Case Report
2013
March
Volume : 1
Issue : 1
Suprasellar colloid cyst: An unusual location
Paniraj GL, Panigrahi M, Reddy AK, Satish Rao
Pdf Page Numbers :- 5-8
Paniraj GL1,*, Panigrahi M1, Reddy AK1 and Satish Rao2
1Department of Neurosurgery, Krishna Institute of Medical sciences, Minister Road, Secunderabad - 500003, AP, India
2Department of Neuropathology, Krishna Institute of Medical sciences, Minister Road, Secunderabad - 500003, AP, India
*Corresponding author: Dr. Gurram Lokamanya Paniraj, MCh (Neurosurgery), Junior Consultant, Krishna Institute of Medical Sciences, Minister Road, Secunderabad - 500003, AP, India, Mobile: +91 8008404160; Email: glphaniraj@yahoo.com
Received 18 December 2012; Revised 20 January 2013; Accepted 2 February 2013
Citation: Paniraj GL, Panigrahi M, Reddy AK and Satish. Suprasellar Colloid Cyst: An Unusual Location. J Med Sci Res 2013; 1(1): 5-8. http://dx.doi.org/10.17727/JMSR.2013/1-001
Copyright: © 2013 Paniraj GL et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Colloid cysts are rare intracerebral lesions that are preferentially encountered within the third ventricle. There are only a few reports in which colloid cysts are described in other locations such as the fourth ventricle, brainstem, cerebellum and suprasellar region.
Clinical description: Young female had presented with headache since one year and on episode of generalized tonic, clonic seizures one week ago. She had bitemporal visual field cuts on examination. Imaging showed a hyperdense suprasellar lesion which was isointense on T1 weighted MR images, profoundly hypointense on T2 weighted images, and did not show any enhancement on post contrast MR study. It showed no restriction on DWI. A pteronal craniotomy and total excision of the lesion was done and the patient recovered well with no further neurological deficits. Pathology was consistant with a colloid cyst.
Conclusion: Colloid cyst is rarely found in suprasellar location. Such a rare diagnosis has to be considered in the differential diagnosis in patients who present with a suprasellar cystic lesion.
Keywords: Colloid cyst; Enterogenous cyst; Rathkes' cleft cyst
Full Text
Background
Colloid cysts are rare intracerebral lesions that are preferentially encountered within the third ventricle. There are only a few reports in which colloid cysts are described in other locations such as the fourth ventricle, brainstem, cerebellum and suprasellar region. Colloid cysts are rare lesions, accounting for 0.2 to 2% of all intracranial neoplasms. They are slow-growing benign tumors, the majority of which are located in the third ventricle [4, 5, 9, 10]. Other locations include the leptomeninges,the posterior fossa,and the fourth ventricle [1, 3, 6-8]. In the present report we describe the clinicopathological features of a case of suprasellar colloid cyst.
Case report
A 27 year old female presented to us in December 2011, with history of headache since one year and decreased vision since one month. One week prior she came to us with an episode of generalized tonic clonic seizures. On examination, she had a normal vision on the left side and 6/24 visual acuity on the right side. She had minimal bitemporal field cuts on visual field charting. She had no other deficits. Her hormonal status was normal.
Imaging
Axial CT study of the brain revealed a well-defined hyperdense mass lesion located within the suprasellar cistern, with the contents showing attenuation values of 103 Hounsfield units. There were no fluid levels or foci of wall calcification. CT Angiogram performed to exclude vascular origin of the lesion revealed posterior displacement and normal caliber of the basilar artery [Figure 1]. The lesion was uniformly isointense on T1 weighted MR images, profoundly hypointense on T2 weighted images, and did not show any enhancement on post contrast MR study [Figure 2]. It was limited superiorly by the floor of the third ventricle, anteriorly by the infundibulum of pituitary gland and posteriorly by the basilar artery. Focal inferior extension into the sella with invagination between the anterior and posterior lobes of the pituitary gland was appreciable. No restriction was noted on diffusion weighted scan [Figure 3].
