Full Text
Introduction
Recurrent wheezing in early childhood is a major cause of respiratory morbidity, leading to frequent healthcare visits and a substantial economic burden. It affects a large proportion of children under five years of age and is commonly precipitated by upper respiratory tract infections (URTI). Among the viral etiologies, respiratory syncytial virus (RSV) and rhinovirus are the most frequently implicated pathogens associated with recurrent wheezing episodes throughout childhood [1].
Iron deficiency anaemia (IDA) remains the most prevalent nutritional disorder worldwide, with a disproportionately higher burden among children in low- and middle-income countries. According to the World Health Organization, approximately 40% of children under five years of age were anaemic in 2019 [2]. Although iron deficiency and IDA have been identified as risk factors for lower respiratory tract infections and bronchial asthma in several studies over the past two decades [3,4], evidence specifically linking iron deficiency anaemia with recurrent wheezing is limited. Therefore, this study was undertaken to evaluate the association between anaemia and recurrent wheezing in children.
The objectives of this study were to estimate the prevalence of iron deficiency, with and without anaemia, among childhood wheezers, and to compare iron status across different wheezing phenotypes.
Materials and methods
This was a hospital-based cross-sectional observational study conducted in the Department of Pediatrics at ESI-PGIMSR, ESIC Medical College and Hospital, over a period of 18 months (July 2023 to December 2024). Ethical clearance was obtained from the Institutional Ethics Committee of PGIMSR and ESIC Medical College, Joka. Written informed consent was obtained from the parents or legal guardians of all participating children.
Inclusion criteria: Children aged 1–12 years were included in the study if they met either of the following criteria: the presence of respiratory symptoms with wheeze on clinical examination, or a documented history of physician-diagnosed wheeze within the preceding 12 months.
Exclusion criteria: Children with conditions known to affect iron status or ferritin levels were excluded from the study. These conditions included acute febrile illness at presentation, chronic inflammatory diseases, liver disorders, hematological disorders, congenital heart disease, malabsorption syndromes, and prior receipt of oral or parenteral iron therapy within the preceding three months. To minimise the influence of inflammation on ferritin levels, children with clinical evidence of acute infection were excluded, and only those with C-reactive protein (CRP) levels <5 mg/L were included in the analysis.
Sample size: The sample size was determined based on the feasibility of recruitment within the defined study period at a single centre. Although an ideal sample size for estimating prevalence with 5% precision and 95% confidence would be approximately 384, the expected number of eligible children during the study period was substantially lower. Therefore, the study was designed as an exploratory, hypothesis-generating cross-sectional analysis. A total of 96 consecutively enrolled children who fulfilled the inclusion criteria and had complete laboratory data were included. This sample size was considered adequate to describe iron status patterns and to assess potential associations with wheezing phenotypes.
Operational definitions
Wheeze was defined as a high-pitched, musical, adventitious lung sound produced by airflow through an abnormally partially narrowed or compressed lower airway.
Wheezing phenotypes were classified based on the number of wheezing episodes in the preceding 12 months, using definitions adapted from the Asthma Predictive Index (API) [5]. Children with 1–2 episodes per year were classified as having infrequent episodic wheeze. Those with three or more episodes per year were classified as having recurrent episodic wheeze. Children with six or more episodes per year, or at least one episode per month, were classified as having frequent wheeze.
Table 1: Serum ferritin levels (in µg/l) according to WHO 2020 guidelines [6] adjusting for inflammation.
|
Age
|
Ferritin cut-off (no inflammation, CRP<5mg/L)
|
Ferritin cut-off( inflammation, CRP >5mg/L)
|
|
6-23 months
|
<12
|
<30
|
|
24-59 months
|
<12
|
<30
|
|
5-9 years
|
<15
|
<70
|
|
10-12 years
|
<15
|
<70
|
Anaemia was defined as a hemoglobin concentration below the established cut-off for age, sex, and physiological status. The World Health Organization (WHO) age-specific cut-offs [7] were used for classification. Accordingly, anaemia was defined as hemoglobin <11.0 g/dL in children aged 6 months to 4 years, <11.5 g/dL in children aged 5–11 years, and <12.0 g/dL in children aged 12 years.
