Full Text
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disorder that primarily affects the axial skeleton, leading to progressive spinal rigidity and deformity. With disease progression, patients often develop significant thoracolumbar kyphosis, reduced chest wall compliance, and compromised pulmonary function, all of which pose considerable challenges to anaesthetic management during surgical interventions [1]. Airway management in such patients is particularly complex due to restricted cervical spine mobility, temporomandibular joint involvement, and the inability to assume optimal positioning for conventional laryngoscopy [2].
In advanced cases, as in our patient with global kyphotic deformity, conventional airway techniques are often ineffective or dangerous. Awake fiberoptic intubation is regarded as the gold standard in anticipated difficult airways, particularly when neck mobility is severely restricted and alignment for direct laryngoscopy is not feasible [3]. Furthermore, surgical correction of spinal deformities in such patients is associated with prolonged operative time, extensive blood loss, and positioning difficulties, necessitating comprehensive preoperative planning and multidisciplinary coordination.
Ankylosing spondylitis (AS) frequently causes rigid spinal deformity, thoracolumbar kyphosis, and restrictive pulmonary mechanics, severely complicating anesthetic and airway management. Awake fiberoptic intubation is the safest technique when cervical and thoracic spine mobility is severely limited. Recent studies also emphasize multidisciplinary perioperative planning, neuromonitoring, and optimized hemodynamic strategies to mitigate operative risk and improve outcomes [4, 5].
We present a case of an adult female with severe AS and a fixed global kyphotic deformity who underwent successful corrective spinal surgery. This case underscores the importance of thorough airway evaluation, the utility of awake fiberoptic intubation, and meticulous intraoperative management in achieving a favourable anaesthetic outcome in high-risk patients.
Case report
A 43-year-old female, with a body mass index (BMI) of 31 kg/m², was scheduled for corrective spinal deformity surgery due to advanced Ankylosing Spondylitis (AS) with global kyphotic deformity. The patient’s primary complaint was difficulty in standing upright and progressive breathlessness on exertion over the past five years. She also reported severe lower back pain and fatigue while walking short distances. There was a history of trauma while riding in a bus 5 years ago from which she started experiencing the symptoms.
Her medical history included a confirmed diagnosis of AS 4 years ago, with gradually worsening spinal deformity. She was on long-term non-steroidal anti-inflammatory drugs (NSAIDs) and had received physiotherapy intermittently, with a non-relevant history of surgical intervention involving the distal radius bone 1 year back. There was no history suggestive of cardiovascular or metabolic disorders. Family history was significant for a first-degree relative with AS. Genetic testing revealed HLA-B27 positivity.
On physical examination, the patient had a fixed thoracolumbar kyphosis, with the chin resting on the upper chest and severely restricted cervical spine mobility. Mallampati grading could not be assessed due to limited mouth opening and temporomandibular joint stiffness. Chest expansion was markedly reduced. Cardiopulmonary examination was otherwise unremarkable.
Preoperative imaging showed extensive syndesmophyte formation with complete atlanto-occipital assimilation, anterior wedge compression fracture of D11 vertebra and a global kyphotic angle exceeding 80 degrees. Pulmonary function tests revealed moderate restrictive lung disease (FVC: 50% predicted). Routine laboratory investigations were within normal limits.
Anaesthetic management
Due to the anticipated difficult airway and the inability to align for direct laryngoscopy, awake fiberoptic nasal intubation was planned (Figure 1). After premedication with glycopyrrolate and starting on dexmedetomidine infusion for light sedation, airway topicalisation was achieved using 4% lignocaine nebulisation, nasal pledgets with 2% lignocaine and xylometazoline, and transtracheal injection. Fiberoptic bronchoscopy was performed via the right nostril, and a 7.0 mm flexometallic endotracheal tube was railroaded successfully into the trachea under spontaneous ventilation.
