Full Text
Introduction
Thyroid neoplasm is the most prevalent endocrine cancer, with a dramatically increased incidence, and the follicular epithelial cells account for more than 90% of all thyroid carcinomas [1, 2]. It often manifests as an asymptomatic neck tumour, while occasionally, it might cause local discomfort.
The most frequent primary malignant thyroid tumour is papillary thyroid carcinoma [3]. Microscopically, it can be identified by searching for the papillary pattern, which can have any variant pattern and, most significantly, its traditional nuclear features [4, 5]. The nuclear characteristics comprise nuclear enlargement, overlapping, crowding, or elongation; nuclear membrane abnormalities, grooves or pseudo inclusions; glassy nuclei or clear chromatin with margination, etc. Since non-neoplastic lesions like papillary thyroid hyperplasia and follicular lesions exhibiting papillary patterns with focal nuclear characteristics similar to PTC pose diagnosis challenges, it is not always easy to distinguish them. Due to the inter- and intra-observer variability caused by overlapping histomorphology patterns, auxiliary approaches must be used for the final, conclusive diagnosis. The use of IHC biomarkers may greatly aid its classification and diagnosis [6, 7]. Numerous researchers have looked into various immunohistochemistry markers in this context thus far. One such marker employed in this investigation is trophoblastic antigen 2. It was initially found in trophoblast cells and had a role during placental implantation. The tacsdt two gene on chromosome 1p32 encodes the transmembrane receptor glycoprotein Trop-2 [8]. It comprises an intracellular cytoplasmic tail, a transmembrane domain, and an extracellular domain. Trop-2 controls stem cell-like characteristics in addition to cell development, transformation, regeneration, and proliferation [9]. Its overexpression in several epithelial malignancies is associated with tumour aggressiveness and a poor prognosis [10, 11]. According to the limited research done thus far, Trop-2 expression displays a higher sensitivity and specificity for detecting PTC than other well-established markers widely used in clinical practice, such as cytokeratin 19, HBME1, and galectin 3. Numerous independent groups have identified Trop-2 as a novel papillary thyroid cancer immunohistochemistry marker with great sensitivity and specificity. Furthermore, Hongyu et al. demonstrated that MAPK-ERK/JNK/AP1/MMP2 signaling facilitates thyroid cancer cells' invasion and migration when Trop-2 is overexpressed [11]. The BRAF mutation, the most frequent genetic change in papillary thyroid cancer, is correlated by Kong et al. with Trop-2 overexpression. The team also concluded that Trop-2 expression is related to BRAF mutations, and its immunochemistry investigation can predict BRAF mutations in addition to other ways to diagnose PTC [12].
The current study evaluated the variable expression of Trop-2 in benign and malignant thyroid lesions. We contrasted PTC with other thyroid carcinomas in terms of its expression. Comparing Trop-2 expression in PTC with other thyroid carcinomas shed light on its specificity and relevance in distinguishing different thyroid cancer subtypes. This evaluation provided valuable insights into the role of Trop-2 in thyroid lesions and its potential as a diagnostic marker for PTC.
This study aimed to analyze the expression of Trop-2 in various thyroid lesions and its potential role in distinguishing papillary thyroid cancer from other thyroid tumors.
Materials and methods
Data for the present study was obtained from the specimens with macroscopically and microscopically visible malignant lesions, such as those from thyroid operations, e.g., lobectomy, isthmectomy, hemithyroidectomy, subtotal, near total, and total thyroidectomy received in the Department of Pathology, Mysore Medical College and Research Institute during the period from August 2022 to March 2024 (18 months). The clinical details were collected from the subject’s file, patients with clinically and screen-detected suspicious palpable thyroid carcinomas from K.R. Hospital and subsequently confirmed by histopathological diagnosis from the basis of the study. The study has been approved by the institutional ethical committee.
The inclusion criteria encompass all isthmectomy, hemithyroidectomy, subtotal thyroidectomy, and total or near-total thyroidectomy specimens, irrespective of age, in the Department of Pathology, MMCRI. The exclusion criteria include all thyroid specimens with metastatic deposits.
Methodology
The specimens were fetched in 10% formalin, the patient details were scrutinised, and the thyroidectomy specimens were fixed in fresh formalin for 24 hours. A gross description of all the fragments and processing were done. The hematoxylin and eosin slides were reviewed to confirm the diagnosis, and an IHC examination of Trop-2 was performed.
