Full Text
Introduction
The most common type of carcinoma diagnosed in the world is Breast cancer. There were an estimated 2.3 million women diagnosed with breast cancer and 670 000 deaths globally in 2022. In India breast cancer is the most common cancer with 2.2 lakh cases reported in 2022 with a need for specific studies in different areas of India [1].
The breast cancer is a heterogenous disease which can be classified into molecular subtypes as per the St. Gallen Consensus (2011) depending on the expression of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER 2) by immunohistochemistry (IHC) markers, the breast carcinoma’s molecular subtypes are Luminal A, Luminal B [ Luminal B (HER 2 positive) and Luminal B (HER 2 negative)], HER 2 Enriched and Triple negative [4]. Ki- 67 levels are used to determine the molecular subtype, guide the therapy, predict outcomes and assess the aggressiveness of breast cancer. Molecular subtypes help in guiding the treatment and for better prognosis.
Globally, luminal A is the most common molecular subtype of breast cancer. However, in India, several institutional studies have reported a higher prevalence of luminal B and triple-negative subtypes, with triple-negative breast cancer being disproportionately common compared to Western populations [2,3]. Triple negative, HER 2 enriched and luminal B subtypes are associated with higher grades and higher rates of relapse whereas luminal A is associated with lower grades with better prognosis [5]. Studies in South India breast cancer shows it is frequently diagnosed in younger women with high prevalence of aggressive subtypes particularly triple negative and luminal B [6, 7].
This study aims to describe the distribution of age and tumor grade across breast cancer molecular subtypes and assess their associations. It will also examine variation in the Ki-67 proliferation index among subtypes. Frequencies and proportions will be calculated for each variable by subtype, with associations analyzed using the Chi-square test, and Ki-67 levels compared across subtypes to evaluate differences in proliferative activity.
Materials and methods
Retrospective cohort study was conducted on 500 consecutive cases of invasive breast carcinoma diagnosed at Krishna Institute of Medical Sciences, Secunderabad, Telangana, after receiving approval from the ethics committee. The data was collected from February 2023 to August 2025.
Inclusion criteria: Histopathologically confirmed invasive breast carcinoma cases with available data on age at diagnosis, histologic grade, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor 2 (HER 2) and Ki – 67 were included in the study.
Exclusion criteria: Cases lacking essential data for molecular subtyping or Ki – 67 assessment or pure ductal carcinoma in situ were excluded. Male breast carcinoma cases were excluded.
Data for this study were obtained from pathology reports and electronic medical records. Immunohistochemistry (IHC) results for estrogen receptor (ER), progesterone receptor (PR), HER2, and Ki-67 were retrieved for each patient. Tumor histologic grade was recorded as reported by the examining pathologist.
The variables assessed in this study included age at diagnosis, histologic tumor grade, hormone receptor status, HER2 status, and the Ki-67 proliferation index. Age at diagnosis was analyzed as a continuous variable and categorized into 21–30, 31–40, 41–50, 51–60, 61–70, 71–80, and 81–90 years, as well as dichotomized into ≤50 years and >50 years. Histologic tumor grade was recorded as Grade I, II, and III. Estrogen receptor (ER) and progesterone receptor (PR) status were determined by immunohistochemistry (IHC), with ER positivity defined as ≥1% tumor cell nuclei staining in accordance with current guidelines. HER2 status was assessed using IHC (0–3+), with fluorescence in situ hybridization (FISH) performed for equivocal (2+) cases; HER2 positivity was defined as IHC 3+ or FISH amplification, whereas HER2 negativity was defined as IHC 0–1+ or non-amplified FISH results when applicable. The Ki-67 proliferation index was reported as the percentage of tumor cell nuclei positive for Ki-67, with a value of ≥15% considered indicative of high proliferative activity.
Molecular subtypes definitions
Molecular subtypes of breast cancer were classified according to the criteria proposed by the St. Gallen 2011 Consensus. Tumors were categorized as luminal A if they were ER and PR positive, HER2 negative, and exhibited low Ki-67 levels (≤15%). Luminal B tumors were further subdivided into luminal B(HER2-positive), defined as ER and PR positive with HER2 overexpression and any Ki-67 level, and luminal B (HER2-negative), defined as ER and PR positive, HER2 negative, and Ki-67 >15%. HER2-enriched tumors were characterized by HER2 positivity with negative ER and PR status, while triple-negative tumors lacked expression of ER, PR, and HER2.
Statistical analysis
Association between molecular subtypes with histological grade and age were evaluated by Chi-square test. In this study the significance level was taken as p <0.05. Microsoft Excel was used for statistical analysis and data processing.
Results
500 cases diagnosed with invasive breast carcinoma at Krishna Institute of Medical Sciences were included in the study. The mean age was 56.45 +/- 12.21 with an age range of 25 to 89 years. The majority of patients diagnosed with breast cancer were > 50 years with 67.2 % (n = 336) and 32.8% (n = 164) were </= 50 years. The Demographic and Clinical characteristics of the study are summarized in Table 1.
