Case Report
2025
December
Volume : 13
Issue : 4
Navigating the shunt: Anaesthetic challenges in a child with pulmonary arteriovenous malformation undergoing endovascular embolisation
Sugganya N, Manickam A, Aravindan M, Akilandeswari M
Pdf Page Numbers :- 448-452
Sugganya N1, Akilandeswari Manickam1, Aravindan M1 and Akilandeswari M1,*
1Department of Anesthesiology and Pain Medicine, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India
*Corresponding author: Dr. Akilandeswari M, Professor, Department of Anesthesiology and Pain Medicine, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. Email: akilaanes@gmail.com
Received 6 August 2025; Revised 18 September 2025; Accepted 1 October 2025; Published 13 October 2025
Citation: Sugganya N, Manickam A, Aravindan M, Akilandeswari M. Navigating the shunt: Anaesthetic challenges in a child with pulmonary arteriovenous malformation undergoing endovascular embolisation. J Med Sci Res. 2025; 13(4):448-452. DOI: http://dx.doi.org/10.17727/JMSR.2025/13-79
Copyright: © 2025 Sugganya N et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Hereditary hemorrhagic telangiectasia (HHT) is a rare autosomal dominant disorder characterized by mucocutaneous telangiectasias and arteriovenous malformations (AVMs) involving the lungs, brain, and liver. These vascular abnormalities predispose affected individuals to hypoxemia, paradoxical embolism, hemorrhage, and neurological complications. Thorough perioperative evaluation and an individualized anaesthetic strategy are essential to ensure safe endovascular embolisation, particularly in the pediatric population, where physiological reserves are limited. We report the anaesthetic management of a child with pulmonary and parietal AVMs who presented with acute unresponsiveness and required urgent endovascular embolisation of a pulmonary AVM. The primary anaesthetic goals included prevention of systemic air embolism, maintenance of oxygenation, preservation of hypoxic pulmonary vasoconstriction, and avoidance of haemodynamic instability. The procedure was successfully performed under carefully titrated intravenous sedation with advanced monitoring, including continuous capnography, invasive arterial blood pressure measurement, and vigilant neurological assessment. No intraoperative adverse events occurred, and the child had an uneventful recovery. This case emphasises the importance of meticulous perioperative planning, vigilant monitoring, and tailored anaesthetic techniques when managing pediatric patients with HHT undergoing endovascular interventions. Awareness of the unique pathophysiological implications of pulmonary AVMs is critical for ensuring safe anaesthetic care in this vulnerable population.
Keywords: hereditary hemorrhagic telangiectasia; pulmonary arteriovenous malformation; pediatric anaesthesia; hypoxic pulmonary vasoconstriction
Full Text
Introduction
Hereditary hemorrhagic telangiectasia (HHT) is a genetic vascular dysplastic disorder characterized by abnormal direct connections between arteries and veins without intervening capillary beds [1]. The site, size, and number of malformations present on mucocutaneous surfaces or within major organs determine the clinical presentation and disease severity [1]. Pulmonary arteriovenous malformations (PAVMs) can result in significant right-to-left shunting, causing hypoxemia without respiratory distress, as well as ischemic stroke and cerebral abscess due to paradoxical embolism [2]. Coexisting cerebral AVMs further increase the risk of hemorrhagic stroke and secondary seizures [2]. Endovascular embolisation is now considered the standard of care for PAVMs, with success rates exceeding 90% [4].
Anaesthetic management for embolisation requires a thorough understanding of the disease process and its systemic implications. The pharmacodynamic effects of anaesthetic agents on pulmonary and systemic circulation influence the magnitude of right-to-left shunting and thus impact end-organ oxygen delivery during the procedure [5]. Additionally, the presence of intracranial AVMs necessitates meticulous control of blood pressure to preserve cerebral perfusion and minimise the risk of rupture [6]. Total intravenous anaesthesia (TIVA) with propofol and remifentanil administered via target-controlled infusion offers advantages by preserving hypoxic pulmonary vasoconstriction, enabling stable haemodynamics, and facilitating rapid recovery critical components in minimising pulmonary shunt and protecting cerebral autoregulation [3,7].
