Full Text
Introduction
Deep Neck Space Infections (DNSIs) are serious and potentially life-threatening conditions involving the deep fascial compartments of the neck [1]. They commonly originate from odontogenic sources, tonsillitis, or upper respiratory tract infections [2]. Among these, odontogenic infections particularly those associated with lower third molars represent a significant cause because of the close anatomical relationship between mandibular molar roots and the submandibular and parapharyngeal spaces [3]. The neck is anatomically divided into several potential spaces by the deep cervical fascia. These spaces are vulnerable to infection when breached by odontogenic, oropharyngeal, or salivary gland sources [4]. The parapharyngeal space is one of the most frequently affected compartments and is commonly involved in infections spreading from the tonsils, teeth, or parotid gland. Retropharyngeal space infections are more prevalent in children and arise from suppuration of retropharyngeal lymph nodes. They may also develop secondary to upper respiratory tract infections or trauma [5].
The danger space lies posterior to the retropharyngeal space and extends from the skull base to the diaphragm. Although it is rarely primarily infected, it is clinically significant due to its ability to rapidly transmit infection into the mediastinum, resulting in descending mediastinitis [6].
The submandibular space, including the sublingual and submental compartments, is particularly susceptible to odontogenic infections involving the lower molars. It is classically associated with Ludwig’s angina, a rapidly progressive cellulitis that can lead to airway obstruction [7]. The masticator space, which includes the muscles of mastication and the mandibular ramus, is commonly secondarily involved through dental sources and typically presents with trismus and facial swelling [8].
The parotid space is less frequently involved but may be affected in cases of sialadenitis or parotitis, occasionally presenting with facial nerve weakness [9]. Rarely, infection of the prevertebral space may occur secondary to tuberculous spondylitis or vertebral osteomyelitis, resulting in neck rigidity and neurological deficits.
Although the incidence of DNSIs has declined in the antibiotic era, they continue to be associated with significant morbidity and mortality, particularly when diagnosis or treatment is delayed. In adults, the parapharyngeal and submandibular spaces are most commonly affected, whereas retropharyngeal infections predominate in pediatric patients [10].
This case report describes a diabetic male who developed extensive parapharyngeal and submandibular abscesses following mandibular third molar extraction, presenting with dysphagia and trismus.
Case report
A 41-year-old male, known to have diabetes mellitus, presented with a five-day history of progressively worsening swelling over the left side of the jaw, which began shortly after the extraction of the left mandibular third molar. The extraction was performed by a dentist, who did not prescribe any postoperative antibiotics. The swelling was insidious in onset and gradually increased in size. The patient complained of trismus, odynophagia, and difficulty swallowing, but denied any initial fever or respiratory distress. Five days post-extraction, due to worsening symptoms, he revisited the same dentist and was prescribed oral Augmentin 625 mg twice daily.
As his symptoms continued to progress, he sought care at a local ENT clinic, where he received a single dose of intravenous Zostum 1.5 g stat. Due to persistent and non-resolving symptoms, the patient subsequently presented to a tertiary care hospital.
On clinical examination, there was a tender, diffuse swelling over the left submandibular and parapharyngeal regions, with markedly restricted mouth opening and palpable cervical lymphadenopathy on the left side. Oropharyngeal examination was limited due to trismus but revealed bulging of the left lateral pharyngeal wall. Ultrasonography demonstrated a collection within the left masseter space extending into the masticator space, suggestive of abscess formation. Contrast-enhanced CT of the neck revealed an ill-defined collection with peripheral enhancement extending from the submandibular to the parapharyngeal and retropharyngeal spaces, consistent with a deep neck space abscess (Figure 1). Associated left cervical lymphadenopathy was also noted.