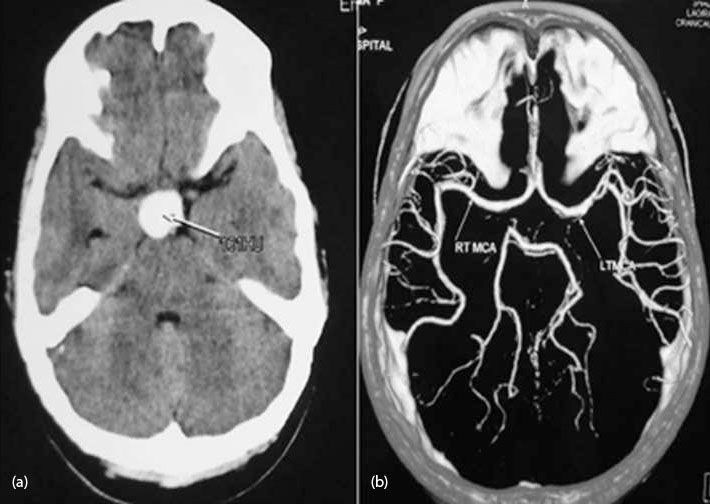
Figure 1: (a) CT - brain showing a well-defined hyperdense mass lesion located within the suprasellar cistern, with the contents showing attenuation values of 103 Hounsfield units. There are no fluid levels or foci of wall calcification. (b) No aneurysm is seen onCT Angiogram.
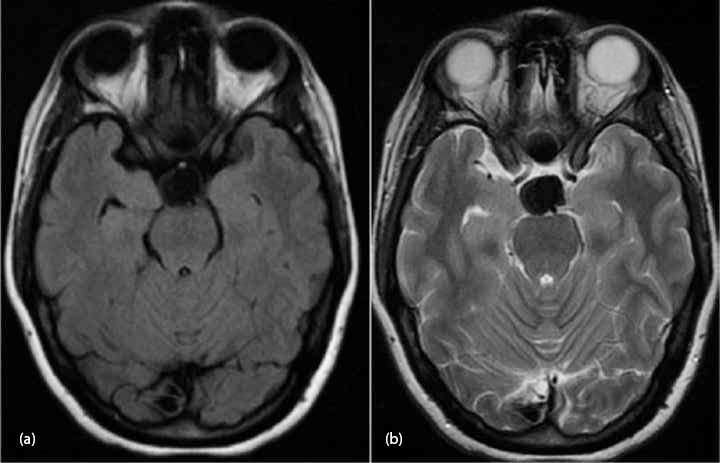
Figure 2: (a) The lesion is uniformly isointense on T1 and hypointense image. (b) The lesion is uniformly isointense on T2 weighted image.
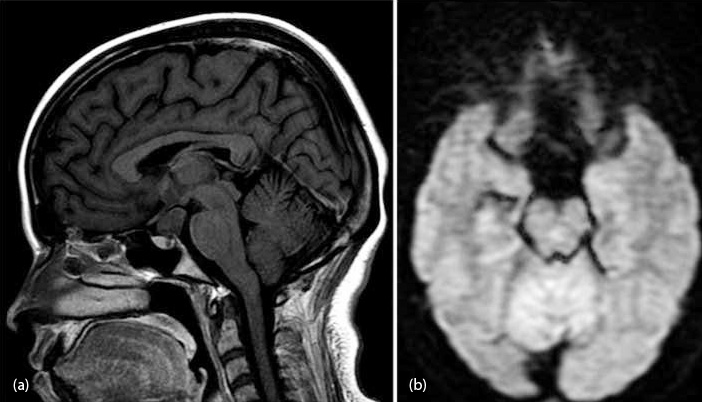
Figure 3: (a) It was limited superiorly by the floor of the third ventricle, anteriorly by the infundibulum of pituitary gland and posteriorly by the basilar artery. Focal inferior extension into the sella with invagination between the anterior and posterior lobes of the pituitary gland was appreciable. (b) No restriction was noted on diffusion weighted scan.
Operation
The patient underwent a right Pteronal craniotomy and total excision of the lesion via the opticocarotid and interoptic corridors. Greenish cyst filled with mucinous material was noted intraoperatively [Figure 4].
