Short Communications
2019
December
Volume : 7
Issue : 4
A rare variant in Pipkin classification- A technical note
Vishal Kumar, Rohit Kansal, Himanshu Bhayana, Sameer Aggarwal
Pdf Page Numbers :- 123-127
Vishal Kumar1,*, Rohit Kansal1, Himanshu Bhayana1 and Sameer Aggarwal1
1Department of Orthopedics, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh, India
*Corresponding author: Dr. Himanshu Bhayana, Department of Orthopaedics, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh-160012, India. Email: Himanshu.bhayana.mamc@gmail.com
Received 20 June 2019; Revised 20 August 2019; Accepted 2 September 2019; Published 13 September 2019
Citation: Kumar V, Kansal R, Bhayana H, Aggarwal S. A rare variant in Pipkin classification- A technical note. J Med Sci Res. 2019; 7(4):123-127. DOI: http://dx.doi.org/10.17727/JMSR.2019/7-22
Copyright: © 2019 Kumar V et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Femoral head fracture is a relatively uncommon entity. Pipkins provided classification of femoral head fractures into four types; as per the classification, type 1 includes infrafoveal fragment and type 2 includes supra foveal fragment. There is no mention of transfoveal variety in the literature. We present a case of 22-year-old male who sustained posterior hip dislocation with femoral head fracture, which appeared to be type 2 on radiological investigations. Per operatively the fracture extended both proximal and distal to fovea, which we termed it as “transfoveal” variety. The patient was managed surgically by Ganz surgical dislocation of hip, and internal fixation using 2 HCS. Trans-foveal variety of femoral head fracture is hitherto unknown variety which has not been published in the literature so far as per the authors.
Keywords: Femoral head fracture; Pipkin classification; transfoveal variety
Full Text
Introduction
Femoral head fracture is a relatively uncommon entity. 6-16% of femoral head fractures occur in conjunction with posterior hip dislocation [1-3]. It usually results from high velocity trauma and may also be associated with femoral neck or femoral shaft fracture or acetabulum fracture. The surgeon needs to have high index of suspicion for these associated injuries in such cases. Garrett Pipkin in 1957 had sub classified the Stewart and Milford grade IV fracture dislocation classification of hip and classified a new Pipkins classification that is still valid today [4, 5]. Pipkins classification not only divided the femur head fracture in to 4 groups but also dictated the further dictum of management. The management of Pipkins type 2 fracture is mostly operative and open reduction and internal fixation of fracture with headless compression screw (HCS) is recommended. Initially proposed approach for type 2 Pipkins fracture was anterior Smith Peterson approach; however, Ganz safe surgical dislocation is also getting popular in last few decades [5]. As per the classification, type 2 entails supra foveal zone, however there in no mention of transfoveal variety. Likewise, Yonk et al. in 2001, has described a new classification system based on Pipkins [6]. In this technical note we describe a hitherto unknown “trans-foveal” fracture pattern which, to the best of our knowledge, has not been published so far, and how he we tackled it.
Case summary
A 22-year-old male patient sustained road traffic accident and referred to our advance trauma center for head injury and posterior fracture dislocation of left hip with right volar Barton fracture. The close reduction of hip was already done outside in a peripheral center. Further radiograph and CT scan showed concentric reduction of left hip joint but with a large displaced intra articular fragment (Figure 1). It was classified as Pipkins type 2/Yonk type 3 (Supra-foveal) fracture. Patient also sustained subdural hematoma for which he was managed conservatively and operative plan was made for Pipkins fracture and right volar Barton injury.