IHC staining method
Tissues for this study were obtained from the patients mentioned in the inclusion criteria at the Department of Pathology, MMCRI.
The tissues were embedded in paraffin and sliced into 2-4 micrometre sections mounted on adhesive-coated slides. Paraffin sections were deparaffinised by xylene and rehydrated by a graded alcohol. Sections were incubated for 5 minutes with 0.3% hydrogen peroxide at room temperature to block the endogenous peroxidase activity.
Heat-based antigen retrieval was performed to obtain optimal results. Sections were treated with 5% bovine serum albumin to block nonspecific staining. The slides were incubated with the primary anti-Trop-2 antibody (1:100, monoclonal antibody MR54, eBioscience, code 14-6024-82, Invitrogen). 3’,3’diaminobenzidine hydrochloride was used as chromogen and hematoxylin as a counterstain.
Assessment of IHC
Immunostained slides were evaluated. Normal thyroid tissue was employed as a negative control and validated PTC tissue as a positive control. Only the membranous staining was taken into account with no staining or with staining in 5% or less of the cells noted as negative, and membranous staining of more than 5% of the cells was considered positive with 1+(5-25%), 2+(26-50%), 3+(51-75%) and 4+(>75%); similar to guidelines followed by other studies [13, 14].
Results
The present study included 32 patients who presented thyroid swelling and were subjected to FNAC and, finally, thyroidectomy procedures. The study was conducted over 18 months, from December 2022 to March 2024, at the Department of Pathology, MMC &RI. The cases were thoroughly studied clinically and histopathologically. After analysing the data, the following observations were made.
The present study's age ranged from 23-71 years, with female predominance. The highest cases were in the age group of 31-40, and the least were older than 61 (Table 1). The mean age was 41 years. The current analysis showed a male-to-female ratio of 1:7, indicating a majority of women.
Table 1: Age distribution of the study population.
|
Age group(years)
|
Number of subjects
|
Percentage
|
|
20-30
|
4
|
12%
|
|
31-40
|
12
|
38%
|
|
41-50
|
9
|
28%
|
|
51-60
|
5
|
16%
|
|
61-70
|
1
|
3%
|
|
71-80
|
1
|
3%
|
In this study, there were three cases of diffuse thyroid disease, seven cases of multinodular goitre, and twenty-two cases of solitary thyroid nodules (Figure 1). The majority of the cases were euthyroid states followed by hypothyroidism presentation, and the least cases were in hyperthyroid states. None of the neoplastic cases were on any medications. The cases with deranged TFT were on off-and-on medications.
Of all the cases, the maximum was classical PTC, and the least were follicular and anaplastic thyroid carcinoma (Table 2).
Table 2: Distribution based on histomorphology.
|
Histomorphological Dx
|
No. of cases
|
|
Classic PTC
|
9
|
|
FVPTC
|
5
|
|
NIFTP
|
2
|
|
Follicular carcinoma
|
1
|
|
WDT-UMP
|
2
|
|
Anaplastic carcinoma
|
1
|
|
Oncocytic cell adenoma
|
2
|
|
Hashimoto’s Thyroiditis
|
2
|
|
Nodular Thyroid disease
|
3
|
|
Colloid Goiter
|
3
|
|
Follicular adenoma
|
2
|
|
Total
|
32
|
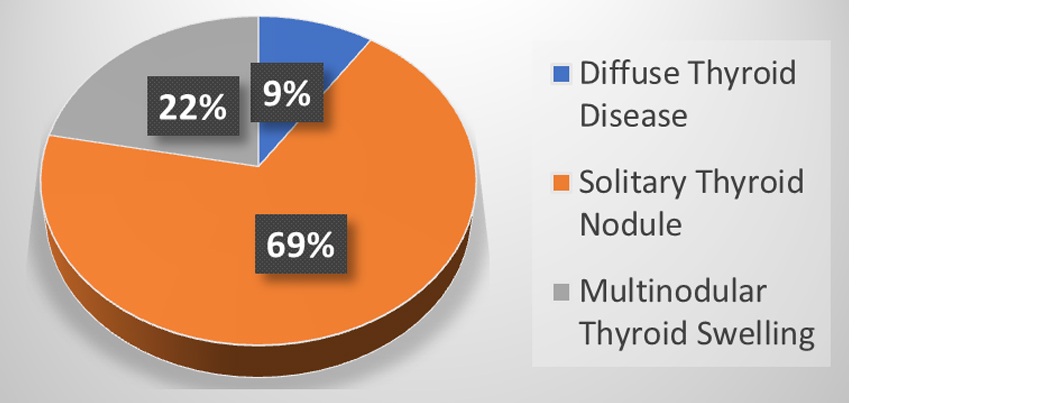
Figure 1: Distribution based on clinical findings.