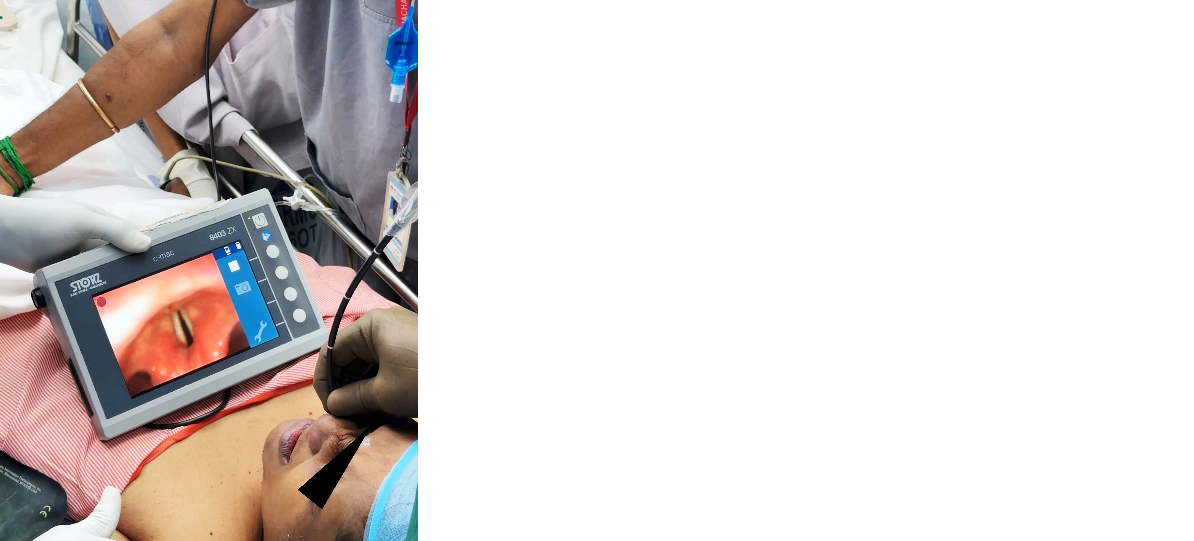
Figure 1: Awake fiberoptic intubation.
General anaesthesia was induced with intravenous fentanyl and propofol, followed by vecuronium for neuromuscular blockade. Anaesthesia was maintained with oxygen, air, and sevoflurane. The patient was positioned in a modified prone posture with extensive padding and continuous pressure point monitoring (Figure 2).

Figure 2: Intraoperative positioning.
Surgery lasted seven hours, with intraoperative blood loss of approximately 2000 mL. Haemodynamic parameters remained stable with guided fluid and blood product replacement: 4 units of packed red blood cells, 4 units of fresh frozen plasma, and 1 unit of platelets.
Postoperative course
The patient was transferred to the intensive care unit (ICU) for elective ventilation. Extubation was performed after 12 hours following full neurological and respiratory recovery. No perioperative complications or airway trauma was observed. The patient was discharged on postoperative day 5 with no neurological deficits.
Discussion
We selected awake fiberoptic intubation as the primary airway intervention in this case of severe ankylosing spondylitis (AS) with global kyphotic deformity, owing to the significant risk of airway compromise and failed intubation with conventional techniques. Given the fixed cervical spine, limited mouth opening, and impaired pulmonary reserve, this approach was the safest and most reliable option to ensure airway security while maintaining spontaneous ventilation.
Awake fiberoptic intubation is the gold standard for anticipated difficult airways, particularly in patients with limited cervical spine mobility or fixed spinal deformities, as seen in advanced AS [6]. AS patients often exhibit ossification of spinal ligaments, atlantoaxial subluxation, and temporomandibular joint stiffness—all of which increase the risk of failed laryngoscopy and traumatic intubation [7, 8]. Additionally, spinal deformities result in restrictive pulmonary physiology, making airway obstruction or apnoea during induction potentially catastrophic [9]. Preserving spontaneous ventilation and adequate oxygenation during intubation, therefore, becomes paramount.
In this case, meticulous preparation, including effective airway topicalisation and sedation, ensured patient comfort and cooperation. The nasal route was preferred due to limited oral access and better alignment in the neutral position. Prior studies have emphasized the importance of pre-procedure counselling, topical anaesthesia, and the use of antisialagogues such as glycopyrrolate to enhance success rates with minimal complications [10, 11].
Our case also highlights the challenges in intraoperative positioning. Global kyphotic deformity prevents standard prone positioning. We used customized bolstering and padding strategies to maintain spinal alignment while preventing pressure injuries and compromising ventilation. Such positioning techniques, though labor-intensive, are essential to avoid perioperative morbidity [12].
Regarding intraoperative management, expected blood loss in extensive spinal surgeries is often high, necessitating proactive transfusion planning. Although newer modalities such as cell salvage and tranexamic acid have shown benefits, our patient was managed effectively with blood component therapy and fluid optimization [13].