Table 1: Demographic and Clinical characteristics of the study.
|
Parameter
|
Number of patients (%)
|
|
Age (Mean +/- SD)
|
56.45 +/- 12.20
|
|
</= 50 years
|
164 (32.8%)
|
|
>50 years
|
336 (67.2%)
|
Predominant histologic subtype of breast cancer was invasive breast carcinoma of no specific type (90.6 %), followed by mucinous carcinoma (3.8 %) (Figure 1), invasive lobular carcinoma (2.6%), invasive papillary carcinoma (1.4 %), invasive solid papillary carcinoma (1%), invasive micropapillary carcinoma (0.4%) and tubular carcinoma (0.2 %) (Figure 2).
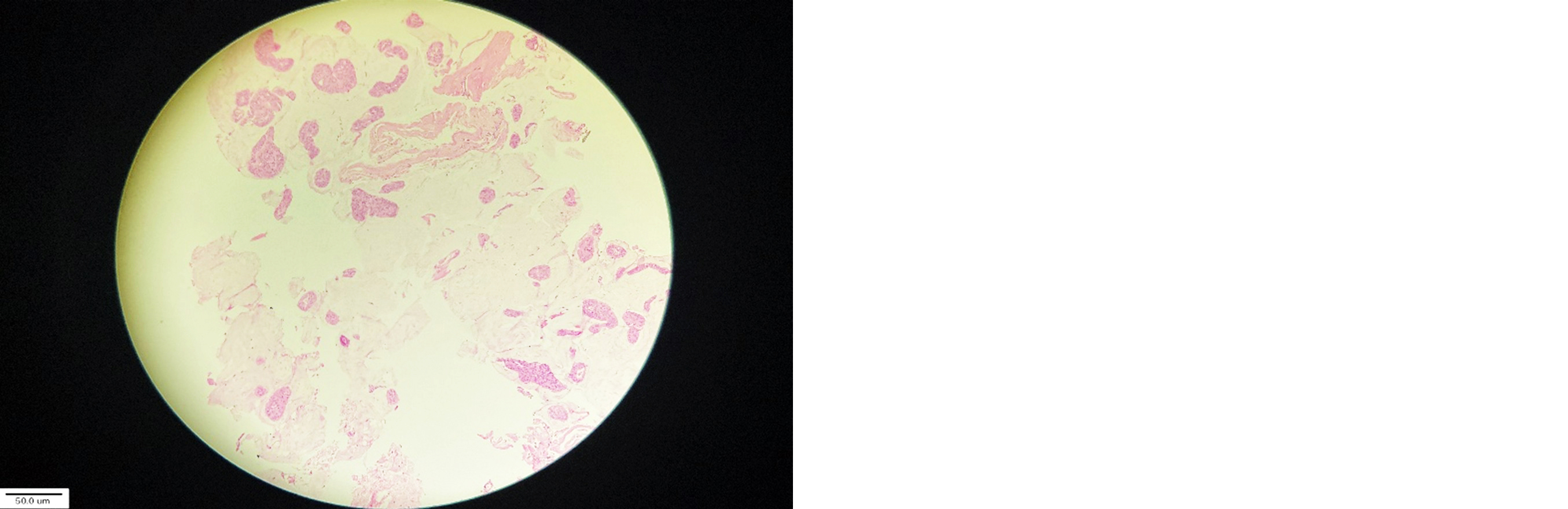
Figure 1: Mucinous carcinoma 40X.
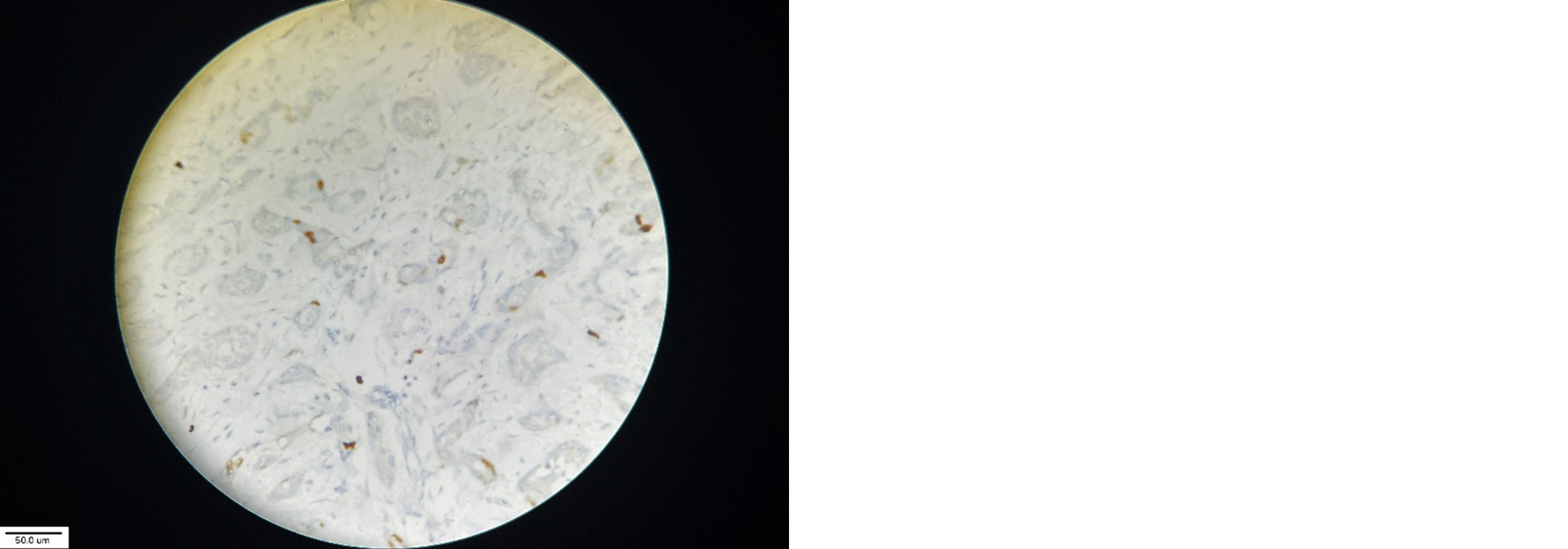
Figure 2: Tubular carcinoma 40X.