Result of Trop-2 expression in thyroid lesions.
Of 32 cases, Trop-2 expression was seen in all cases of PTC (Figure 2). All the non-PTC thyroid carcinomas and benign thyroid lesions are negative for Trop-2 IHC expression. 2 cases of FVPTC were negative for Trop-2 expression (Figure 3). Weak positive Trop-2 staining was observed in one case of anaplastic thyroid cancer (Figure 4, Table 3).
Table 3: Distribution based on Trop-2 expression.
|
Diagnosis
|
Trop-2 positive
|
Trop-2 negative
|
|
Classic PTC (9)
|
9
|
0
|
|
FVPTC (5)
|
3
|
2
|
|
NIFTP (2)
|
0
|
2
|
|
FTC (1)
|
0
|
1
|
|
Anaplastic carcinoma (1)
|
1
|
0
|
|
WDT- UMP (2)
|
0
|
2
|
|
Oncocytic cell adenoma (2)
|
0
|
2
|
|
HT (2)
|
0
|
2
|
|
Nodular thyroid disease (3)
|
0
|
3
|
|
Colloid goitre (3)
|
0
|
3
|
|
Follicular adenoma (2)
|
0
|
2
|

Figure 2: Positive membranous staining for Trop-2 in classic PTC.
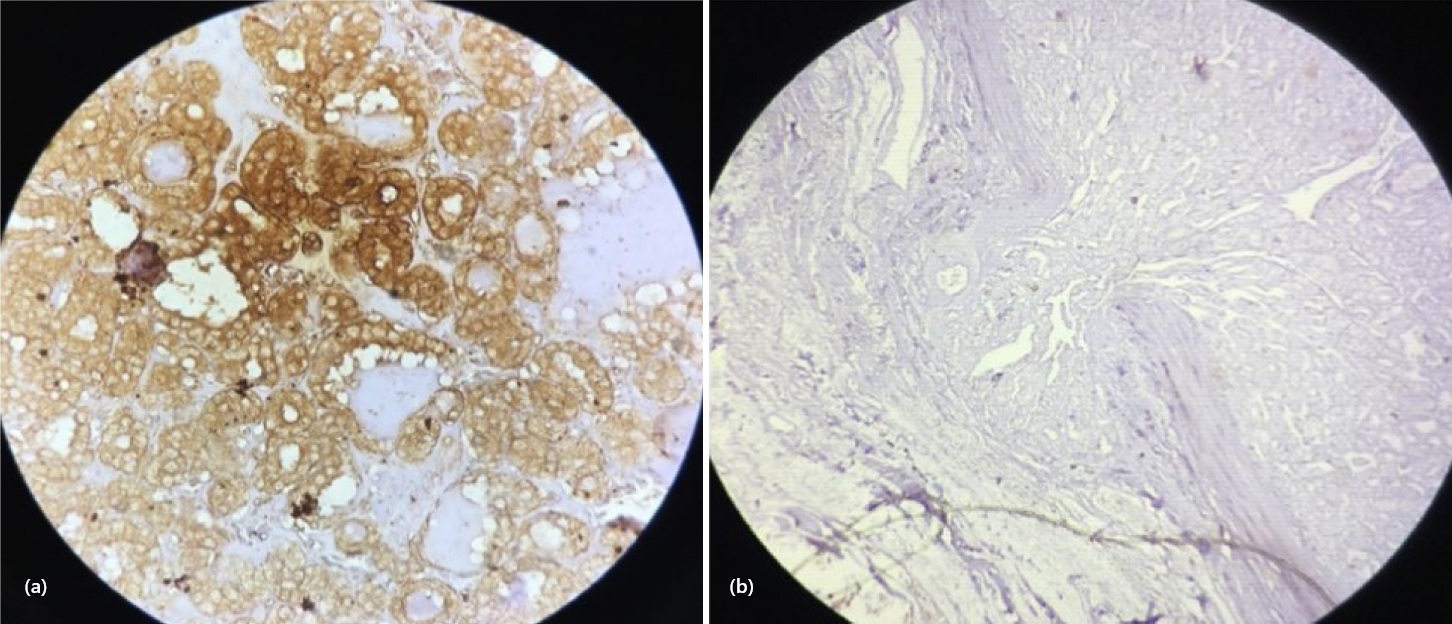
Figure 3: Trop-2 expression in FVPTC. a) Positive membranous b) Negative staining (Note: capsular invasion).