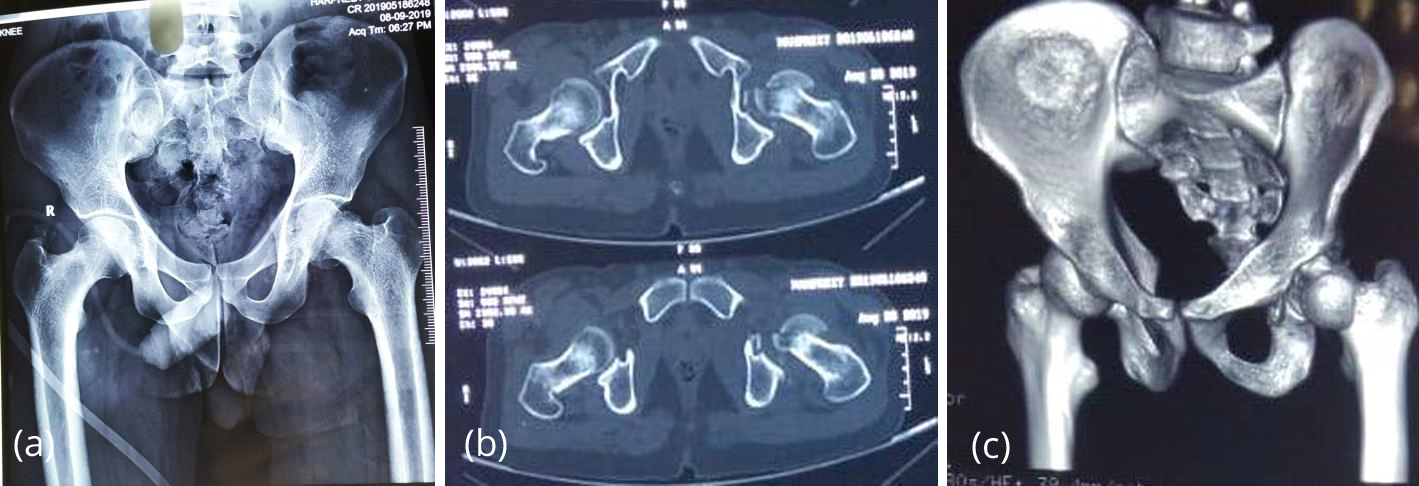
Figure 1: (a) Preoperative X ray; (b) Axial CT scan; (c) 3D recon film showing concentric reduction of hip with displaced intra-articular fragment.
After obtaining preoperative clearance from neurosurgery department, patient was taken for orthopaedic intervention after 18 days. Patient was given general anesthesia and was placed in lateral decubitus position with left side up. Ganz safe surgical approach was planned following which trochanteric flip osteotomy done and hip was dislocated anteriorly after Z shaped anterior capsulotomy. On thorough examination of head and hip joint, the fragment was retrieved. After preparing the fracture bed, it was realized that the fracture line has extended both inferior and superior to fovea centralis. We termed it as “trans foveal variant” which has not been reported in literature yet and has not been discussed in Pipkins classification either (Figure 2).
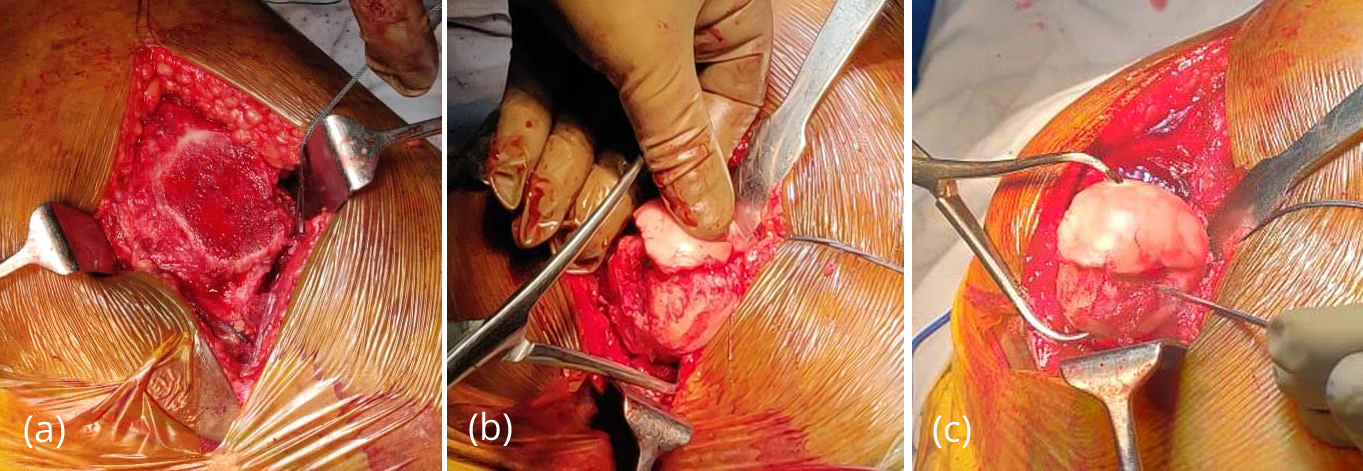
Figure 2: (a) Intraoperative pictures showing flip trochanteric osteotomy; (b) depicting provisional reduction of fracture fragment with reduction; (c) depicting k wire pointing towards the fovea centralis- indicating a trans foveal extent of fracture.