According to Nottingham grade classification, tumors were classified into Grade I, II and III. Grade I with 16.6 % (n = 83), Grade II with 53.6% (n = 268) and Grade III with 29.8 % (n = 149). The immunohistochemistry study showed that invasive breast carcinoma cases were ER positive in 347 patients (69.4%) (Figure 3), PR positive in 347 patients (69.4%) (Figure 4) and HER 2 positive in 119 patients (23.8%). The study showed the high Ki-67 (-->15%) was observed in 354 patients (70.8%) (Figure 5). High Ki-67 was shown in luminal B (HER 2 Negative) in 161(100 %), luminal A in 0 (0 %), luminal B (HER 2 Positive) in 45(90 %), HER 2 Enriched in 66(95.6 %) and Triple Negative in 82 (97.6 %) (Figure 6).
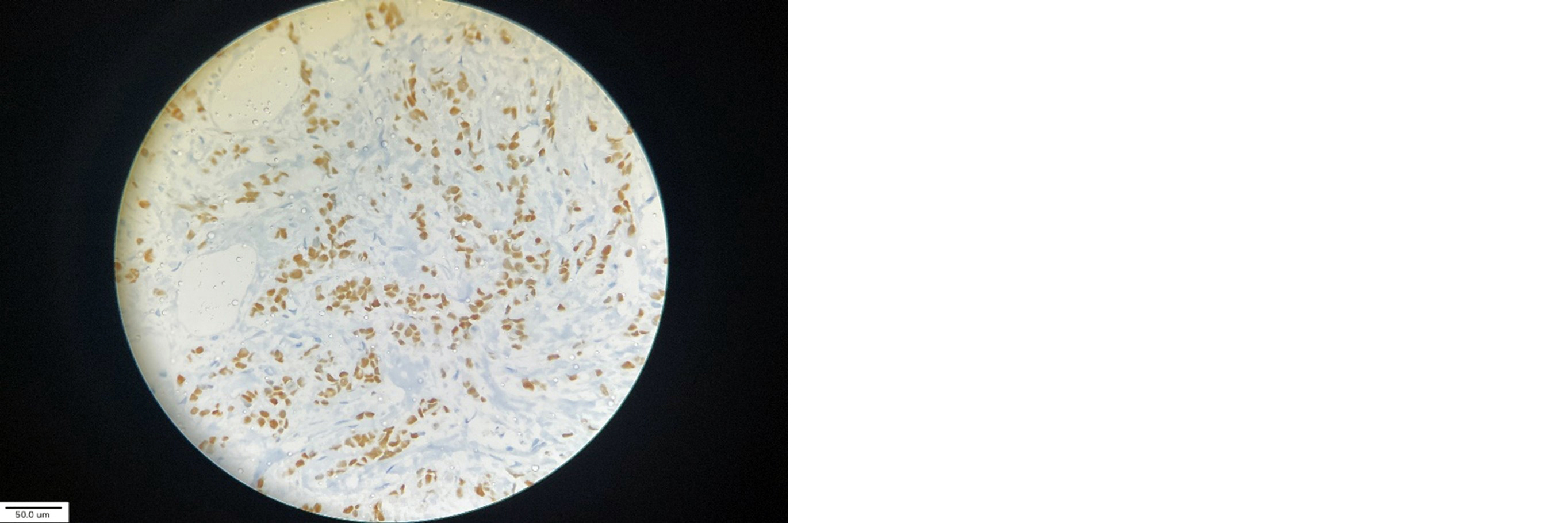
Figure 3: Immunohistochemical staining demonstrates nuclear positivity for estrogen receptor (ER) in tumor cells “x 40”.