Figure 4: Weak positive staining in Anaplastic thyroid carcinoma.
Table 4: Statistical evaluations.
|
Statistic
|
Value
|
95% CI
|
|
Sensitivity
|
85.71%
|
57.19% - 98.22%
|
|
Specificity
|
94.44%
|
72.71% - 99.86%
|
|
Disease prevalence
|
43.75%
|
26.36% - 62.34%
|
|
Positive predictive value
|
92.31%
|
63.83% - 98.79%
|
|
Negative predictive value
|
89.47%
|
70.10% - 96.86%
|
|
Accuracy
|
90.62%
|
74.98%- 98.02%
|
The sensitivity and specificity of the current study were 85.71% and 94.4%, respectively. The result of the study was highly significant, with a P- value (< 0.05).
Discussions
Immunohistochemistry is an ancillary test for the definitive diagnosis of various thyroid lesions in the population. Though most diagnoses are based on histomorphological studies, some entities of thyroid lesions can have overlapping features. This makes it cumbersome for the further management process for the patient. Hence, IHC can be pivotal in the definitive diagnosis and additional management of thyroid lesions.
Trop-2 was a useful marker for differentiating between PTC, benign lesions, non-neoplastic lesions, and other thyroid neoplasms [16]. It is an oncogene that is upregulated in several human cancers while showing low to no expression in normal tissues. Its upregulation has been linked to poor prognosis in various cancers due to its pro-proliferative and pro-invasive properties [17].
The current study dealt with Trop-2 antigen expressions in various Thyroid lesions. A total of 32 various thyroid lesions with a mean age of 41 years was recruited for the tests. The Male to female ratio in the distribution of cases was 1:7.
In this study, we had taken 20 cases of malignant thyroid lesions, four benign thyroid lesions, and eight non-neoplastic thyroid lesions. Of the malignant lesions, only 2 cases showed cervical lymph node metastasis and one 1 case had infra-thyroidal extension. The mean age of the current study was 41 years, which was in line with Kong et al [3]. The current also presented the male-to-female ratio of 1:7, in line with Singh et al [1].
The sensitivity and specificity of this study were 85.71% and 94.4%, respectively, comparable to the findings of Addati et al [15] (Table 5).
Table 5: Comparative study based on sensitivity and specificity of Trop-2 expression in various studies.
|
Previous studies
|
Sensitivity
|
Specificity
|
|
Nesreen et al [6]
|
93.8%
|
94.1%
|
|
Nooshin et al [5]
|
93%
|
74%
|
|
Simms et al [4]
|
90%
|
95.2%
|
|
Addati et al [15]
|
87%
|
89%
|
|
Current study
|
85.71%
|
94.4%
|
Our study found significant expression of Trop-2 in PTC, especially in classic PTC. No intensity differences were found in classical PTC and FVPTC. All non-neoplastic thyroid lesions and benign lesions were entirely negative for Trop-2 expression. One case of anaplastic thyroid carcinoma showed a weak positive expression of Trop-2, indicating its potential to progress from PTC. None of the oncocytic cell lesions were stained positive.
The present study evaluated the Trop-2 expression in various thyroid lesions, especially in PTC and non-PTC lesions from other primary thyroid lesions. Most cases presented clinically as SNT (Solitary nodule thyroid) with female preponderance and a mean of 41 years.
The classic PTC displays beautiful membranous positivity (3 to 4+) for Trop-2 expression. 3 out of 5 cases of FVPTC showed Trop-2 positivity, and one ATC (Anaplastic Thyroid Carcinoma) showed Trop-2 immunoreactivity.
NIFTP Cases and other thyroid lesions were entirely negative for Trop-2 expression. Therefore, IHC for Trop-2 expression in thyroid lesions provides the definitive diagnosis and proper management.