We further reduce this fragment provisionally with k wires and then secured it with two 3mm HCS (headless compression screw). Joint was examined thoroughly for any other loose fragment following which hip reduced and capsular repair was done. Two 4.5 mm screws were used to secure trochanteric osteotomy (Figure 3). Patient was further operated for volar Barton fracture in the same sitting with distal end radius anatomical volar locking plate.
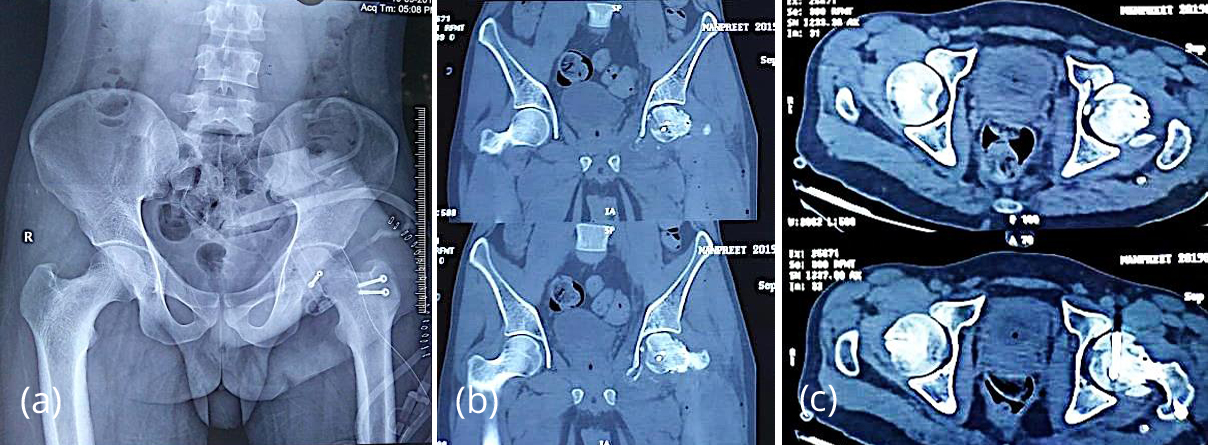
Figure 3: (a) Post op X ray; (b & c) Post-operative CT scan showing concentric reduction of hip with two 3mm Herbert screw fixation of trans-foveal fragment of femur head.
Discussion
The AO principle of anatomical reduction holds true for femur head fracture, like any other intra- articular fracture. Over decades, several classification systems have been proposed for femur head fracture [6-9]. Brumback et al, gave a more comprehensive classification than Pipkins taking into account the joint stability and direction of dislocation [7] Likewise, Yoon et al. modified Pipkins classification and had taken fracture fragment size into account. They described type 1 as a small head fragment caudal to fovea; type 2 as large fragment caudal to fovea; type 3 as large fragment cephalad to fovea; and type 4 as comminuted head fragment [6]. Despite of this, Pipkins classification still being most widely used among surgeons in day to day practice. The major drawbacks of this classification is that it does not consider the ability of achieving and maintaining a concentric reduction, fracture fragment size and displacement and the characteristics of the associated acetabular fracture in Type 4 injuries [5]. The original Pipkins classification, based on 24 patients, described type 1 as infra-foveal, type 2 as supra-foveal, type 3 as type 1 or 2 with associated femur neck fracture and type 4 as type 1 or 2 with associated acetabulum fracture [8]. There is no entity termed as “trans- foveal variant” of Pipkins fracture that could be traced in any published literature including the original Pipkins classification.