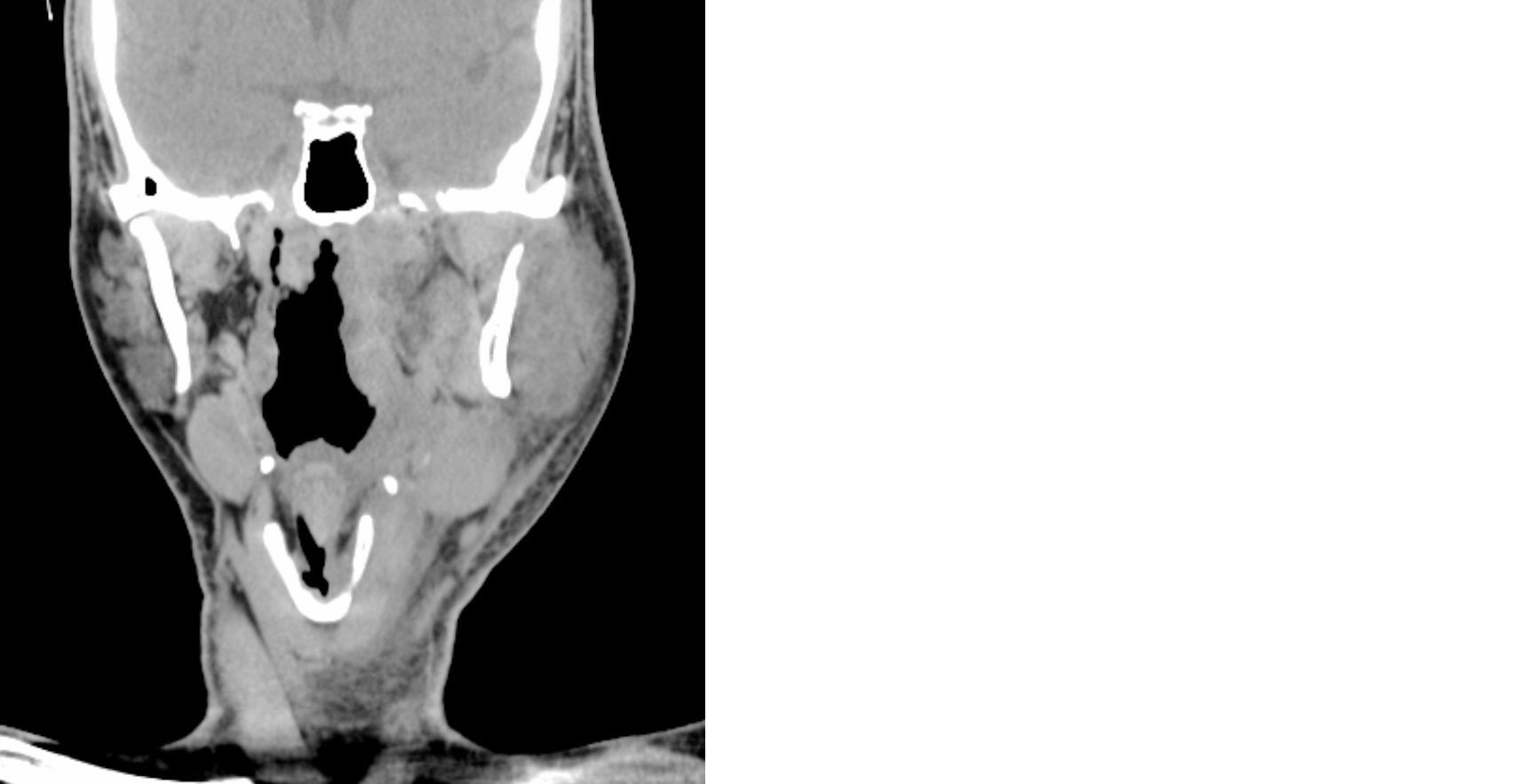
Figure 1: CT neck plain (Coronal view) showing Ill-defined collection extending from submandibular to parapharyngeal spaces.
On the second day of admission, ultrasound-guided aspiration of the left neck space abscess was performed by the interventional radiology team, yielding approximately 8 ml of purulent material. The sample was sent for Gram stain, fungal stain and acid-fast bacilli (AFB) testing, all of which returned negative results.