The lacking point in our study was the unavailability of variants of PTC ( Papillary Thyroid Carcinoma) and the fact that there needs to be more cases that would have been more intensely studied
Conclusion
In conclusion, Thyroid disease is the most prevalent in the general population, yet the management of various thyroid lesions along with their hormonal abnormalities is controversial. Thus, the definitive diagnosis of these lesions is the scaffold for further management. Immunohistochemistry provides definitive aid for its diagnosis, rendering proper care and treatment.
Conflicts of interest
Authors declare no conflicts of interests.
References
[1] Singh V, Bagga PK, Singh B. Application of Thyroid Peroxidase (TPO) and Hector Battifora Mesothelial–1 (HBME–1) immunohistochemical markers in diagnosing papillary thyroid carcinoma of the thyroid. Int J Med Res Rev. 2020; 8:110–117.
[2] Sumana BS, Shashidhar S, Shivarudrappa AS. Galectin–3 immunohistochemical expression in thyroid neoplasms. J Clin Diagn Res. 2015; 9:EC07–EC11.
[3] Kong JS, Kim HJ, Kim MJ, Kim A, Lee D, et al. The significance of TROP2 expression in predicting BRAF mutations in papillary thyroid carcinoma. J Pathol Transl Med. 2018; 52:14–20.
[4] Simms A, Jacob RP, Cohen C, Siddiqui MT. TROP‐2 expression in papillary thyroid carcinoma: potential diagnostic utility. Diagn Cytopathol. 2016; 44 :26–31.
[5] Zargari N, Mokhtari M. Evaluation of diagnostic utility of immunohistochemistry markers of TROP–2 and HBME–1 in diagnosing thyroid carcinoma. Eur Thyroid J. 2019; 8:1–6.
[6] Nesreen HH, Manal SZ, Mohamed AM. Diagnostic utility of trophoblastic cell surface antigen 2 immunohistochemical expression in papillary thyroid carcinoma. J Pathol Nepal. 2018; 8:1235–1243.
[7] Asmaa GA, Nehal MN, Rania AA, Mohammed IS. The diagnostic validity of TROP–2 in recognizing papillary thyroid carcinoma. Med J Cairo Universit. 2018; 86:4349–4355.
[8] Abdou AG, Shabaan M, Abdallha R, Nabil N. Diagnostic value of TROP–2 and CK19 expression in papillary thyroid carcinoma in surgical and cytological specimens. Clin Pathol. 2019; 12.
[9] Shvartsur A, Bonavida B. Trop2 and its overexpression in cancers: regulation and clinical/therapeutic implications. Genes & cancer. 2015; 6:84.
[10] Bychkov A, Sampatanukul P, Shuangshoti S, Keelawat S. TROP–2 immunohistochemistry: a highly accurate method in the differential diagnosis of papillary thyroid carcinoma. Anatom Pathol. 2016; 48:425–433.
[11] Liu H, Shi J, Lin F. The potential diagnostic utility of TROP–2 in thyroid neoplasms. Appl Immunohistochem Mol Morphol. 2016; 25:525–533.
[12] Guan H, Guo Z, Liang W, Li H, Wei G, et al. Trop2 enhances invasion of thyroid cancer by inducing MMP2 through ERK and JNK pathways. BMC cancer. 2017; 17:10.
[13] Murtezaoglu AR, Gucer H. Diagnostic value of TROP–2 expression in papillary thyroid carcinoma and comparison with HBME–1, galectin–3 and cytokeratin 19. Pol J Pathol. 2017; 68:1–10.
[14] Eid A, Safia HA. TROP–2: a unique immunohistochemical marker for diagnosis of papillary thyroid carcinoma. Int J Cancer Biomed Res. 2021; 5:17–26.
[15] Addati T, Achille G, Centrone M, Petroni S, Popescu O, et al. TROP‐2 expression in papillary thyroid cancer: a preliminary cyto‐histological study. Cytopathology. 2015; 26:303–311.
[16] Turan Z, Erkılıç S. TROP2: A potential marker in diagnosis of thyroid neoplasms. Ir J Med Sci. 2023; 192:99–103.
[17] Attia AS, Hussein S, Sameh H, Khalil A, Waley AB, et al. Diagnostic and prognostic utility of TROP–2, SLP–2, and CXCL12 expression in papillary thyroid carcinoma. Cancer Biomark. 2024; 39:211–221.