This case report highlights the unique clinical challenges posed by the coexistence of pulmonary and parietal AVMs in a child and describes the anaesthetic strategies employed during endovascular embolisation.
Case presentation
A twelve-year-old child weighing 35 kg, with no known prior medical illness, presented with sudden unresponsiveness accompanied by seizure-like movements and recurrent vomiting. The child was intubated, stabilised at a private hospital, and subsequently referred to our centre with a CT diagnosis of an arteriovenous (AV) malformation in the left occipital lobe supplied by branches of the left posterior cerebral artery. On arrival, the child was responsive to verbal commands (GCS 10T/15). Oxygen saturation was 74% despite an FiO₂ of 1.0. Blood pressure was 90/52 mmHg and the respiratory rate was 18/min. Cardiac examination revealed normal heart sounds without murmurs, and bilateral basal crepitations were audible on auscultation. Neurological examination showed no focal deficits, and pupils were equal and reactive to light. Baseline haematological and metabolic parameters were within normal limits (Table 1). ECG demonstrated sinus tachycardia with T-wave inversion in leads II, III, and aVF. Transthoracic echocardiography revealed a structurally normal heart with good biventricular function and normal pulmonary artery pressures.
Contrast echocardiography with agitated saline demonstrated microbubbles entering the left atrium from the right side, suggestive of a pulmonary arteriovenous malformation (PAVM). Digital subtraction angiography revealed multiple small cerebral AVMs and diffuse pulmonary AVMs in both the upper and lower lobes of the right lung, the largest measuring 5.79 mm findings consistent with hereditary hemorrhagic telangiectasia (Figure 1). After multidisciplinary evaluation, the child was scheduled for transcatheter endovascular embolisation of the pulmonary AVM. The patient was stabilised with antiepileptic medications as per neurological guidance, and intravenous antibiotics were initiated due to bilateral heterogeneous infiltrates on chest radiography. The neurosurgical team advised conservative management with regular follow-up for the cerebral AVM.
Table 1: Preoperative investigations.
|
Parameters
|
Values
|
Reference values
|
|
Hemoglobin (g/dL)
|
18.1
|
13.0-17.0
|
|
Total count(cells/cu.mm)
|
17790
|
4000-11000
|
|
Platelet count(lakhs/mm3)
|
2.50
|
1.5-4.5
|
|
Prothrombin time(seconds)
|
13.3
|
10.8-12.9
|
|
Control
|
11.8
|
|
|
International normalized ratio
|
1.16
|
|
|
Partial thromboplastin time(seconds)
|
28.9
|
22.7-27.5
|
|
Control
|
24.8
|
|
|
Blood urea nitrogen (mg/dL)
|
10
|
7.9-20.1
|
|
Creatinine(mg/dL)
|
0.5
|
0.5-1.2
|
|
Sodium(mmol/L)
|
137
|
136-146
|
|
Potassium(mmol/L)
|
4.2
|
3.5-5.1
|
|
Chloride(mmol/L)
|
105
|
101-109
|
|
Bicarbonate(mmol/L)
|
17
|
21-31
|
The patient was classified as ASA–PS III and planned for the procedure under intravenous moderate sedation with full haemodynamic monitoring. Standard monitoring included ECG, invasive arterial blood pressure, SpO₂, EtCO₂, and axillary temperature measurement. Serial arterial blood gas analysis and hourly urine output monitoring were performed. Sedation depth was assessed intraoperatively using the Ramsay Sedation Score.
Balanced salt solution was administered at 50 mL/hour. All intravenous lines, infusion tubing, and injection ports were meticulously primed to eliminate air and prevent inadvertent systemic air embolism.
Oxygen was delivered through a closed-circuit breathing system with an FiO₂ of 1.0. Intravenous sedation was maintained using a propofol infusion at 1–2 mg/kg/hour, supplemented with fentanyl at an initial bolus dose of 2 mcg/kg. Femoral vascular access was obtained under ultrasound guidance after local infiltration with 2% lignocaine. The dilated feeders supplying the right lower lobe AVMs were embolised using vascular plugs (Figure 2). The procedure lasted approximately two hours, and analgesia was reinforced with fentanyl 0.5 mcg/kg administered at hourly intervals.
