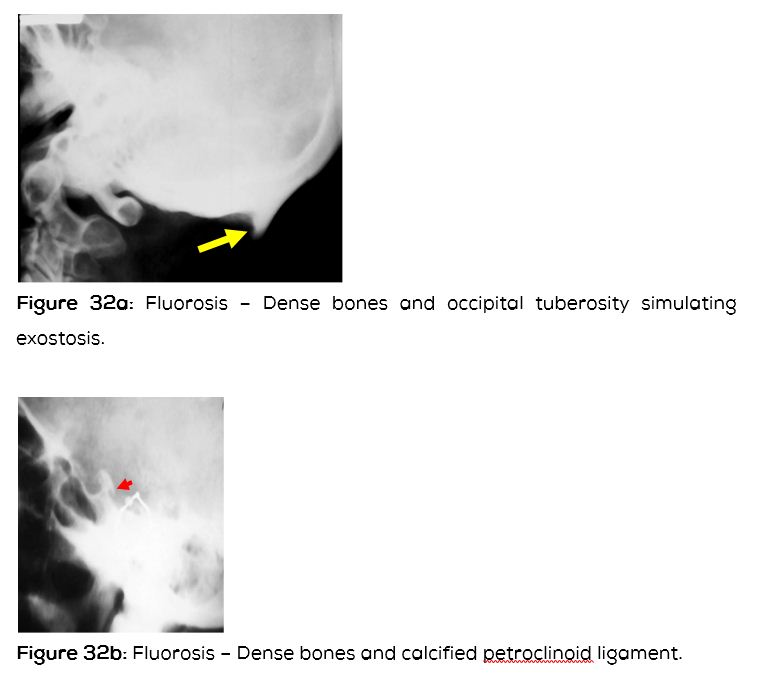
Radiological findings include dense bones with calcification of ligaments and muscular attachments (Figure 32a,b).
Miscellaneous – Paget’s
Ø Osteitis deformans
Ø Chronic bone disorder with excessive abnormal bone remodelling
Ø Pelvis (often asymmetric)
Ø Skull
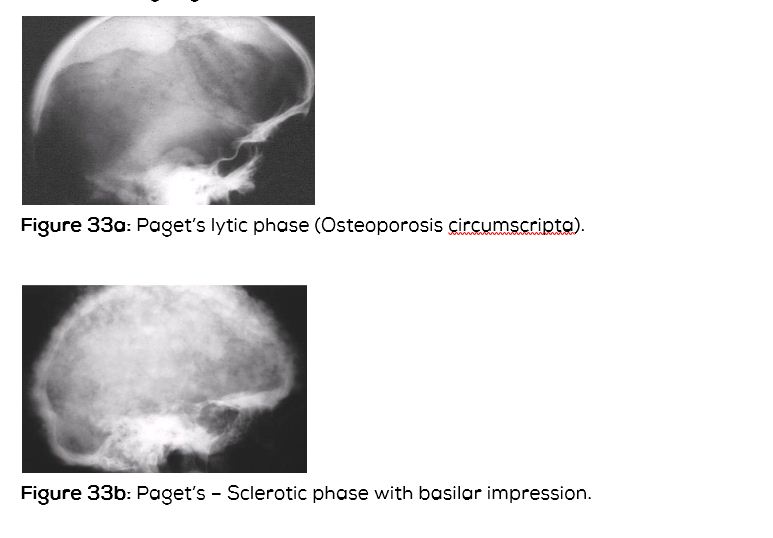
Radiological findings – Lytic, sclerotic and mixed
Ø Active (osteolytic) osteoporosis circumscripta in skull (large well defined lytic lesion) (Figure 33a).
Ø Osteolytic and sclerotic phase.
Osteosclerotic phase with cotton wool appearance of skull and diploic widening (Figure 33b).
Conclusion
Conventional radiographs of the skull are rarely taken at the present time, since CT and MRI play a major role in neuroradiology. However, several systemic disorders and traumatic situations demand skull radiographs. The container is also important in studying the contents. A variety of disorders reflecting on the skull radiographs are described with various radiological features.
Acknowledgements
Departments of radiology, NIMS & KREST Museum, Hyderabad.
Conflicts of interest
Author declares no conflicts of interest.