Full Text
Introduction
Growing skull fracture (GSF), also known as a leptomeningeal cyst, is a rare but clinically significant complication of pediatric head trauma. It accounts for less than 1% of all skull fractures in children and is predominantly observed in those younger than three years of age, owing to the increased pliability of the calvarium and rapid brain growth during early childhood. The pathogenesis of GSF involves a linear skull fracture associated with an underlying dural tear, which permits herniation of arachnoid membrane, cerebrospinal fluid (CSF), and occasionally brain parenchyma through the fracture site. This leads to progressive enlargement of the bony defect over time due to pulsatile forces and impaired osteogenesis [1].
Clinically, GSF often presents as a progressively enlarging scalp swelling, which may be pulsatile and associated with neurological symptoms such as seizures, focal deficits, or developmental delay in advanced cases. The interval between initial trauma and clinical presentation can vary from weeks to months, frequently resulting in delayed diagnosis. Neuroimaging modalities, particularly computed tomography (CT) and magnetic resonance imaging (MRI), play a crucial role in confirming the diagnosis and delineating associated intracranial pathology [2].
Early recognition and prompt surgical intervention are essential to prevent long-term neurological sequelae and achieve satisfactory cosmetic outcomes. Surgical management typically involves excision of gliotic tissue, watertight dural repair (duraplasty), and reconstruction of the skull defect (cranioplasty). Despite its rarity, awareness of this entity among clinicians is vital for timely diagnosis and management [3, 4].
This case report aims to emphasize the importance of early recognition, accurate diagnosis, and timely surgical management of growing skull fracture to prevent complications and ensure favorable neurological and cosmetic outcomes in children.
Case presentation
A 3-year-old male child was brought to our neurosurgery outpatient department with complaints of a progressively enlarging swelling over the left frontal region for the past two months. The child had a history of head trauma following a fall from height approximately 15 months prior, for which no immediate medical attention was sought. The swelling was insidious in onset and gradually increased in size over time. It was described as pulsatile and non-tender, and was occasionally associated with irritability. There was no history of seizures, vomiting, loss of consciousness, or focal neurological deficits.
On general and neurological examination, the child was conscious, alert, and developmentally appropriate for age, with no focal neurological deficits. Local examination of the scalp revealed a soft, compressible, and pulsatile swelling measuring approximately 4 × 4 cm over the left frontal region near the midline. The overlying skin was normal, and the margins of the underlying bony defect were palpable, suggesting a defect in the calvarium.
Imaging findings
Non-contrast computed tomography (CT) of the brain with bone window settings demonstrated a well-defined defect in the left frontal bone with widening of the fracture margins. There was evidence of an associated dural defect with herniation of underlying brain parenchyma through the bony gap. Magnetic resonance imaging (MRI) of the brain further confirmed herniation of cortical tissue along with cerebrospinal fluid through the defect, consistent with a growing skull fracture. No significant mass effect, midline shift, or associated intracranial hemorrhage was noted.
Management and outcome
The patient underwent surgical intervention under general anesthesia. Intraoperatively, a dural defect with herniated gliotic brain tissue was identified. The gliotic tissue was carefully excised, followed by watertight duraplasty using an autologous pericranial graft. Cranioplasty was performed using the native bone to reconstruct the defect. The postoperative period was uneventful. At 3-month follow-up, the child remained asymptomatic with no neurological deficits and demonstrated a satisfactory cosmetic outcome (Figure 1).
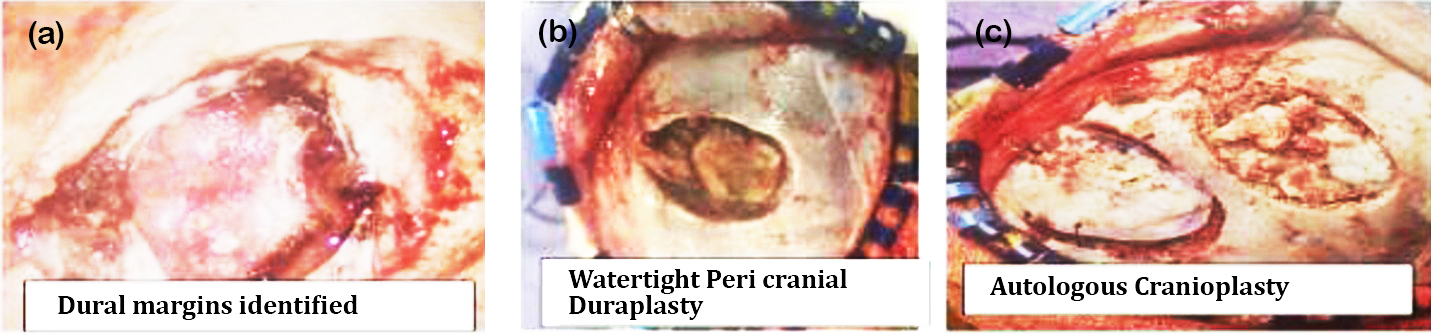
Figure 1: Intraoperative photos, (a) Dural margins identified, (b) Watertight peri cranial duraplasty, (c) Autologous cranioplasty.
