Case Report
2014
March
Volume : 2
Issue : 1
Waist line skin cancer: A case report
Jagadishwar Goud G, Kaveri Shaw, Vikas Kumar MB, Arun Katari, Kiranmai Gottapu V
Pdf Page Numbers :- 21-23
Jagadishwar Goud G1,*, Kaveri Shaw1,*, Vikas Kumar MB1, Arun Katari1 and Kiranmai Gottapu V1
1Department of Surgical Oncology, Minimal Inavasive and Robotic assisted Laparoscopy, Krishna Institute of Medical sciences, Minister Road, Secunderabad - 500003, AP, India.
*Corresponding authors: Dr. Jagadishwar Goud Gajagowni, MS, M.Ch, Consultant Surgical Oncologist, Department of Surgical Oncology, Minimal Inavasive and Robotic assisted Laparoscopy, Krishna Institute of Medical Sciences, Minister Road, Secunderabad - 500003, AP, India, Email: jagadishgdr@yahoo.com and Kaveri Shaw, Department of Surgical Oncology, Minimal Inavasive and Robotic assisted Laparoscopy, Krishna Institute of Medical Sciences, Minister Road, Secunderabad - 500003, AP, India. Tel.: +91-8801805202; Email: kaverishaw@gmail.com
Received 23 October 2013; Revised 21 December 2013; Accepted 28 December 2013
Citation: Kaveri Shaw, Jagadishwar Goud G, Vikas Kumar MB, Arun Katari, Kiranmai Gottapu V. Waist line skin cancer: A case report. J Med Sci Res 2014; 2(1):21-23. DOI: http://dx.doi.org/10.17727/JMSR.2014/2-004
Copyright: © 2014 Kaveri Shaw et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Squamous cell carcinoma of skin is second most common non melanoma malignancy next to Basal cell carcinoma. The occurrence of diseases is noticed in various part of the body but waist line skin is not a common site for it. The present case report is that of elderly male from south India wearing typical south Indian ethnic wear Lungi and developed the disease in waist line with primary metastasis. Surgery stays the main treatment of choice after topical chemotherapeutic agents and radiation. The case needs its reporting due its rarity and association with hypertension and diabetes which are said to be at lower risk for this malignancy.
Keywords: Lungi cancer; Squamous cell carcinoma; Waist line cancer
Full Text
Introduction
Clothing performs a range of social and cultural functions, such as individual, occupational and sexual differentiation, and social status. In many societies, norms about clothing reflect standards of modesty, religion, gender, and social status. The dhoti and saree are the traditional ethnic wear in most part of India. Unfortunately it has been found to be associated with a specific type of skin cancer [1]. The dhoti is a piece of large cloth (mostly cotton fabric) wrapped around waist by south Indian men as a cultural dress. There is no tie in lungi/dhoti. The upper end is rolled over waist and tied together. The traditional wear gets moist with sweat and dust due to sunny and humid environment in southern India. Long time usage is a source of infection and irritiation over skin. The constant friction by tight garments causes keratosis and dermatitisis of skin and may progress to carcinoma [2]. The squamous cell carcinoma the second most common skin cancer is found to be present due to chronic irritation following keratosis and dermatitis [3]. This cancer was named as Dhoti cancer or saree cancer in 1945 by khanolkar and Suryabai [2].
Case report
An eighty year old male presented to outpatient department with complaint of ulcero-proliferative growth in left side of waist line since 4 months. The subject used to wear tight lungi (traditional ethnic wear of South India, a sheet of cloth wrapped around waist) since his young age (approximately 60 yr) and noticed some irritation since one year. Initially there was dry skin with occasional pruritis. Recently he noticed a thickened growth along the same site which gradually started growing with on and off bleeding. Home remedies and topical application of different ointments were tried .This non healing ulcer with growth brought him to physician. The biopsy of growth was diagnosed as squamous cell carcinoma.
On examination an ulcero-proliferative growth in left waist line measuring 17x11x4 cm with ulcer of 7x4x1 cm was noticed. Blood oozing from growth noticed. Surrounding skin was thick, atrophied and hypopigmented (Figure 1).

Figure 1: The ulcero-proliferiative growth on the left waist line skin with surrounding hypopigmented skin in Eighty year old diabetic and hypertensive male of south India.
The bilateral groin palpated. Lymph node enlargement not found. The subject is a known hypertensive since 15 yr and is regularly on Angiotensin Receptor blockers (ARB’s). Recently he developed complete heart block with coronary artery disease for which permanent pacemaker implantation with revascularization was done 2 month back. He is also a known Diabetic since 5 years and is on oral hypoglycemic drugs. After primary work up case planned for wide excision with left inguinal block dissection.