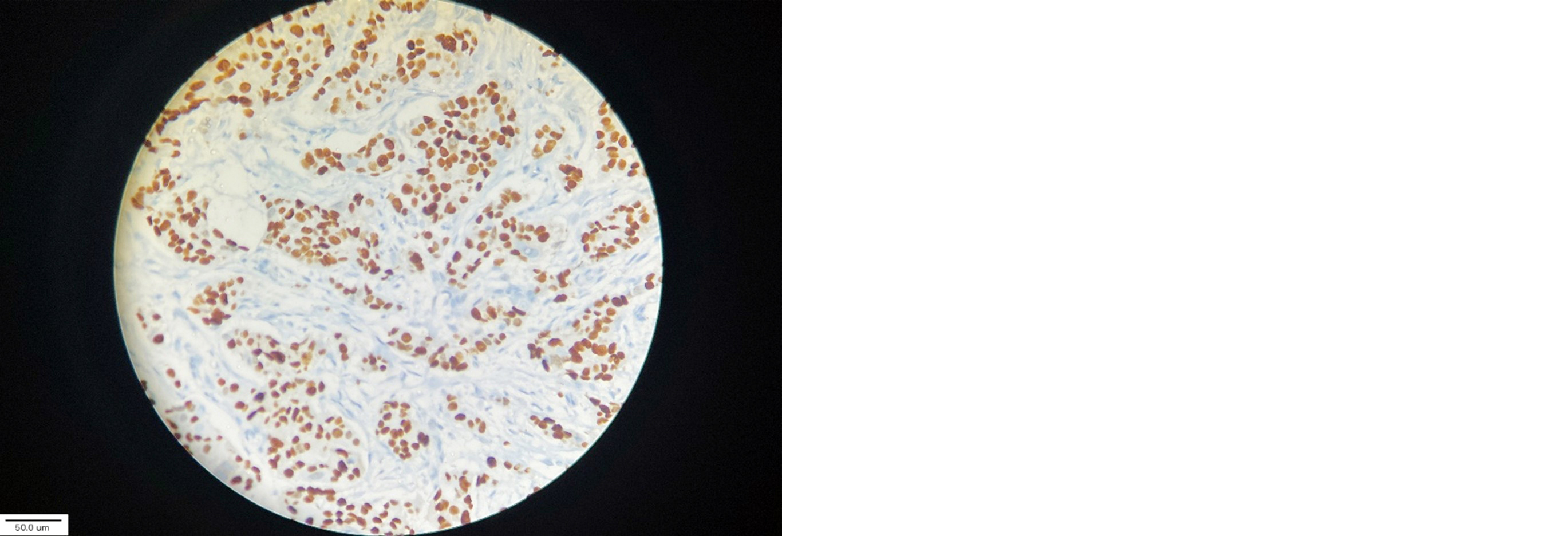
Figure 4: Immunohistochemical staining demonstrates nuclear positivity for progesterone receptor (PR) in tumor cells “x 40”.
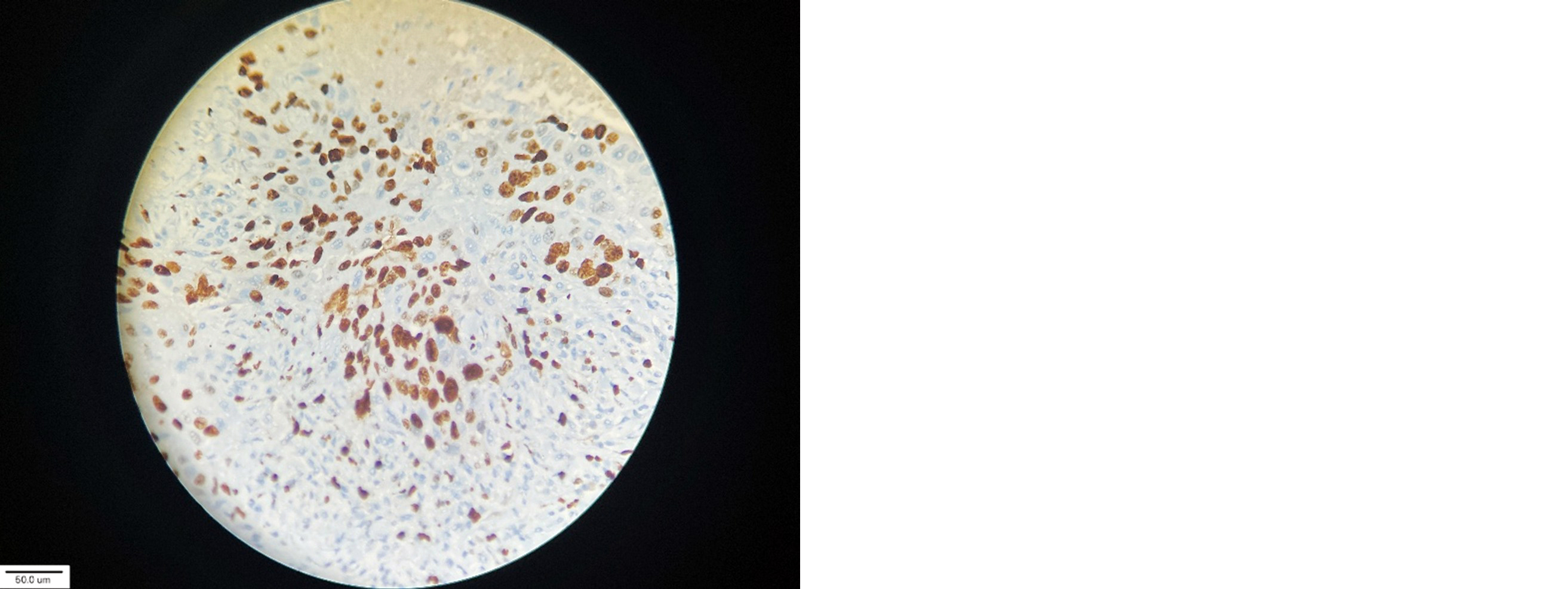
Figure 5: Ki-67 High index (>15%) 40X.