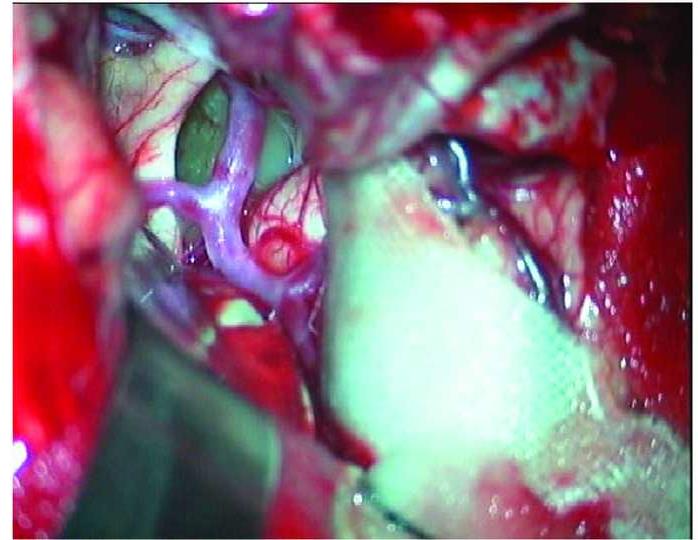
Figure 4: Intraoperative picture showing the greyish cyst in suprasellar location.
Histopathology
Microscopic examination revealed a cyst containing eosinophilic material lined by a single layer of out cuboidal cells and ciliated coloumnar cells [Figure 5]. They have stained positive for EMA and cytokeratin [Figure 6a, b, c].
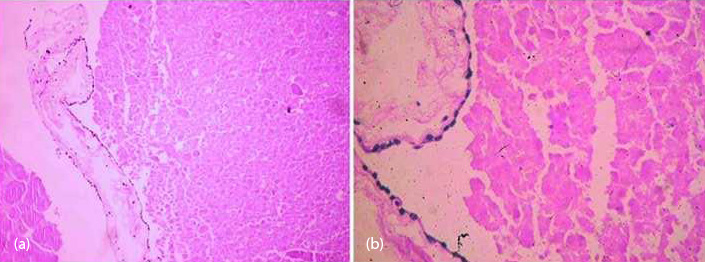
Figure 5: H & E staining showing the cyst containing eosinophilic material lined by a single layer of out cuboidal cells and ciliated colomnar cells.
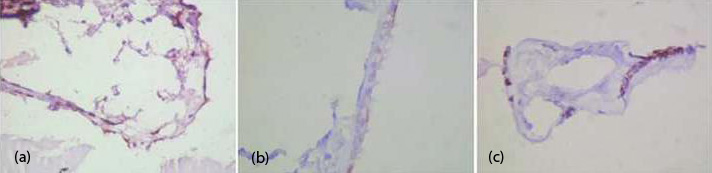
Figure 6: The lesion showing positive staining for EMA (6a) and cytokeratin(6b,c).
Postoperative course
The patient improved symptomatically. At one month of follow up, the Vision remained unchanged.
Discussion
In the differential diagnosis of suprasellar lesions, the following had been considered in our case: Rathekes cleft cyst, craniopharyngioma, aneurysm, enterogenous cyst and colloid cyst. Colloid cysts are commonly found in the third ventricular region and are rarely found in suprasellar location. Nomikos et al, had reported 11 colloids cysts in their series of 69 sellar and suprasellar cystic Lesions [7]. Colloid cyst wall is built of a collagenous connective tissue stroma, lined with a single layer of pseudostratified epithelium. The cells may be columnar, ciliated and nonciliated, cuboidal or squamous. The cyst consists of gelatinous material. [5, 8, 11] They can be found anywhere throughout the neuroaxis, but commonly appear within the third ventricle [6, 7]. Neuroepithelial and endodermal origin have been considered for the pathogenesis. Ciric et al, emphasized invagination or evagination of neuroepithelium from the diencephalic roof into the space between the two fornices and eventually resulting cyst formation as the mechanism attributed to explain lesions within the third ventricle or upward in the septum pellucidum [1]. The theory for extraventriculer or cortical location consists of neuro-epithelial cysts originating from primitive ectopic glial tissue in the subarachnoid space. Shuangshoti et al, reported that these so called neuroepithelial cyst have a common origin from the seessel pouch (endodermal diverticulum located behind the oropharyngeal membrane) and they show histological features similar to Rathke’ cleft cysts and enterogenous cyst [7]. Grazizani et al, proposed that all these cysts arise from Seessel pouch and should be named according to their localization. Nevertheless, despite the controversy, histopathological investigation remains the standard diagnostic method for discriminating between these lesions [2].