A 2 cm margin from visible lesion was taken and the tumor was excised (Figure 2).
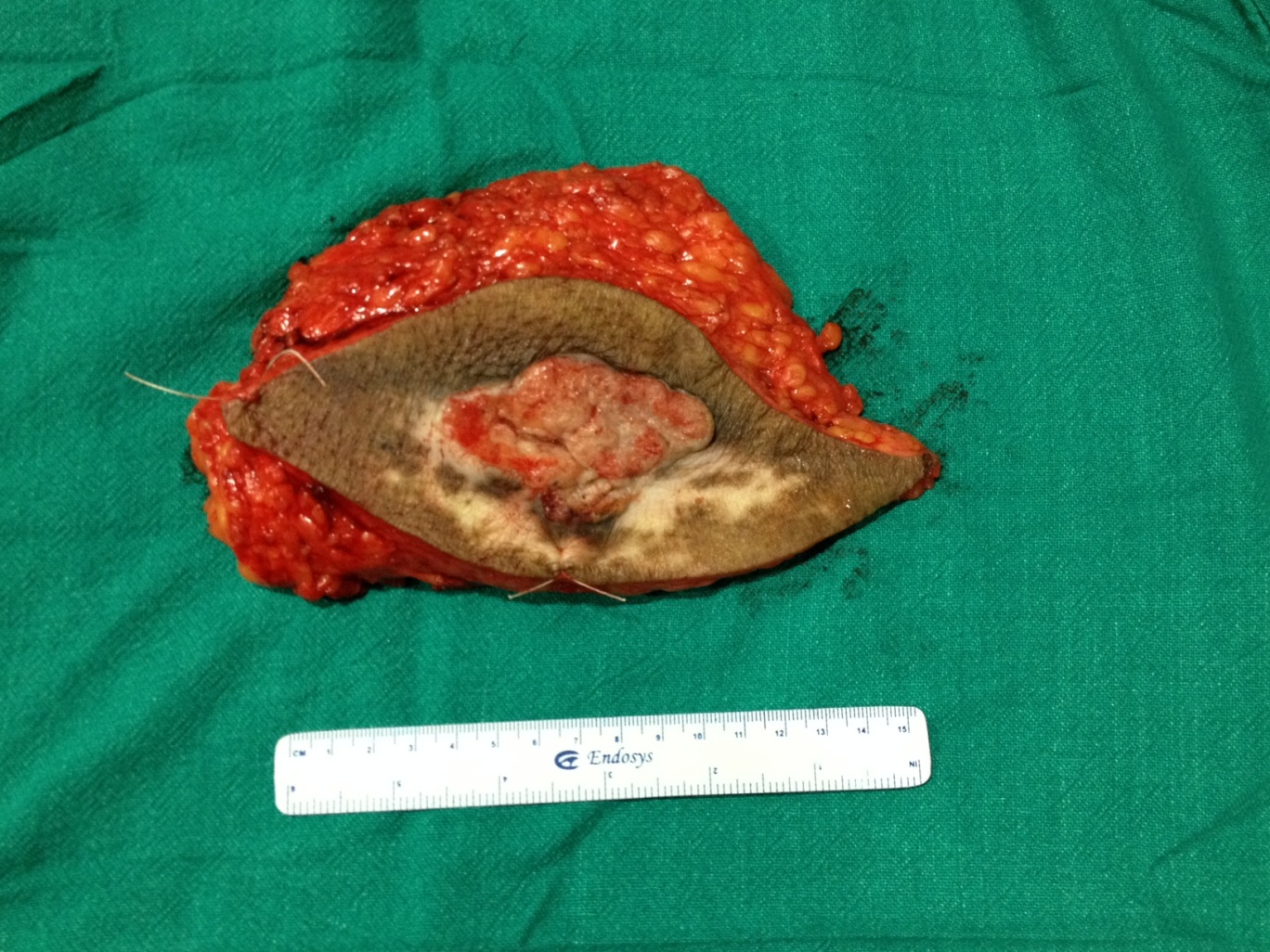
Figure 2: The specimen of the mass from waist line skin with adequate margins.
The tension free skin approximation was done. A subcutaneous drain was kept. The inguinal lymph nodes were enlarged and en-block dissection was done (Figure 3).

Figure 3: The post closure wound of waist after wide excision and groin after lymph node dissection.
Post operative course was uneventful.The patient was discharged on post operative day three.
The final histopathology report is suggestive of a well defined squamous cell carcinoma with tumor free margins. One of the three dissected inguinal lymph node is showing metastatic deposit. Radiation treatment is planned.