The strengths of our approach lie in detailed preoperative planning, the use of a multidisciplinary team, and adherence to best-practice airway guidelines. The case exemplifies the importance of adapting anaesthetic techniques to the patient’s unique anatomical and physiological constraints.
A potential limitation was the lack of preoperative video laryngoscopy evaluation, which could have offered comparative insight into alternative airway strategies. However, the severity of deformity and clinical judgement supported our choice. In similar future cases, the addition of imaging-guided airway assessment or point-of-care ultrasound might improve preparedness further.
Previous case reports have documented the successful use of awake fiberoptic intubation in AS, though outcomes have varied based on the extent of deformity, patient cooperation, and institutional experience [14, 15]. Compared to those reports, our case was notable for the presence of a global (not segmental) kyphosis and the extended surgical duration, which posed additional challenges. Yet, the absence of intraoperative or postoperative airway or neurological complications underlines the effectiveness of our approach.
Conclusion
This case reinforces the pivotal role of awake fiberoptic intubation in anticipated difficult airways due to fixed spinal deformities. A thorough understanding of the patient’s pathology, coupled with anticipatory planning, multidisciplinary coordination, and vigilant perioperative care, can lead to safe and successful outcomes in high-risk anaesthetic scenarios. The primary take-away from this case is the uncompromising need to individualize airway and anaesthetic strategies in patients with severe ankylosing spondylitis undergoing complex spine surgeries.
Acknowledgements
The Department of Spine Surgery and the surgical team at Sri Ramachandra Institute of Higher Education and Research for their support in intra-operative management.
Conflicts of interest
Authors declare no conflict of interest.
References
[1] Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007; 369:1379–1390.
[2] Kim H, Lee CJ, Lee SC. Anesthetic management of a patient with ankylosing spondylitis undergoing total hip arthroplasty. Korean J Anesthesiol. 2011; 60:290–293.
[3] Heidegger T, Gerig HJ, Ulrich B, Schnider TW. Validation of a simple algorithm for tracheal intubation: daily practice is the key to success in emergencies. Anesth Analg. 2001; 92:517–522.
[4] Limalvin NP, Sathiyapriya V, Rajkumar S, Mahalakshmi M, Pradeep S. Difficult airway management in an ankylosing spondylitis patient with severe cervical spine and temporomandibular involvement: successful video‑laryngoscope use in emergency. Int J Res Med Sci. 2023; 11:2279–2883.
[5] Luo J, Wu T, Yang Z, Liu H, Zhang Y, et al. An effective strategy for treatment of severe kyphosis secondary to ankylosing spondylitis: one‑level modified osteotomy combined with shoulders lifting correction method. J Orthop Surg Res. 2024; 19:536.
[6] Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, et al. Practice Guidelines for Management of the Difficult Airway: An Updated Report. Anesthesiology. 2013; 118:251–270.
[7] Turkstra TP, Craen RA, Pelz DM. Cervical spine motion: a fluoroscopic comparison during intubation with lighted stylet, GlideScope®, and Macintosh laryngoscope. Anesth Analg. 2005; 101:910–915.
[8] Kapoor MC. Anaesthetic considerations in ankylosing spondylitis. Indian J Anaesth. 2016; 60:10–15.
[9] Ranganathan V, Gracey E, Brown MA, Inman RD, Haroon N. Pathogenesis of ankylosing spondylitis – recent advances and future directions. Nat Rev Rheumatol. 2017; 13:359–367.
[10] Crosby ET. An evidence-based approach to airway management: is there a role for clinical practice guidelines? Anesthesiology. 2004; 100:1004–1005.
[11] Ovassapian A. Fiberoptic Endoscopy and the Difficult Airway. Anesthesiol Clin North America. 2001; 19:755–771.
[12] McBeth PB, Ball CG, Mulloy RH, Kirkpatrick AW, Vogt KN, et al. Spine trauma management: a protocol for all patients with ankylosing spondylitis. Can J Surg. 2009; 52:30–34.
[13] Verma K, Errico TJ, Lonner BS. Surgical management of severe spinal deformity in ankylosing spondylitis. Spine. 2010; 35:1520–1525.
[14] Gupta S, Kulkarni M, Naphade R, Patel D, Joshi R. Anesthetic management of a patient with severe kyphosis and difficult airway: a case report. Egypt J Anaesth. 2015; 31:173–176.
[15] Sun L, Dong X, Fu X, Zhang Y, Li M, et al. Management of airway in patients with ankylosing spondylitis: a retrospective study. Medicine (Baltimore). 2018; 97:10923.