Due to persistent symptoms and ongoing radiological evidence of deep neck space infection, the patient was taken for open surgical drainage (incision and drainage) via a transcervical approach (Figure 2). Thick purulent material was evacuated and the wound was left open for dependent drainage.

Figure 2: Image showing neck incision for Surgical drainage of abscess by transcervical approach.
Blood investigations revealed elevated C-Reactive Protein (CRP) levels and an increased White Blood Cell (WBC) count. Postoperatively, the patient developed worsening dysphagia and a coughing/choking sensation while attempting to drink liquids or eat solid food. A Ryle’s tube was inserted for enteral feeding. Flexible laryngoscopy demonstrated pooling of secretions in the bilateral pyriform fossae and mildly reduced mobility of the left vocal cord.
A follow-up contrast-enhanced CT scan of the neck and chest revealed persistent collections within the deep neck spaces, including the retropharyngeal and danger spaces, with extension into the mediastinum and partial reduction of the masticator space component (Figure 3). Narrowing of the left internal jugular vein was also noted.
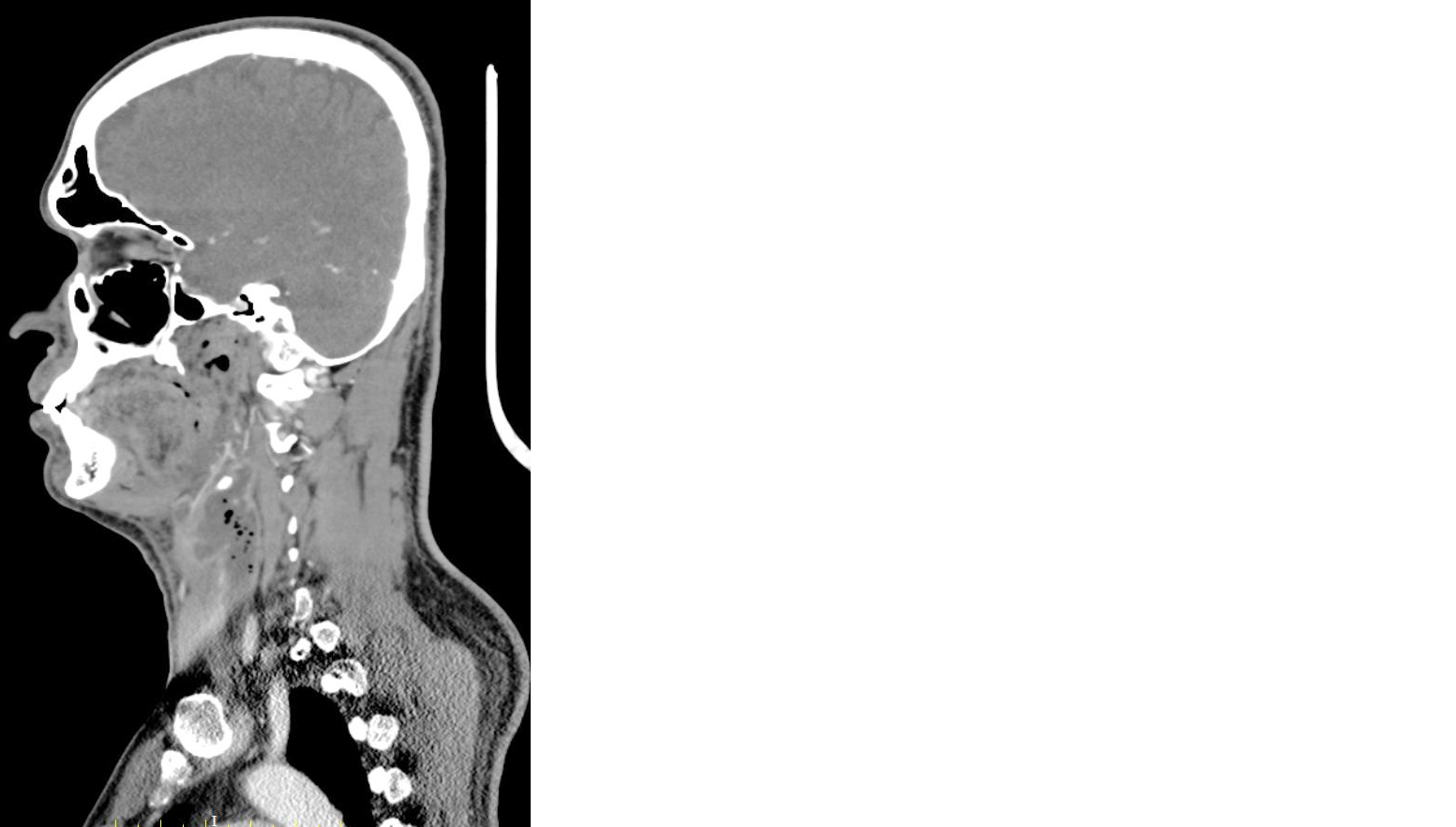
Figure 3: CT neck (sagittal view) showing neck abscess extending into retropharyngeal, danger space and mediastinal space with reduction in masticator space component.