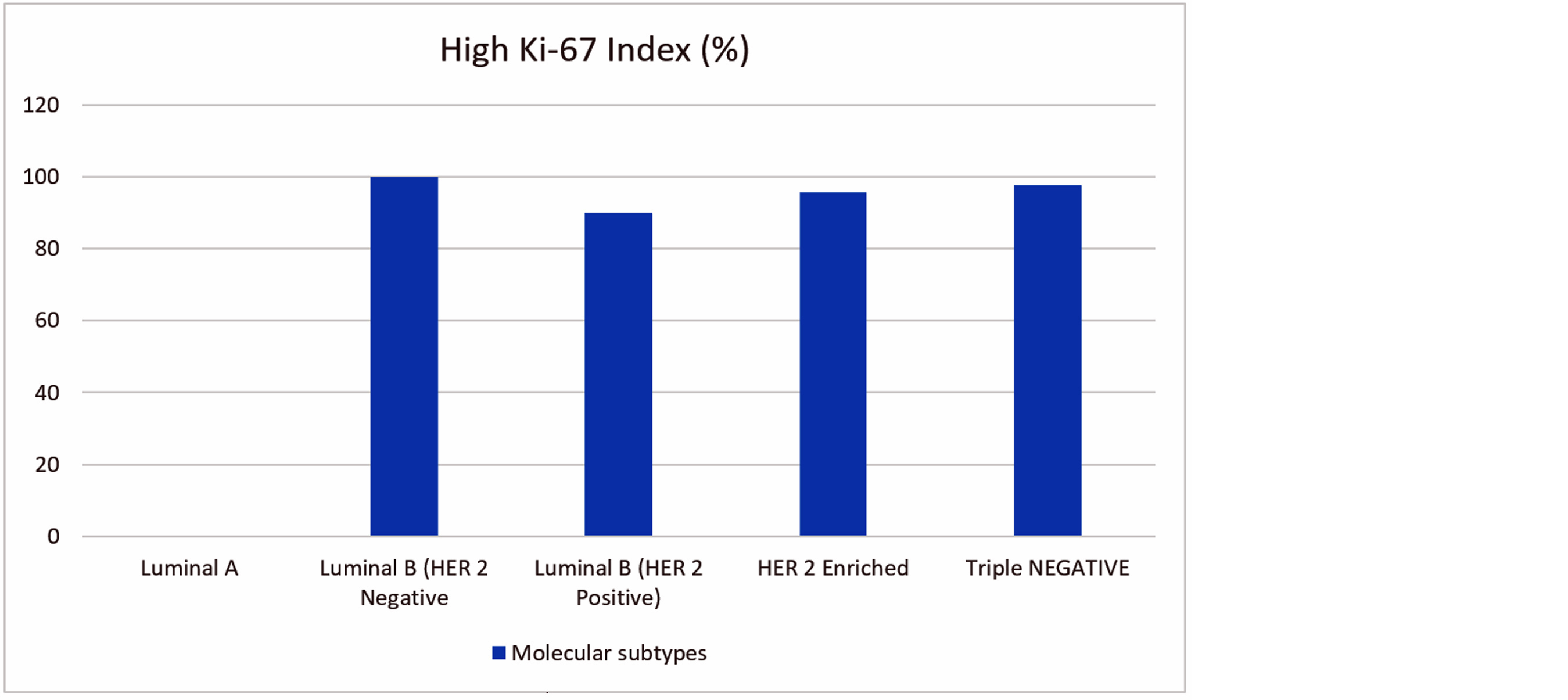
Figure 6: High Ki-67 index among the molecular subtypes.