Systolic blood pressure was maintained between 100–120 mmHg, and heart rate between 85–95 bpm. During embolisation, oxygen saturation improved from 77% at baseline to 85%. The patient was extubated two hours later in the paediatric critical care unit. As part of a staged management plan, the child subsequently underwent re-embolisation of the middle lobe pulmonary AVM.
Table 2: Serial ABG’S.
|
Parameter
|
Pre-operative
|
Pre-operative
|
Intra-operative
|
Post-operative
|
|
FiO2
|
1
|
0.4
|
1
|
1
|
|
Ph
|
7.408
|
7.346
|
7.313
|
7.324
|
|
PCO2‚ (mmHg)
|
46.3
|
40.8
|
45.8
|
43.6
|
|
PO2 (mmHg)
|
30.5
|
42.5
|
55.5
|
58.5
|
|
HCO3- (mmol/L)
|
18.8
|
21.8
|
22.7
|
22.2
|
|
Na+ (mmol/L)
|
136.6
|
134.3
|
134.7
|
138.1
|
|
K+ (mmol/L)
|
3.48
|
3.85
|
3.48
|
3.29
|
|
Ca2+ (mmol/L)
|
0.661
|
1.100
|
0.934
|
1.141
|
|
Cl- (mmol/L)
|
99.1
|
98.8
|
99.1
|
101.5
|
|
Lactate (mmol/L)
|
1.05
|
1.82
|
0.79
|
0.85
|
|
Hemoglobin (g/dL)
|
18.95
|
15.27
|
14.39
|
13.98
|
|
Oxygen Saturation (%)
|
83.1
|
72.8
|
84.8
|
94
|
|
Glucose (mg/dL)
|
105.0
|
94
|
93.5
|
89.1
|
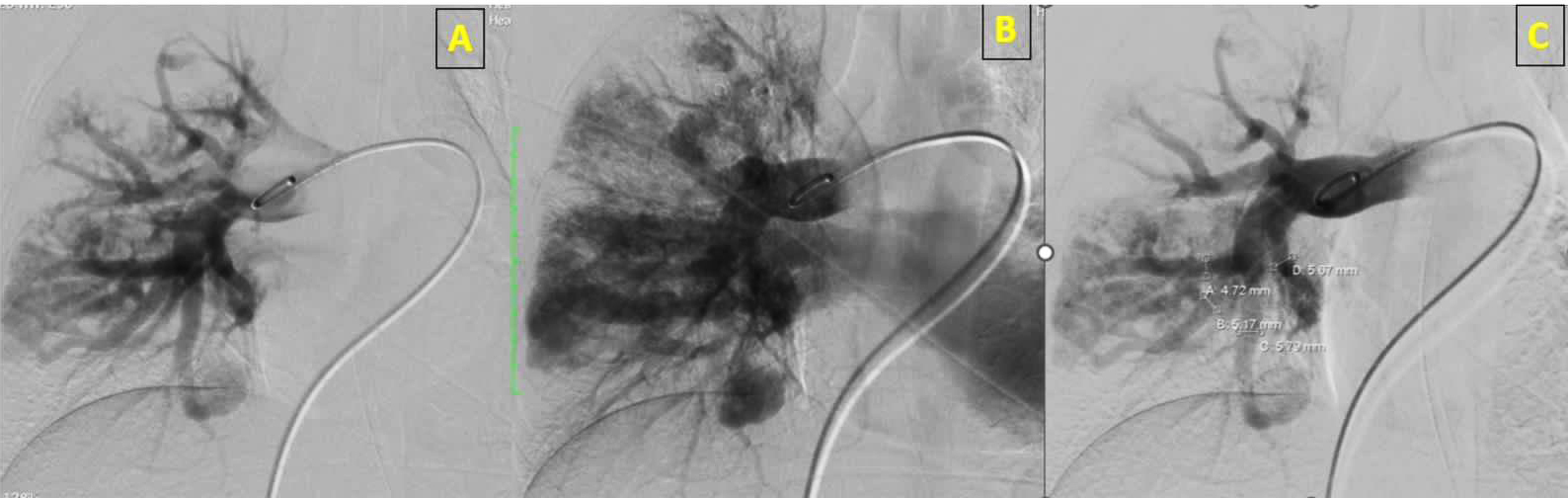
Figure 1: Pulmonary arteriovenous malformation in the middle lobe of the lung.