Discussion
Squamous cell carcinoma (SCC) of skin is the second most common cancer of skin [4]. The risk factors earlier described by various authors include the age more than 50 yr, male sex, sun exposure, constant irritation, chronic scarring, chemical irritation, immunecompromised status and HPV infection [3, 5].
One interesting fact came out from a case control study that use of anti hypertensive drugs like angiotensin receptor blockers and ACE inhibitors reduces the 33% relative risk of developing squamous cell carcinoma [6]. But only 33 % does not mean 100 % secure. Therefore though there may be protective factors in any cancer but close watch on disease can give better results.
The lesion usually starts as hypo-pigmented chronically irritated area of skin as dermatoses. Later the atrophic skin becomes thick and appears as raised firm, flesh colored papule or plaque and progresses to everted growth and ulcer. Atrophic dermatitis has been found to be more prone for developing carcinoma [7]. Most of the time the patient seeks treatment once the lesion becomes chronic non healing ulcer.
The best part of the SCC is early diagnosis due to non healing ulcer which brings the patient to health care professional before it gets metastasized. The diagnosis of lesion is done by full thickness biopsy without missing the extent of lesion till dermis. The radiologic investigation like, CT SCAN, PET-SCAN has limited role only to evaluate metastasis.
This cancer is locally infiltrating and extensive metastasis at the time of diagnosis is uncommon. The thickness of tumor is one of the factor for determination of metastasis. A Tumor thickness of 2 mm or less does not metastasis, 6 mm or more presents with 16% metastasis and 2.1-6 mm only 4% with metastasis at the time of diagnosis [8]. In the present patient, the lesion has infiltrated more than 6 mm depth from skin and presenting with local metastasis. The recurrence rate also postulated in similar manner from multivariate analysis of SCC.
The widely accepted treatment plan for this kind of tumor is surgery. The wide excision of tumor with resection of margins more than 1 cm with inguinal block dissection [9]. The National Comprehensive Cancer Network 2013, Multi professional guidelines from British association of dermatologists and all various dermatologist groups suggest that the principle of treatment of SCC should be to resect the tumor with preservation of function and cosmesis according to age and risk factor for the patient. The other non surgical options include topical application of 5 fluorouracil and imatinib in low risk group. The third option is local radiotherapy but acceptable for early lesions only. The radiation may be the option in high risk group when surgery causes compromised cosmesis [10].
Conclusion
Squamous cell carcinoma of skin is not a rare disease but along the waist line is not common. The tight garments are now proved to be associated in developing the typical waist line cancer. The studies also suggest that the relative low risk of developing such a cancer in hypertensive individuals with ARBs and ACE inhibitor as well as in diabetics on oral hypoglycemic drugs. The present case is complete exception for such. Other than this Squamous cell carcinoma has precursor as keratosis. It should be taken care where ever possible. Wide excision is the treatment of choice with adjuvant radiation.
Conflicts of interest
Authors declare no conflicts of interest.
References
1. Eapen BR, Shabana S, Anandan S. Waist dermatoses in Indian women wearing saree. Indian J Dermatol Venereol Leprol. 2003; 69(2):88-89.
2. Khanolkar VR, Suryabai B. Cancer in relation to usages; three new types in India. Arch Pathol (Chic). 1945; 40:351-361.
3. Motley RJ, Preston PW, Lawrence CM. Multi-professional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma; 2009.
4. Johnson TM, Rowe DE, Nelson BR, Swanson NA. Squamous cell carcinoma of the skin (excluding lip and oral mucosa). J Am Acad Dermatol. 1992; 26(3 Pt 2):467-484.
5. Vagholkar KR. Cutaneous Squamous Cell Carcinoma At An Unusual Site. The Internet Journal of Dermatology. 2010; 8(1).
6. Groch J. Blood Pressure Drugs Linked to Protection Against Non-Melanoma Skin Cancer. Dermatology. 2008.
7. Darjani A, Mohtasham-Amiri Z, Mohammad Amini K, Golchai J, Sadre-Eshkevari S, et al. Skin Disorders among Elder Patients in a Referral Center in Northern Iran (2011). Dermatol Res Pract. 2013.
8. Brantsch KD, Meisner C, Schönfisch B, Trilling B, Wehner-Caroli J, et al. Analysis of risk factors determining prognosis of cutaneous squamous-cell carcinoma: a prospective study. Lancet Oncol. 2008; 9(8):713-720.
9. Robins P, Dzubow LM, Rigel DS. Squamous-cell carcinoma treated by Mohs' surgery: an experience with 414 cases in a period of 15 years. J Dermatol Surg Oncol. 1981; 7(10):800-801.
10. National Comprehensive Cancer Network, Basal cell and Squamous cell skin cancer 2013.
http://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf.