Full Text
Introduction
Aggressive fibromatosis of the cervical region, although histologically benign, is characterized by local invasiveness and a high recurrence rate. Surgical excision is the primary treatment; however, recurrent disease often results in fibrosis, scarring, and anatomical distortion. These sequelae pose significant challenges in anaesthetic management, particularly airway control, where anatomical unpredictability can elevate perioperative risk.
We present a case of recurrent cervical fibromatosis in a young male with complex airway anatomy, managed successfully with awake fibreoptic intubation in the sitting position. This case demonstrates the significance of meticulous preoperative planning, interdisciplinary coordination, and tailored anaesthetic strategies in managing difficult airways [1].
Case presentation
A 20-year-old male presented with a 10 × 10 cm ulcerated, firm, immobile mass over the nape of the neck, extending to the right shoulder. The patient had recurrent fibromatosis since 2015 and had undergone multiple resections, radiotherapy, and chemotherapy. No other significant comorbidities were present. Prior anaesthetic records were unavailable.
The patient was alert, oriented, and cooperative. Airway examination revealed a mouth opening of 2.5 fingerbreadths, mild buck teeth, a long left upper incisor, and a missing right upper incisor. Neck extension was negligible with minimal flexion. The patient was unable to tolerate a supine position due to tumour compression. These findings indicated a high-risk difficult airway.
MRI revealed a heterogeneous soft tissue mass (10.2 × 13.4 × 14.6 cm) involving subcutaneous, muscular, and intermuscular planes from the occiput to C6 spinous processes (Figure 1). Significant anatomical distortion of posterior cervical spaces was noted, without airway lumen compromise.

Figure 1: Pre-operative assessment of airway, (a) the size of the neck mass severely restricted neck movement (b) adequate mouth opening was present.
Airway management
Given the inability to lie supine, restricted neck movement, and distorted anatomy, the airway was categorized as high-risk (ASA Difficult Airway Algorithm Category IV) [1,2]. Awake fibreoptic intubation in the sitting position was chosen as the primary strategy (Figure 2).
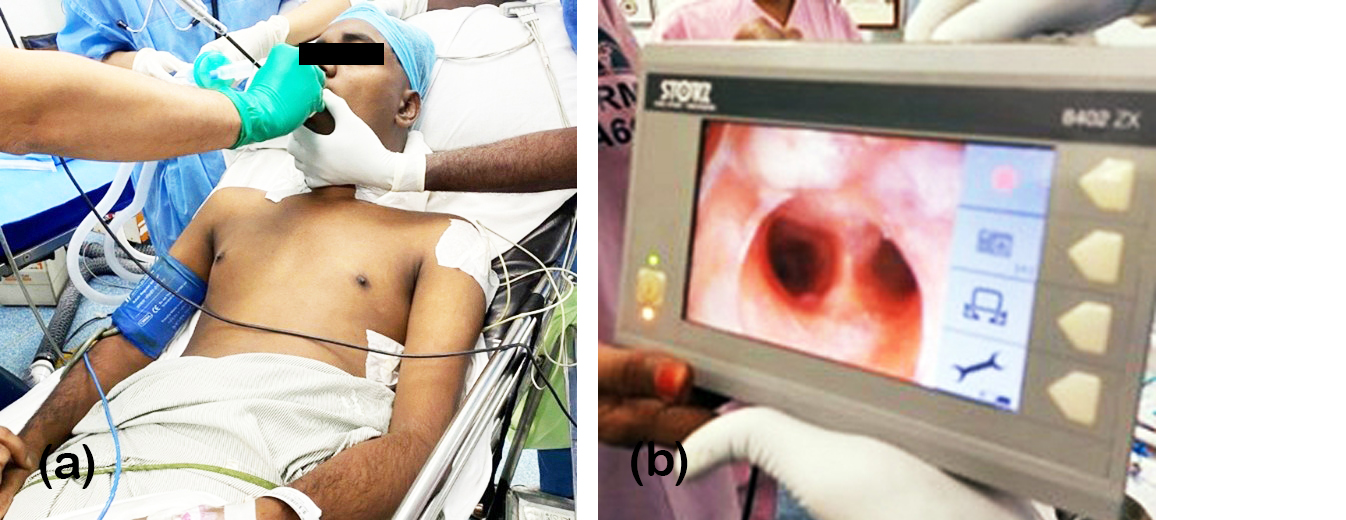
Figure 2: Awake fibreoptic intubation in sitting position. (a) the patient is placed in fowler’s position and the operator is in front of the patient, introducing the fiberoptic scope through the oral airway. (b) fiberoptic view of carina is shown as obtained.