The cyst consists of gelatinous material that reacts positively to periodic acid–Schiff staining. They stain positively for cytokeratin and EMA. They are negative for GFAP and Prealbumin stains. Expression of CEA,Viamentin and S-100 varies. In contrast, endodermal cysts are lined by a two- layered, mucin-secreting ciliated, cuboidal-to-columnar epithelium that resembles that of respiratory and intestinal tracts, which exhibit immunopositivity for carcinoembryonic antigen and cytokeratin [5]. However, differentiating between these two entities in such rare locations is difficult. Clinical findings indicate that these cysts progressively expand in response to many mechanisms, such as active fluid secretion by the epithelial lining cells, or fluid entry into the isolated cyst due to the osmotic effect of the high intracystic protein level, which permits water diffusion from surrounding tissue into the cyst. The best management of colloid cyst in this location is total excision and the same was done in our patient.
Conclusion
We report a case of a suprasellar colloid cyst that was successfully removed via Pterional approach. Although rarely found in this location, such a rare diagnosis has to be considered in the differential diagnosis in patients who present with a suprasellar cystic lesion.
Conflicts of interest
Authors declare no conflicts of interest.
Abbreviations
CT: Computed Tomography; CEA: Carcino Embryonoc antigen; DWI: Diffussion Weighted Imaging; EMA: Epithelial Membrane Antigen; GFAP: Glial Fibrillary Acidic Protein; MR: Magnetic Resonance; Suprasellar colloid cyst: an unusual location.
References
1. Ciric I, Zivin I. Neuroepithelial (colloid) cysts of the septum pellucidum. J Neurosurg 1975, 43: 69-73.
2. Graziani N, Dufour H, Figarella-Branger D, Donnet A, Bouillot P, Grisoli F. Do the suprasellar neurenteric cyst, the Rathke cleft cyst and the colloid cyst constitute a same entity? Acta Neurochir (Wien) 1995, 133:174–180.
3. Jan M, Ba Zeze V, Velut S. Colloid cyst of the fourth ventricle: diagnostic problems and pathogenic considerations. Neurosurgery 1989, 24:939–942.
4. Hernesniemi J, Leivo S. Management outcome in third ventricular colloid cysts in a defined population: a series of 40 patients treated mainly by transcallosal microsurgery. Surg Neurol 1996, 45:2–14.
5. Mackenzie IRA, Gilbert JJ. Cysts of the neuraxis of endodermal origin. Journal of Neurology, Neurosurgery, and Psychiatry 1991, 54:572-575.
6. Müller A, Büttner A, Weis S. Rare occurrence of intracerebellar colloid cyst- Case report. J Neurosurg 1999, 91:128–131.
7. Nomikos et al. Intra- and suprasellar colloid cysts. Pituitary 1999, 2: 123-6.
8. Parkinson D, Childe AE. Colloid cyst of the fourth ventricle. Report of a case of two colloid cysts of the fourth ventricle. J Neurosurg 1952, 9:404–409.
9. Shuangshoti S, Netsky MG. Neuroepithelial (colloid) cysts of the nervous system. Further observations on pathogenesis, location,incidence, and histochemistry. Neurology 1966, 16:887–903.
10. Shuangshoti A, Roberts MP, Netsky MG. Neuroepithelial (colloid) cysts. Arch Path 1965, 80:214-24.
11. Shuangshoti S, Pitakdamrongwong N, Ponepraset B, et al. Symptomatic neuroepithelial cysts in the posterior cranial fossa. Immunohistochemical and electron-microscopic studies. Surg Neurol 1988, 30:298–304.