Iron status was categorised according to WHO recommendations [6], using ferritin concentrations (adjusted for C-reactive protein [CRP]) to define iron deficiency (Table 1) and WHO haemoglobin thresholds to define anaemia [7]. Iron deficiency anaemia (IDA) was defined as low ferritin (adjusted for CRP) in the presence of haemoglobin below the WHO age-specific cut-offs. Iron deficiency without anaemia (ID) was defined as low ferritin (adjusted for CRP) with normal haemoglobin levels. Normal iron status was defined as normal ferritin and haemoglobin levels, along with transferrin saturation greater than 16%.
Data collection
A structured proforma was used to record demographic details, clinical history (age at onset of wheeze, number of episodes, atopy, family history of asthma), and medication use. All children underwent detailed physical examination including anthropometry and auscultation for wheeze. Venous blood samples were collected during clinically stable periods (no fever >38°C and no acute respiratory infection in last 72 hours) to assess hemoglobin, Red Blood Cell Indices, serum ferritin, serum iron, total iron-binding capacity (TIBC), transferrin saturation and C-Reactive Protein (CRP). Children were categorized as iron-deficient based on WHO guidelines [6], using age-appropriate ferritin cut-off values. Because ferritin is an acute-phase reactant, only samples with normal CRP were considered eligible for defining iron deficiency. Iron deficiency and anaemia were classified according to WHO guidelines [7].
Statistical analysis
Descriptive and inferential statistics were used to summarize participant characteristics and laboratory parameters using SPSS version 26.0. Continuous variables are presented as mean ± standard deviation (SD) and range, while categorical variables are presented as frequencies and percentages.For inferential analysis, categorical variables were compared using the Chi-square test and continuous variables were compared across groups using one-way ANOVA and Kruskal-Wallis test as appropriate. The association between serum ferritin levels and wheezing severity was assessed using Spearman’s rank correlation coefficient. A p-value <0.05 was considered as statistically significant.
Results
A total of 96 participants was included in the study. The mean age of children was 4.97±2.95 years with a range of 1-12 years. Out of 96 participants, 61(63.5%) were male and the rest 35(36.5%) were females. In our study, one-third (28.1%) of children had history of atopy/eczema; almost half (44.8%) of children had a family history of asthma and one-fifth (20.8%) of children had some history of food allergy. The study highlighted that iron deficiency anaemia was present in 33.3% and iron deficiency in 36% of the cases (Tables 2 and 3).
Table 2: Prevalence of iron deficiencyamong wheezing children.
|
Total sample
|
Iron deficiency anaemia
|
Iron deficiency without anaemia
|
Normal iron status
|
|
96
|
32(33.3%)
|
36(37.5%)
|
28(29.1%)
|
Table 3: Descriptive statistics of the laboratory parameters of the participants (n=96).
|
Variable
|
Mean
|
Standard Deviation
|
Minimum
|
Maximum
|
|
Hemoglobin(g/dl)
|
10.82
|
1.82
|
10
|
14.40
|
|
MCV (fL)
|
71.34
|
8.37
|
43
|
86
|
|
MCH (pg)
|
28.9
|
3.49
|
11.9
|
26
|
|
MCHC(g/dl)
|
31.76
|
2.72
|
21.3
|
39.5
|
|
WBC Total count (cells/mm3)
|
8025.72
|
2242.14
|
4600
|
13700
|
|
Eosinophil (cells/mm3)
|
2.78
|
1.25
|
1
|
6
|
|
C-Reactive Protein (mg/dl)
|
4.22
|
2.02
|
0.4
|
12.2
|
|
Serum ferritin (µg/l)
|
39.18
|
26.9
|
4.3
|
138.6
|
|
Serum iron (µg/dl)
|
36.18
|
26.2
|
10
|
163
|
|
Serum TIBC (µg/dl)
|
318
|
66.8
|
206
|
437
|
|
Transferrin saturation (%)
|
11.83
|
6.75
|
3
|
41.4
|
In our study we observed significant differences in hematological and iron parameters across the three wheezing phenotype groups. Children with frequent wheeze had the lowest mean hemoglobin, MCV, MCH, serum ferritin, transferrin saturation, and the highest TIBC values, indicating a markedly poorer iron status compared to the other groups. In contrast, infrequent wheezers demonstrated the most favourable hematological and biochemical profiles, with higher mean hemoglobin, ferritin, iron levels, and transferrin saturation. All parameters showed statistically significant variation among the groups (p < 0.001 for most measures), suggesting a strong association between wheezing frequency and iron deficiency (Table 4).