Preoperative preparation included intravenous glycopyrrolate 0.2 mg and dexamethasone 8 mg. Sedation was achieved with dexmedetomidine (1 μg/kg loading over 10 minutes, then 0.5 μg/kg/min infusion) [5].
The airway was meticulously prepared using a multimodal topical anaesthesia approach to ensure optimal patient comfort and suppress airway reflexes during awake fibreoptic intubation. This included pre-procedure nebulization with 4% lignocaine to achieve widespread mucosal anaesthesia of the upper and lower airways, followed by the placement of nasal pledgets soaked in 2% lignocaine combined with adrenaline to provide local anaesthesia while minimizing mucosal bleeding. Additional 10% lignocaine oropharyngeal spray was administered to anesthetize the tongue, oropharynx, and posterior pharyngeal wall, thereby reducing gag and cough reflexes. During bronchoscope advancement, the “spray-as-you-go” technique with 2% lignocaine was employed to provide targeted anaesthesia of deeper airway structures, ensuring a smooth and well-tolerated intubation process [3].
The total lignocaine dose was ~300 mg (20 ml), within the safe limit for a 70 kg patient. A preloaded 8.0 mm flexometallic endotracheal tube was introduced orally via a modified bite block. Fibreoptic advancement to the carina allowed successful intubation, confirmed by end-tidal CO₂.
Surgical procedure
The patient was placed prone with bolsters and pressure padding. Wide local excision of the cervical mass was performed, followed by bilateral latissimus dorsi flap reconstruction. Intraoperative monitoring included invasive arterial pressure, three intravenous lines, urine output, and arterial blood gas (ABG)-guided fluid therapy. Anaesthesia was maintained with fentanyl (2 μg/kg), propofol (2 mg/kg), vecuronium (0.1 mg/kg), and sevoflurane (MAC 0.8–1.0) in air–oxygen (FiO₂ 40%).
Follow-up and outcomes
Postoperatively, the patient remained intubated and prone in the ICU for 48 hours. Extubation on postoperative day (POD) 2 was uneventful. Mobilization began on POD 10, and recovery proceeded without respiratory or surgical complications.
Discussion
This case underscores the complexities of airway management in patients with large posterior cervical masses. Repeated surgeries, radiotherapy, and tumour recurrence contribute to scarring and distortion, making conventional laryngoscopy hazardous.
Rationale for awake fibreoptic intubation in sitting position: The anatomical limitations—fixed neck, posterior mass displacement, and supine intolerance—necessitated an approach that preserved spontaneous breathing, maintained airway patency, and allowed optimal visualization [1,2]. The sitting position improved visualization, aided gravity-assisted airway clearance, and reduced the risk of airway collapse.
Topicalization and sedation: Graded airway topicalization, as recommended by Yasuda et al. [3] and Lee et al. [4], effectively blunted gag and cough reflexes. Dexmedetomidine was selected for its anxiolytic, sedative, and analgesic effects without respiratory depression, aligning with Abdelmalak et al.’s findings [5].