Figure 2: Post embolisation of the pulmonary AVM.
Discussion
Hereditary hemorrhagic telangiectasia (HHT) is suspected when the classical triad of recurrent epistaxis, mucocutaneous telangiectasias, and a positive family history is present [16]. The development of visible telangiectasias may be delayed in children, and epistaxis is often the earliest and most frequently reported symptom [17]. In contrast, our patient presented with an acute alteration in consciousness with suspected seizure-like activity, without any prior history of epistaxis or relevant family history. Pulmonary arteriovenous malformation (PAVM) was suspected due to persistent hypoxemia unresponsive to high FiO₂, consistent with a significant right-to-left shunt. Bubble echocardiography and digital subtraction angiography confirmed the diagnosis, and embolisation was planned. Endovascular embolisation, followed by periodic surveillance, is now the standard of care for PAVMs, with success rates exceeding 90% [4].
Anaesthetic management should focus on strategies that maintain oxygenation without worsening the right-to-left shunt, prevent paradoxical air embolism, and maintain stable haemodynamics to preserve the transmural pressure gradients across cerebral AVMs [18]. Maintaining cerebral perfusion pressure is essential in the background of baseline hypoxemia to prevent ischaemic stroke, while avoiding sudden blood pressure surges that may precipitate haemorrhagic stroke [2,7]. The magnitude of right-to-left shunting is dynamic and may worsen with positive pressure ventilation and volatile anaesthetic–induced attenuation of hypoxic pulmonary vasoconstriction (HPV) [11,2]. Total intravenous anaesthesia (TIVA) using propofol and fentanyl has been shown to preserve HPV, a crucial physiological mechanism in such cases [2,8]. Propofol additionally reduces intracranial pressure and cerebral metabolic oxygen consumption, providing neuroprotection during interventions involving cerebral AVMs [9]. For these reasons, we used continuous propofol infusion with preserved spontaneous ventilation, thereby minimising further desaturation. During airway management, gentle laryngoscopy-guided intubation is advisable, and nasal airways or nasogastric tubes should be avoided because of the high risk of bleeding [19].
Vigilant intraoperative monitoring, including continuous capnography, invasive arterial pressure measurement, oxygen saturation, and depth of sedation, is essential in the interventional suite to promptly identify respiratory depression or excessive sedation [12]. Haemodynamics were maintained within 20% of baseline values to minimise the risk of AVM rupture, consistent with published recommendations advocating tight blood pressure control [13–15].
The risks of contrast-induced nephropathy and embolic complications were addressed by maintaining euvolemia, thus preventing blood sludging associated with secondary polycythemia. All procedures were performed under strict aseptic precautions, along with broad-spectrum antibiotic prophylaxis, to minimise the risk of bacteremia and subsequent cerebral abscess formation, and close monitoring was ensured for post-embolisation reperfusion-related bleeding [12].
Pediatric pharmacokinetic and pharmacodynamic considerations are vital, as children exhibit different distribution volumes and propofol clearance profiles compared to adults [10]. TIVA remains a favourable technique in pediatric patients due to its rapid onset, haemodynamic stability, and predictable recovery characteristics.
Conclusion
Given the rarity and complex nature of hereditary hemorrhagic telangiectasia, a multidisciplinary preoperative evaluation combined with meticulous anaesthetic planning is essential to prevent worsening shunting and its associated complications. A carefully tailored approach, guided by detailed preoperative imaging and the planned endovascular intervention, is crucial to optimising perioperative safety and improving patient outcomes.
Acknowledgement
Radiological intervention team of Sri Ramachandra Institute of Higher Education and Research for their intraoperative support.