As the symptoms continued to persist, an Upper Gastrointestinal Endoscopy (UGIE) was performed, which revealed only mild erosive gastritis. A Neurologist’s opinion was sought in view of suspected neurological dysphagia. MRI of the neck was advised and subsequently performed, demonstrating a collection along the left medial pterygoid muscle with extension into multiple adjacent deep neck spaces, causing compression of the esophagus and involvement of the left alveolar margin.
Since trismus remained unresolved even on postoperative day 7 (POD-7), a repeat contrast-enhanced CT scan of the neck and chest was obtained. It revealed persistent retropharyngeal and mediastinal extension of the abscess. The patient was advised to continue Ryle’s tube feeding and perform incentive spirometry for pulmonary support.
As the patient gradually improved symptomatically, with normalization of the WBC count, he was discharged with the Nasogastric Tube (NGT) in situ, along with instructions to continue intravenous antibiotics at home and attend regular follow-up in the outpatient department.
Discussion
Deep Neck Space Infections (DNSIs) remain a critical concern in otorhinolaryngology due to their rapid progression and close proximity to vital neurovascular structures and the airway [1]. Although third molar extraction is among the most common minor oral surgical procedures, this case highlights a rare yet serious complication of post-extraction deep neck infection [6].
Odontogenic infections account for up to 70% of DNSIs, most commonly arising from lower molars due to their close anatomical relationship with the submandibular, masticator, and parapharyngeal spaces [3]. In the present case, the infection likely originated from the extraction socket and subsequently spread into deeper cervical fascial compartments. The parapharyngeal space, bordered medially by the pharynx and laterally by the carotid sheath, serves as a conduit for infection to extend superiorly toward the skull base or inferiorly into the mediastinum via the danger space [5]. This potential for rapid dissemination emphasizes the need for early recognition and aggressive management [7].
Clinical features such as trismus, dysphagia, odynophagia, fever, and neck swelling following dental procedures should raise suspicion for deep neck space involvement [8]. Contrast-enhanced computed tomography remains the imaging modality of choice, as it accurately delineates the extent of infection, identifies abscess formation, and guides surgical planning [4].
DNSIs are typically polymicrobial, involving both aerobic and anaerobic organisms. In diabetic patients, gram-negative pathogens are more prevalent, particularly Klebsiella pneumoniae (25–40%), followed by Streptococcus species (~20%) and anaerobes (20–25%) [11]. In contrast, non-diabetic individuals more commonly demonstrate Streptococcus viridans(40–50%), Staphylococcus aureus (15–20%), and anaerobes such as Peptostreptococcus, Prevotella, and Fusobacterium(20–30%) [3]. The predominance of Klebsiella pneumoniae in diabetic patients is clinically significant, as it is associated with more severe disease, rapid spread, and higher complication rates [11].