Physiological and safety considerations: Maintaining spontaneous ventilation is a central principle in anticipated difficult airway scenarios. Loss of spontaneous breathing after induction in such cases may precipitate a “cannot ventilate, cannot intubate” crisis, particularly when surgical airway access is anatomically compromised [6,7]. By avoiding neuromuscular blockade until the airway was secured, we reduced the risk of dynamic airway collapse and hypoxia. Additionally, the upright position improved functional residual capacity and oxygenation, which is particularly advantageous in prolonged intubation attempts [8].
Sedation strategy and team coordination: Dexmedetomidine, compared with other sedatives such as midazolam or propofol, offers superior hemodynamic stability and allows easy arousability, which is beneficial when patient cooperation is needed for AFOI [5,9]. Furthermore, comprehensive planning—including backup strategies such as emergency surgical airway preparation—was critical to safety. Simulation-based team rehearsals and clear communication among anaesthesia, surgical, and nursing staff have been shown to improve outcomes in anticipated difficult airways [10, 11]. Our approach adhered closely to current international guidelines, such as those from the Difficult Airway Society, which emphasize patient positioning, sedation titration, and the preservation of spontaneous breathing until the airway is secured [12].
Alternative techniques: Options such as video laryngoscopy, supraglottic device-guided intubation, or tracheostomy were considered but posed higher risks of failure, trauma, or surgical delay. The chosen approach—oral AFOI in the sitting position—provided the most controlled, safest, and patient-centered outcome in this setting [1, 2].
Conclusion
Awake fibreoptic intubation in the sitting position offers a safe and effective airway strategy for patients with massive cervical tumours and positional limitations. This approach facilitates spontaneous ventilation, improves visualization, and minimizes the risk of airway collapse. Success depends on early airway risk recognition, multidisciplinary coordination, stepwise topicalization, and cooperative sedation.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Saxena KN, Dua CK, Chalam KS. Awake fibreoptic intubation in a patient with a huge thyroid swelling. Indian J Anaesth. 2011; 55:154–157.
[2] Kumar A, Sinha C, Kumar A. Awake fibreoptic intubation in a sitting position: airway management in a case of anticipated difficult airway. J Anaesthesiol Clin Pharmacol. 2018; 34:286–288.
[3] Yasuda Y, Ueki R, Tanioka S, Yamanaka K, Ouchi T, et al. Management of anesthetic airway in juvenile hyaline fibromatosis. JA Clin Rep. 2021; 7:1–4.
[4] Lee H, Baek SJ, Kim DW, Kim JH. Fibreoptic intubation via laryngeal mask airway in patients with cervical spine fixation. Korean J Anesthesiol. 2012; 62:92–95.
[5] Abdelmalak B, Makary L, Hoban JD, Doyle DJ. Dexmedetomidine for awake fiberoptic intubation in the patient with a compromised airway: a review. Anesth Analg. 2007; 105:1265–1272.
[6] Collins SR, Blank RS. Fiberoptic intubation: an overview and update. Respir Care. 2014; 59:865–878.
[7] Cook TM, Woodall N, Frerk C. Fourth National Audit Project. Major complications of airway management in the UK. Br J Anaesth. 2011; 106:617–631.
[8] Bhavani–Shankar K, Kumar AY, Moseley H, Delph Y. Oxygenation and ventilation during awake fiberoptic intubation in different positions. Anesth Analg. 2000; 91:780–782.
[9] Tsai CJ, Chu KS, Chen TI, Lu DV, Wang HM, et al. A comparison of dexmedetomidine versus propofol target–controlled infusion for sedation during fiberoptic intubation. Anaesthesia. 2010; 65:930–935.
[10] Chrimes N, Higgs A. Planning for airway management in resource–limited settings. Anaesthesia. 2019; 74:69–83.
[11] Greenland KB, Acott C, Segal R, Goulding G, Riley RH. Emergency surgical airway in life–threatening airway obstruction: a structured approach to decision making. Anaesth Intensive Care. 2011; 39:761–769.
[12] Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015; 115:827–848.