Discussion
Growing skull fracture (GSF) is a distinctive complication of pediatric cranial trauma that arises from the combination of a linear skull fracture and an underlying dural tear. The dural defect permits herniation of leptomeninges and brain tissue, and the continuous pulsatile forces of the growing brain contribute to progressive widening of the fracture margins over time. This pathophysiological mechanism explains the delayed presentation commonly seen in affected children, often weeks to months after the initial injury [5].
The parietal bone is the most frequently involved site due to its anatomical vulnerability; however, frontal bone involvement, as observed in our case, is relatively uncommon and less frequently reported in the literature [6, 7]. Clinically, GSF typically manifests as a gradually enlarging, soft, and pulsatile scalp swelling. In advanced or neglected cases, patients may develop seizures, focal neurological deficits, or developmental delay, emphasizing the importance of early recognition [8]. Radiological evaluation plays a pivotal role in diagnosis. Computed tomography (CT) with bone window settings is highly effective in identifying calvarial defects and fracture diastasis, while magnetic resonance imaging (MRI) provides superior visualization of associated dural tears, herniated brain tissue, and any underlying gliosis or cystic changes.
Definitive treatment involves surgery with three key principles
The management of GSF is primarily surgical and should be undertaken promptly once the diagnosis is established. The first step involves meticulous excision of herniated and gliotic brain tissue to prevent further neurological compromise. The second and most critical step is achieving a watertight dural closure (duraplasty), commonly performed using an autologous pericranial graft, which minimizes the risk of cerebrospinal fluid leakage and recurrence. The third step is reconstruction of the bony defect (cranioplasty), preferably using autologous bone to ensure optimal integration and cosmetic outcome.
Early surgical intervention is associated with excellent prognosis, with most patients achieving good neurological recovery and satisfactory cosmetic results. Delay in treatment, however, may lead to persistent neurological deficits, epilepsy, and progressive cranial deformity, underscoring the need for timely diagnosis and management [6-9].
An important aspect in the management of growing skull fractures is the emphasis on early recognition and close follow-up of pediatric head injuries, even when the initial trauma appears trivial. Minor head injuries in young children are often underestimated, and the absence of immediate neurological symptoms may delay medical evaluation. However, persistent scalp swelling, especially if progressive or pulsatile, should raise suspicion for an underlying dural tear and evolving GSF. Regular clinical surveillance and timely imaging in such cases can facilitate early diagnosis. Furthermore, advances in neurosurgical techniques and imaging modalities have significantly improved outcomes, allowing precise delineation of pathology and effective surgical planning. Long-term follow-up is equally essential to monitor for recurrence, seizure development, or neurocognitive deficits. Educating caregivers about warning signs after head injury can play a crucial role in reducing delays in diagnosis and ensuring timely intervention.
Conclusion
Growing skull fracture is an uncommon yet clinically significant complication of pediatric head trauma that requires a high index of suspicion, particularly in young children presenting with progressive scalp swelling following even minor injury. Early recognition through careful clinical evaluation and appropriate neuroimaging, including CT and MRI, is crucial for accurate diagnosis and assessment of the underlying pathology. Prompt surgical intervention remains the cornerstone of management and is essential to prevent long-term complications such as seizures, neurological deficits, and cranial deformities. With timely and appropriate treatment, the prognosis is generally excellent, with most patients achieving satisfactory neurological recovery and cosmetic outcomes. Increased awareness among clinicians and caregivers regarding this entity can facilitate early diagnosis and improve overall patient outcomes.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Yan HJ. Epidural hematoma following use of a three–point skull clamp. J Clin Neurosci. 2007; 14:691–693.
[2] Li Q, Li J, Lv F, Li K, Luo T, et al. A multidetector CT angiography study of variations in the circle of Willis in a Chinese population. J Clin Neurosci. 2011; 18:379–383.
[3] Raimondi AJ, Gutierrez FA. Growing fractures of the skull in children. J Neurosurg. 1976; 45:455–460.
[4] Di Rocco C, Iannelli A, Caldarelli M. Growing fractures of the skull. Childs Brain. 1980; 6:81–94.
[5] Mahapatra AK, Tandon PN. Growing skull fractures: a clinical study of 41 patients. J Neurosurg. 2003; 99:164–168.
[6] Akhaddar A, Elmostarchid B, Boucetta M. Growing skull fractures: Case report and review of the literature. Surg Neurol. 2009; 71:223–226.
[7] Yilmaz A, Kiymaz N, Yilmaz N. Growing skull fractures in children: clinical features and surgical management. Childs Nerv Syst. 2012; 28:269–274.
[8] Sharma S, Sinha VD, Singh D. Management of growing skull fracture: a study of 22 cases. Pediatr Neurosurg. 2014; 50:274–281.
[9] Ramdasi R, Nadkarni T. Growing skull fractures: A clinical study of 32 patients. J Neurosurg Pediatr. 2019; 23:549–556.