Case Report
2016
March
Volume : 4
Issue : 1
Primary Sjogren syndrome with diffuse alveolar hemorrhage, cryoglobulinaemia and thrombotic microangiopathy
Vijaya Prasanna Parimi, Liza Rajasekhar
Pdf Page Numbers :- 26-27
Vijaya Prasanna Parimi1,* and Liza Rajasekhar2
1Department of Rheumatology, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India
2Department of Rheumatology, Nizam’s Institute of Medical Sciences, Punjagutta, Hyderabad, Telangana 500082
*Corresponding author: Dr. P. Vijaya Prasanna, Consultant Rheumatologist, Department of Rheumatology, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India. Mobile: +91 9849145372; Email: prasanna.parimi.vijaya@gmail.com
Received 15 October 2015; Revised 3 December 2015; Accepted 16 December 2015; Published 25 December 2015
Citation: Parimi VP, Rajasekhar L. Primary Sjogren syndrome with diffuse alveolar hemorrhage, cryoglobulinaemia and thrombotic microangiopathy. J Med Sci Res. 2016; 4(1):26-27. DOI: http://dx.doi.org/10.17727/JMSR.2016/4-008
Copyright: © 2016 Parimi VP, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Sjogren syndrome is an autoimmune exocrinopathy with various extra glandular manifestations. Cryoglobulinemia, small vessel vasculitis has been reported in 5-10% of patients with primary Sjogren syndrome. It may be associated with a higher prevalence of extra glandular disease in Sjogren patients. Thrombotic microangiopathy (TMA), a potentially lethal condition characterized by microvascular thrombosis due to endothelial injury, is rare in SS. Its most characteristic histological finding is intravascular and intraglomerular fibrin thrombi. The association of Sjogren syndrome, cryoglobulinemia and thrombotic microangiopathy has not been previously reported. We report the first case of Sjogren syndrome with these three manifestations, occurring in combination.
Keywords: Sjogren syndrome; alveolar hemorrhage; cryoglobulinemia; thrombotic microangiopathy; pulmonary-renal syndrome
Full Text
Sjogren syndrome (SS) is an autoimmune disease primarily affecting the exocrine glands. Its spectrum extends from an autoimmune organ specific disease to a systemic process. Cryoglobulins are cold precipitable proteins - usually immunoglobulins. Cryoglobulinemia is a small vessel vasculitis caused by deposition of immune complexes. Thrombotic microangiopathy (TMA), a potentially lethal condition characterized by microvascular thrombosis due to endothelial injury, is rare in SS. Its most characteristic histological finding is intravascular and intraglomerular fibrin thrombi. SS associated with cryoglobulinemia, presenting with alveolar hemorrhage & TMA in combination is rare. Pulmonary-renal syndrome with alveolar hemorrhage and rapidly progressive glomerulonephritis occurring due to cryoglobulinemia in patients with SS with associated TMA has not been reported previously.
Case report
A 37-year old lady admitted in Nizams Institute of Medical Sciences, Hyderabad, was diagnosed as primary SS, based on the presence of oral mucosal and ocular dryness, polyarthritis, positive anti-Ro and anti-La antibodies, and a minor salivary gland biopsy showing lymphomononuclear infiltration.