The histological and immunohistochemical profile of the cohort showed that the vast majority of tumors were of no specific type (90.6%), with less common subtypes including mucinous carcinoma (3.8%), invasive lobular carcinoma (2.6%), and other rare histologies collectively comprising less than 5% of cases. Tumor grading revealed that over half of the tumors were moderately differentiated (Grade II, 53.6%), followed by high-grade (Grade III, 29.8%) and low-grade (Grade I, 16.6%) tumors. Hormone receptor analysis indicated that 69.4% of tumors were positive for both ER and PR, whereas 30.6% were negative. HER2 overexpression was observed in 23.8% of cases. Proliferative activity, assessed by Ki-67, was high in the majority of tumors, with 70.8% exhibiting expression above 15%, suggesting a predominance of biologically active tumors. Overall, these findings reflect a cohort largely characterized by conventional histology, moderate differentiation, hormone receptor positivity, and elevated proliferative potential, consistent with patterns observed in similar breast cancer populations.
The histological and immune histochemical characteristics of the study are summarized in Table 2.
Table 2: Histological and Immunohistochemical characteristics of the study.
|
Parameter
|
Number of patients (%)
|
|
Histological type
|
|
No specific type
|
453 (90.6%)
|
|
Mucinous carcinoma
|
19 (3.8%)
|
|
Invasive lobular carcinoma
|
13 (2.6%)
|
|
Invasive papillary carcinoma
|
7 (1.4%)
|
|
Invasive solid papillary carcinoma
|
5 (1%)
|
|
Invasive micro papillary carcinoma
|
2 (0.4%)
|
|
Tubular carcinoma
|
1 (0.2%)
|
|
Histological grade
|
|
Grade I
|
83 (16.6%)
|
|
Grade II
|
268 (53.6%)
|
|
Grade III
|
149 (29.8%)
|
|
Estrogen receptor status
|
|
|
Positive
|
347 (69.4%)
|
|
Negative
|
153 (30.6%)
|
|
Progesterone receptor status
|
|
Positive
|
347 (69.4%)
|
|
Negative
|
153 (30.6%)
|
|
HER 2 status
|
|
|
Positive
|
119 (23.8%)
|
|
Negative
|
381 (76.2)
|
|
Ki-67 expression
|
|
</= 15
|
146 (29.2%)
|
|
>15
|
354 (70.8%)
|
As per the ER, PR, HER 2 and Ki-67 status the tumors were classified into Luminal A, Luminal B [Luminal B (HER 2 positive) and luminal B (HER 2 negative)], HER 2 enriched and triple negative. Luminal A was observed in 136 patients (27.2%), luminal B (HER 2 positive) in 50 patients (10%), luminal B (HER 2 negative) in 161 patients (32.2%), HER 2 enriched in 69 patients (13.8%) and triple negative in 84 patients (16.8%) (Figure 7).
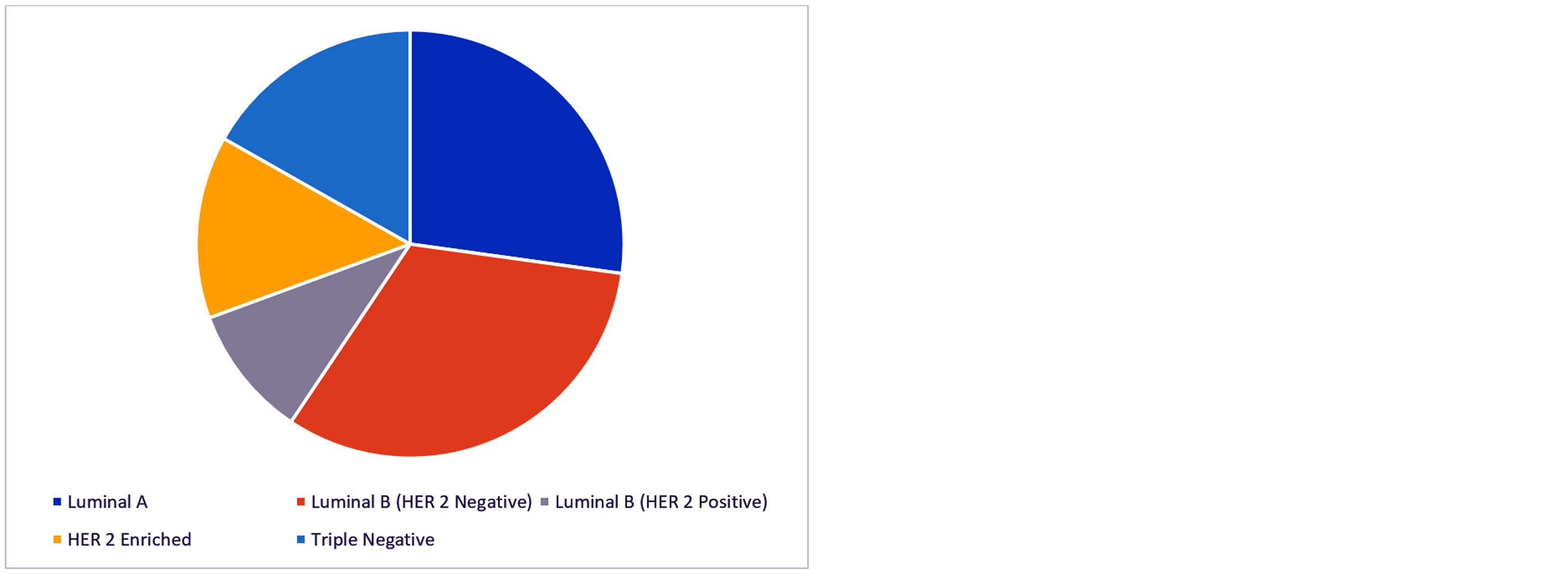
Figure 7: Molecular subtypes in breast carcinoma.