Effective management requires a multidisciplinary approach involving otorhinolaryngologists, maxillofacial surgeons, and cardiothoracic surgeons when mediastinal extension is suspected. Prompt initiation of broad-spectrum intravenous antibiotics and timely surgical drainage remain the cornerstone of treatment [12]. Airway assessment is crucial, particularly in infections involving the submandibular or parapharyngeal spaces, due to the risk of airway compromise.
This case underscores the importance of strict postoperative infection surveillance following dental procedures, especially in high-risk individuals such as diabetic and immunocompromised patients. Furthermore, persistent or worsening symptoms despite antibiotic therapy should prompt urgent contrast-enhanced CT imaging to prevent potentially fatal complications [4,13].
Conclusion
Deep Neck Space Infections, although uncommon in the modern antibiotic era, may develop as serious complications following routine dental procedures such as third molar extraction. Early recognition, prompt diagnostic imaging, aggressive antimicrobial therapy and timely surgical drainage are essential to preventing potentially life-threatening consequences including airway obstruction and descending mediastinitis. This case emphasizes the importance of diligent postoperative monitoring, particularly in high-risk populations such as patients with diabetes. It also underscores the need for coordinated multidisciplinary management involving dental surgeons, otorhinolaryngologists, radiologists and critical care teams to ensure optimal outcomes. Patient education regarding early warning symptoms and the importance of timely follow-up plays a crucial role in reducing morbidity and avoiding preventable complications.
Conflicts of Interest
Authors declare no conflict of interest.
References
[1] Wang LF, Chen YH, Huang CC, Tsai YT, Wu HP. Deep Neck Infections: updated insights on etiology and treatment. J Otolaryngol. 2023; 52:113–120.
[2] Marioni G, Marchese–Ragona R, Nardo C, Staffieri C, Staffieri A. Deep neck infections: evolving trends and future directions. Head Neck. 2019; 41:1120–1127.
[3] Mortimore S, Clarke P, Hughes R, Adams J, Williams M. Odontogenic causes of deep neck infections: clinical implications and surgical outcomes. Br Dent J. 2018; 224:195–199.
[4] Lim JY, Kim DH, Ahn SH, Park HJ, Kim J. Anatomic spread of deep neck space infections and the role of CT imaging. Radiographics. 2017; 37:94–108.
[5] Sethi DS. Pediatric retropharyngeal abscess: changing patterns and management strategies. Pediatr Otolaryngol J. 2015; 10:119–126.
[6] Cunha BA. The danger space and mediastinitis: a critical zone in deep neck infections. Clin Infect Dis. 2014; 58:547–550.
[7] Ali MJ, Naik MN, Honavar SG, Sheth H, Vazirani U. Ludwig’s angina: pathophysiology, presentation, and management. J Craniomaxillofac Surg. 2013; 41:1–5.
[8] Yeh LR, Chang YC, Hsu CY, Lin FH, Chen YT. Masticator space infection secondary to molar extraction. Dent Clin North Am. 2012; 56:381–392.
[9] Healy CM, Moran H, Cunningham M, McCarthy C, O’Connor R. Deep parotid space infections and facial nerve involvement. J Maxillofac Surg. 2011; 39:342–347.
[10] Chang TY, Huang CW, Lee YT, Cheng YH, Wang CY. Prevalence and outcomes of parapharyngeal and retropharyngeal space infections. J Oral Maxillofac Surg. 2021; 79:1034.e1–1034.e7.
[11] Kwon SY, Park JH, Lee SH, Kim YJ, Choi JH. Descending necrotizing mediastinitis from odontogenic infections: a clinical study and review. Korean J Otorhinolaryngol. 2022; 65:41–48.
[12] Singh R, Gupta S, Mehta K, Rao A, Thomas R. Retropharyngeal abscess in adults: an emerging challenge. ENT J. 2020; 99:512–516.
[13] Kass J, Anderson P, Lewis R, Kumar S, Patel K. Parapharyngeal infections: clinical features and management algorithm. Otolaryngol Clin North Am. 2016; 49:81–89.