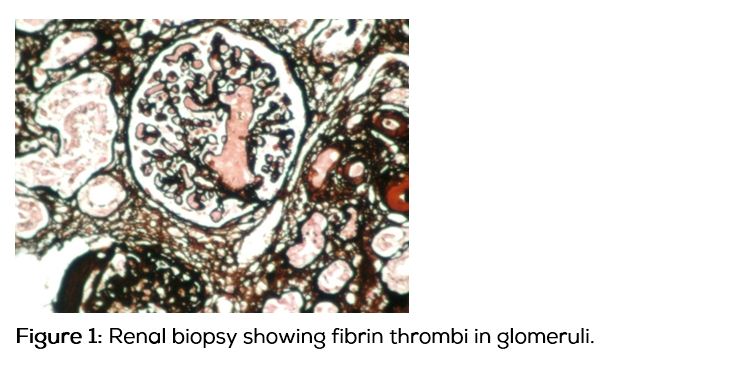
During the course of her illness, she developed superficial punctate keratitis and mononeuritis multiplex and pulmonary arterial hypertension. She was admitted with cough and hemoptysis of 2 days duration. On examination she was pale with tachycardia. Investigations revealed anemia with normal leucocyte and platelet counts. Serum biochemistry was unremarkable. Arterial blood gas (ABG) analysis showed hypoxemia. Radiographs of chest revealed bilateral homogenous opacities in both the lower zones. A high resolution computed tomography of chest showed ground glass opacities predominantly in the basal segments of both lungs, findings of which was compatible with diffuse alveolar hemorrhage. Bronchial wash cytology showed evidence of hemosiderin laden macrophages. A diagnosis of diffuse alveolar hemorrhage was thus made and was initiated on pulse corticosteroids and subsequently oral prednisolone, along with pulse cyclophosphamide therapy. Her hemoptysis initially subsided with therapy and recurred on attempting to taper prednisolone. She subsequently developed severe hemoptysis two days after discharge and was readmitted. Clinical examination revealed pallor, tachycardia, and tachypnea. Investigations showed evidence of anemia, normal platelet count. ABG revealed hypoxemia. During hospital stay, she developed renal dysfunction with severe thrombocytopenia. Anti dsDNA, ANCA, anticardiolipin antibodies and lupus anticoagulant were negative. Complements were low. Cryoglobulins were positive. Peripheral smear, serum electrophoresis was normal. Despite therapy with pulse corticosteroids, her alveolar hemorrhage and renal dysfunction worsened. Plasmapheresis was thus initiated. However she developed severe refractory hypoxemia and died. Post mortem renal biopsy revealed fibrin thrombi in the glomeruli and arterioles, with the absence of immune deposits, which was characteristic of a TMA [Figure 1].
Discussion
Pulmonary renal syndrome in patients with SS is rare. Cryoglobulinemia, although rare, has been described in SS with prevalence ranging from 5%-10% [1-2]. It may be associated with a higher prevalence of extra glandular disease in these patients [3]. Although diffuse alveolar haemorrhage as a manifestation of pulmonary-renal syndrome has been described in patients with cryoglobulinemia, it is again extremely rare.
TMA is rarely associated with SS. Pulmonary haemorrhage secondary to TMA has been reported in paediatric patients with HUS associated diarrhoea, but rarely reported in adults [4]. Renal involvement in TMA occurs due to occlusion of glomerular capillaries by platelet fibrin thrombi. Cryoglobulins can precipitate in the glomerular vessels, appearing as hyaline thrombi [5].
Conclusion
Ours is the first case report of a patient with SS presenting with extremely unusual manifestations including cryoglobulinemia, pulmonary-renal syndrome and TMA, all occurring in combination.
Conflicts of interest
Authors declare no conflicts of interest.
References
1. Aizawa Y, Zawadzki ZA, Micolonghi TS, McDowell JW, Neiman RS. Vasculitis and Sjögren's syndrome with IgA-IgG cryoglobulinemia terminating in immunoblasticsarcoma. Am J Med. 1979; 67(1):160–166.
2. Font J, Cervera R, Lopez-Soto A, Darnell A, Ingelmo M. Mixed membranous and proliferative glomerulonephritis in primary Sjögren's syndrome. Br J Rheumatol. 1989; 28(6):548–50.
3. Tzioufas AG, Manoussakis MN, Costello R, Silis M, Papadopoulos NM, et al. Cryoglobulinemia in autoimmune rheumatic diseases. Evidence of circulating monoclonal cryoglobulins in patients with primary Sjögren's syndrome. Arthritis Rheum. 1986; 29(9):1098–1104.
4. Derebail VK, Parikh P, Jennette JC, Kshirsagar AV. A rare cause of the pulmonary-renal syndrome: a case of atypical haemolytic-uraemic syndrome complicated by pulmonary haemorrhage. NDT Plus. 2008; 1(6):417–419.
5. Ramos-Casals M, Stone JH, Cid MC, Bosch X. The cryoglobulinaemias. Lancet. 2012; 379(9813):348–60.