There was a significant association between molecular subtypes of invasive breast carcinoma with age and tumor grade (p < 0.05). The distribution of breast cancer subtypes varied significantly across age groups and tumor grades. Luminal A tumors were most common in patients aged 61–70 years (32.4%), whereas triple-negative tumors were predominantly observed in younger patients aged 31–40 years (20.2%), indicating a significant age-related pattern (p = 0.001). Luminal B (HER2 negative) and HER2-enriched subtypes were more evenly distributed across middle-aged groups (41–60 years), while luminal B (HER2 positive) cases peaked in the 41–50-year range (34%). Analysis of tumor grade revealed that Luminal A tumors were largely low-grade (Grade I, 45.6%) with no Grade III cases, while high-grade tumors (Grade III) were markedly more frequent among triple-negative (71.4%) and HER2-enriched (46.4%) subtypes. Luminal B subtypes demonstrated intermediate-grade predominance, with Grade II accounting for 67.7% in HER2 negative and 52% in HER2 positive tumors, reflecting a highly significant association between molecular subtype and tumor grade (p < 0.0001). These findings suggest that both patient age and tumor grade are closely associated with breast cancer molecular subtype, highlighting distinct clinical and pathological patterns. The correlation of clinicopathologic parameters with molecular subtypes in invasive breast carcinoma are summarized in Table 3.
Table 3: Clinicopathological parameters in correlation to molecular subtypes of the study.
|
Parameters
|
Luminal A
N (%)
|
Luminal B (HER 2 negative)
N (%)
|
Luminal B (HER 2 positive)
N (%)
|
HER 2 Enriched
N (%)
|
Triple negative
N (%)
|
p value
|
|
Age (Years)
|
|
(21-30)
|
0 (0)
|
4 (2.5)
|
1 (2)
|
1 (1.45)
|
1 (1.2)
|
|
|
(31-40)
|
8 (5.9)
|
13 (8.1)
|
5 (10)
|
3 (4.35)
|
17 (20.2)
|
0.001
|
|
(41-50)
|
18 (13.2)
|
38 (23.6)
|
17 (34)
|
17 (24.65)
|
21 (25)
|
|
|
(51-60)
|
36 (26.5)
|
56 (34.8)
|
10 (20)
|
25 (36.2)
|
23 (27.4)
|
|
|
(61-70)
|
44 (32.4)
|
31 (19.2)
|
13 (26)
|
17 (24.65)
|
13 (15.5)
|
|
|
(71-80)
|
24 (17.6)
|
15 (9.3)
|
4 (8)
|
5 (7.25)
|
8 (9.5)
|
|
|
(81-90)
|
6 (4.4)
|
4 (2.5)
|
0 (0)
|
1 (1.45)
|
1 (1.2)
|
|
|
Tumor grade
|
|
I
|
62 (45.6)
|
16 (9.9)
|
3 (6)
|
1 (1.4)
|
1 (1.2)
|
|
|
II
|
74 (54.4)
|
109 (67.7)
|
26 (52)
|
36 (52.2)
|
23 (27.4)
|
< 0.0001
|
|
III
|
0 (0)
|
36 (22.4)
|
21 (42)
|
32 (46.4)
|
60 (71.4)
|
|
Discussion
This cohort study conducted in Telangana, South India, evaluated clinicopathological parameters across molecular subtypes of invasive breast carcinoma. A total of 500 cases were included, with a mean patient age of 56.45 years (range: 25–89 years), consistent with findings from a study in North India (mean age 54.4 years) and a study in South India (mean age 54 years) [2, 14]. However, the mean age in the present study was higher than the study done by Jagadeesan GM [4].
This study showed predominant histologic subtype of breast cancer was invasive breast carcinoma of no specific type (90.6 %), similar to a study done in a tertiary center in South India (invasive breast carcinoma of no specific type 94%) and other Indian studies [10, 14].
This study showed that invasive breast carcinoma cases were ER positive in 347 patients (69.4%) and PR positive in 347 patients (69.4%), similar to a study done in a tertiary cancer center in North India [2], ER positivity is similar to another study done in South India [14] and PR positivity is similar to another study done by Onitilo A et.al [15].