We came across a unique and unaddressed variant of Pipkins fracture that has not been described before. In all preoperative radiography, it was labelled as Pipkins type 2/Yonk type 3 (Supra-foveal, displaced) fracture. Since Pipkins type 2 fractures are present in weight bearing zone, open reduction is always preferred, particularly in displaced fragments so as to achieve anatomical reduction. At our center, we prefer Ganz safe surgical dislocation over anterior Smith Peterson approach. Contrary to anterior approach, patient was in lateral decubitus position and Kocher langenbeck incision was given, followed by flip osteotomy of greater trochanter so as to protect the deep branch of medial circumflex femoral artery under obturator externus muscle. This is a key step that actually prevents any further vascular insult to femoral head and further reduces the chances of avascular necrosis. Following the Z-shaped anterior capsulotomy, the hip was dislocated anteriorly by traction and external rotation. Intraoperatively, it was observed that the fracture line was crossing both superior and inferior to fovea. This is, contrary to, preoperative images and such variant has not been reported in literature so far. The fragment was finally fixed with 2 headless compression screws and the hip cavity was explored for any loose fragments.
The “trans-foveal” variant is usually a large fragment extending both above and below the fovea and involves weight bearing region of femoral head, hence surgical fixation is warranted. Further, the operating surgeon needs to be aware of existence of such variant that might be misinterpreted even on preoperative imaging and CT scan. This manuscript is written to bring to light a fallacy of Pipkins classification and how we encountered it in our surgical approach.
Conclusion
Femoral head fracture has variable characters so it is imperative that surgeon should be well versed with the intricate details of anatomy of hip joint. Pipkins classification is most widely accepted classification for femur head fracture. Trans-foveal variety is not discussed in literature so far. As per the authors, this is the first reported case of trans-foveal femoral head fracture with posterior hip dislocation. Research involving human participants All procedures were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent Informed consent was obtained from all individual participants included in the study.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Hougaard K, Thomsen PR. Traumatic posterior fracture dislocation of the hip with fracture of the femoral head. J Bone Joint Surg Am. 1988; 70(2):233–239.
[2] Roeder LF, DeLee JC. Femoral head fractures associated with posterior hip dislocation. Clin Orthop Relat Res. 1980; 147:121–130.
[3] Sahin V, Karakaş ES, Aksu S, Atlihan D, Turk CY, et al. Traumatic dislocation and fracture-dislocation of the hip. A long-term follow-up study. J Trauma. 2003; 54(3):520–529.
[4] Stewart MJ, Milford LW. Fracture dislocation of the hip: an end-result study. J Bone Joint Surg Am. 1954; 36(A:2):315–342.
[5] Romeo NM, Firoozabadi R. Classifications in Brief: The Pipkin Classification of Femoral Head Fractures. Clin Orthop Relat Res. 2018; 476(5):1114-1119.
[6] Yoon TR, Rowe SM, Chung JY, Song EK, Jung ST, et al. Clinical and radiographic outcome of femoral head fractures: 30 patients followed for 3–10 years. Acta Orthop Scand. 2001; 72(4):348–353.
[7] Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip. 1987:181–206.
[8] Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957; 39(5):1027–1042.
[9] Tonetti J, Ruatti S, Lafontan V, Loubignac F, Chiron P, et al. Is femoral head fracture-dislocation management improvable: a retrospective study in 110 cases. Orthop Traumatol Surg Res. 2010; 96(6):623–631.
[10] Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, et al. Surgical dislocation of the adult hip: a technique with full access to the femoral head and acetabulum without risk of avascular necrosis. J Bone Joint Surg Br. 2001; 83(8):1119–1124.