Conflict of Interest
Authors declare that there is no conflict of interest.
References
[1] Majumdar S, McWilliams JP. Approach to pulmonary arteriovenous malformations: a comprehensive update. J Clin Med. 2020; 9:1927.
[2] Ryan KM, Siegler E. Pyogenic brain abscess associated with an incidental pulmonary arteriovenous malformation. BMJ Case Rep. 2022; 15:252794.
[3] Hosman AE, de Gussem EM, Balemans WAF, Kelder JC, Zanen P, et al .Screening children for pulmonary arteriovenous malformations: evaluation of 18 years of experience. Pediatr Pulmonol. 2017; 52:1206–1211.
[4] Contegiacomo A, Del Ciello A, Rella R, Russo U, Giurazza F,et al. Pulmonary arteriovenous malformations: what the interventional radiologist needs to know. Radiol Med. 2019; 124:973–988.
[5] Hagerman A, Licker M. Anesthesia, mechanical ventilation, and hypoxic pulmonary vasoconstriction. In: Cohen’s Comprehensive Thoracic Anesthesia. 2022. p.193–212.
[6] Nico E, Hossa J, McGuire LS, Alaraj A. Rupture–risk stratifying patients with cerebral arteriovenous malformations using quantitative hemodynamic flow measurements. World Neurosurg. 2023;179:68–76.
[7] Natanagara IG, Suarjaya IP, Sutawan IB. Navigating frontal lobe arteriovenous malformation resection: a case report on TIVA with propofol–remifentanil TCI for hemodynamic stability and ICP control. Bioscientia Med J Biomed Transl Res. 2025; 9:8290–8304.
[8] Jones J, Ahmad FI. Anesthesia for free flap reconstruction after head and neck surgical resection. In: Oncologic Critical Care. 2019. p. 1–15.
[9] Kumar R, Singh A, Sharma D. Anesthetic management of intracranial arteriovenous malformation surgery using total intravenous anesthesia: a case report and review of perioperative considerations. J Neurosurg Anesthesiol. 2023;35(4):412–417.
[10] Wira Natanagara IGC, Suarjaya IPP, Sutawan IBKJ. TIVA with propofol–remifentanil TCI in AVM resection. Bioscientia Med J Biomed Transl Res. 2025; 9:8290–8304.
[11] Anesthesia and intracranial arteriovenous malformation management. Neurosurg Focus. 2001; 11:E6.
[12] Kaufman CS, Nguyen MA, Borczuk AC, McWilliams JP. Pediatric pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: screening, diagnosis, and management. J Clin Med. 2025; 14:3739.
[13] Pieffer R. Anesthetic considerations in cerebral AVM. CureHHT.org. 2009 [Internet]. Available from: https://curehht.org.
[14] Meek ME, Meek JC, Beheshti MV. Management of pulmonary arteriovenous malformations. Semin Intervent Radiol. 2011; 28:24–31.
[15] Kim JC, Lee KC, Choi JJ, Lee HD, Kwak HJ. Anesthetic management of a patient with pulmonary arteriovenous malformation under total intravenous anesthesia: a case report. Korean J Anesthesiol. 2009; 56:713–716.
[16] Robinson D, Rogers B, Kapoor R, Swan J, Speas G, et al. Anesthetic considerations for a patient with hereditary hemorrhagic telangiectasia undergoing a thoracoscopic maze procedure for atrial fibrillation. J Investig Med High Impact Case Rep. 2014; 2:2324709614553669.
[17] Ortman C, Ortolani E. Hereditary hemorrhagic telangiectasia: a pediatric–focused review. Semin Pediatr Neurol. 2024; 52:101167.
[18] Kamimura Y, Nakanishi T, Sato A. Anesthetic considerations for cesarean delivery in a parturient with hereditary hemorrhagic telangiectasia: a case report. JA Clin Rep. 2021; 7:19.
[19] Faughnan ME, Mager JJ, Hetts SW, Palda VA, Lang–Robertson K, et al. Second International Guidelines for the Diagnosis and Management of Hereditary Hemorrhagic Telangiectasia. Ann Intern Med. 2020; 173:989–1001.