Luminal B was the most common molecular subtype, similar to findings from SCB Medical College and Hospital, Cuttack [8], whereas other studies, such as that by Jagadeesan GM reported luminal A as the predominant subtype [4]. In some populations, such as Togolese women, triple-negative tumors were the most frequent, followed by luminal A [9]. In the present study, after luminal B, luminal A was the second most common subtype, followed by triple-negative and HER2-enriched tumors.
Tumor grade analysis revealed that Grade II tumors were most common (53.6%), followed by Grade III (29.8%), reflecting a substantial proportion of aggressive tumors in this population [4, 14].
Molecular characterization showed that luminal A tumors were ER- and PR-positive, HER2-negative, and had a low Ki-67 index (<15%), corresponding to lower histological grade and favorable prognosis. In contrast, triple-negative and HER2-enriched tumors displayed higher histological grades, indicating poorer prognosis [11]. Hormone receptors were positive in 69.4% of patients, while HER2 positivity was observed in 23.8% of cases, consistent with Sofi et al. in Kashmir [10] and slightly higher than reported by Jagadeesan GM [4].
A high Ki-67 index (>15%) was observed in 70.8% of patients, highlighting the proliferative nature of tumors in this South Indian cohort and their association with aggressive behaviour and poorer prognosis. This finding aligns with other studies in India [11-13, 15].
Conclusion
This study shows high Ki-67 index with higher histological tumor grade and hormones receptors positive in more than half of the patients which results in poor prognosis which indicates the necessity to create awareness about breast cancer and introduce early diagnosis methods and access to molecular subtyping and targeted therapies.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, et al. GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024; 74:229–263.
[2] Jain S, Narang V, Jain K, Paul D, Singh J, et al. Prevalence of molecular subtypes in operated cases of breast cancer and its clinicopathological correlation: A single institute study from a tertiary cancer centre in North India. Indian J Surg Oncol. 2021; 12:538–544.
[3] Sharma JD, Khanna S, Ramchandani S, Kakoti LM, Baruah A, et al. Prevalence of molecular subtypes of breast carcinoma and its comparison between two different age groups: A retrospective study from a tertiary care center of Northeast India. South Asian J Cancer. 2021; 10:220–224.
[4] Jagadeesan GM. The association between molecular subtypes of breast cancer and its clinical and histopathological prognostic factors in Southern India population. Int J Med Pharm Res. 2025; 6:10–17.
[5] Shim HJ, Kim SH, Kang BJ, Choi BG, Kim HS, et al. Breast cancer recurrence according to molecular subtype. Asian Pac J Cancer Prev. 2014; 15:5539–5544.
[6] Lakshmaiah KC, Das U, Suresh TM, Lokanatha D, Babu GK, et al. A study of triple negative breast cancer at a tertiary cancer care center in Southern India. Ann Med Health Sci Res. 2014; 4:933–937.
[7] Sanmathi SB, Narayanan GS, Amogh PS, Kumar BR. Breast cancer in young women: Analysis of incidence, clinicopathological profile and biological behaviour in a tertiary care institute from South India. Asian Pac J Cancer Biol. 2024; 9:295–300.
[8] Shanker Ramchandwani D, Dash M, Panda D, Sahoo SS. Molecular and histopathological correlation of breast cancer subtypes with prognostic markers in Eastern India: A study from a tertiary care center. Eur J Cardiovasc Med. 2025; 15: 77– 81.
[9] Ablavi Adani–Ife, Amegbor K, Doh K, Darre T. Breast cancer in Togolese women: Immunohistochemistry subtypes. BMC Womens Health. 2020; 20:261.
[10] Mir MA, Manzoor F, Singh B, Raja W, Jeelani S, et al. Clinicopathological profile of breast cancer patients at a tertiary care hospital in Kashmir Valley. Surg Sci. 2017; 8:301–308.
[11] Mane A, Khatib KI, Deshmukh SP, Nag SM, Sane SP, et al. A comparison of clinical features, pathology and outcomes in various subtypes of breast cancer in Indian women. J Clin Diagn Res. 2015; 9:1–4.
[12] Louis DM, Mathew M, Gutjahr G, Vijayakumar DK, Pavithran K, et al. Survival outcomes of breast cancer patients in South India over 20 years. Asian Pac J Cancer Prev. 2024; 25:2633–2644.
[13] Devadass CW, Royal AB, Saxena P, Devraj D, Gouri M. Breast carcinoma: Correlation of molecular subtypes with histopathologic characteristics. J Med Sci. 2023; 9:281.
[14] Nawaz PN, Sebastian N, Raja T, Ramya A, Kumanan J, et al. Molecular classification of breast cancer using IHC markers: Experience from a tertiary cancer center in South India. Int J Res Med Sci. 2023; 11: 3729–3733.
[15] Onitilo A, Engel J, Greenlee R, Mukesh B. Breast cancer subtypes based on ER/PR and Her2 expression: Comparison of clinicopathologic features and survival. Clin Med Res. 2009; 7:4–13.