Table 4: Comparison of haematological parameters and Iron indices across wheezing phenotypes.
|
Parameters
|
Infrequent wheeze
(Mean ± SD)
|
Frequent wheeze
(Mean ± SD)
|
Recurrent wheeze
(Mean ± SD)
|
p-value
|
|
Hemoglobin (g/dl)
|
12.25 ± 0.95
|
9.05 ± 1.30
|
11.85 ± 1.09
|
<0.0001
|
|
MCV(fL)
|
79.35 ± 5.53
|
66.32 ± 7.90
|
73.00 ± 3.46
|
<0.0001
|
|
MCH(pg)
|
28.65 ± 3.07
|
21.95 ± 3.43
|
25.20 ± 2.13
|
<0.0001
|
|
MCHC(g/dl)
|
33.81 ± 1.84
|
31.58 ± 2.76
|
31.18 ± 2.78
|
<0.0001
|
|
Serum ferritin (µg/dl)
|
26.53 ± 6.29
|
13.85 ± 4.03
|
22.85 ± 5.96
|
<0.0001
|
|
Serum iron (µg/dl)
|
40.13 ± 16.29
|
25.18 ±13.13
|
33.63 ± 12.92
|
<0.0001
|
|
Serum TIBC
(µg/dl)
|
352.75 ±51.36
|
650.04 ±58.38
|
342.71 ±55.14
|
<0.0001
|
|
Transferrin saturation (%)
|
15.96 ± 8.81
|
9.50 ± 4.41
|
11.76 ± 5.87
|
<0.0001
|
Note: Test used- Kruskal–Wallis test.
In our study, the distribution of iron status varied significantly across the three wheezing phenotypes. Children with frequent wheeze demonstrated the highest burden of iron deficiency anaemia (IDA), with more than half (51.1%) falling into this category. In contrast, recurrent wheezers had a much lower prevalence of IDA (20%) but showed a predominance of iron deficiency without anaemia (34.3%), suggesting early depletion of iron stores without a fall in hemoglobin. Infrequent wheezers exhibited the most favourable profile, with 62.5% having normal iron status, and comparatively lower proportions of IDA (12.5%) and ID without anaemia (25.5%) (Table 5).
Table 5: Distribution of Iron status across wheezing Phenotypes.
|
Wheezing phenotype
|
Iron deficiency anaemia
|
Iron deficiency without anaemia
|
Normal iron status
|
|
Infrequent (n=16)
|
2(12.5%)
|
4(25.5%)
|
10(62.5%)
|
|
Frequent(n=45)
|
23(51.1%)
|
20(44.4%)
|
2(4.44%)
|
|
Recurrent(n=35)
|
7(20%)
|
12(34.3%)
|
16(45.7%)
|
Note: Test used- Chi square test. P-value- 0.0021.
Correlation between ferritin and wheezing phenotype
A significant negative correlation was observed between serum ferritin levels and wheezing phenotype severity (Spearman’s ρ = –0.376, p = 0.00016) (Figure 1). As the frequency of wheezing episodes increased from infrequent to recurrent and frequent categories, serum ferritin values demonstrated a progressive decline. Figure 1 illustrates the distribution of ferritin levels across the three wheezing phenotypes, showing the lowest median ferritin concentrations among children with frequent wheeze, whereas recurrent and infrequent wheezers exhibited comparatively higher levels. This pattern supports the association between poorer iron status and increasing wheezing severity.
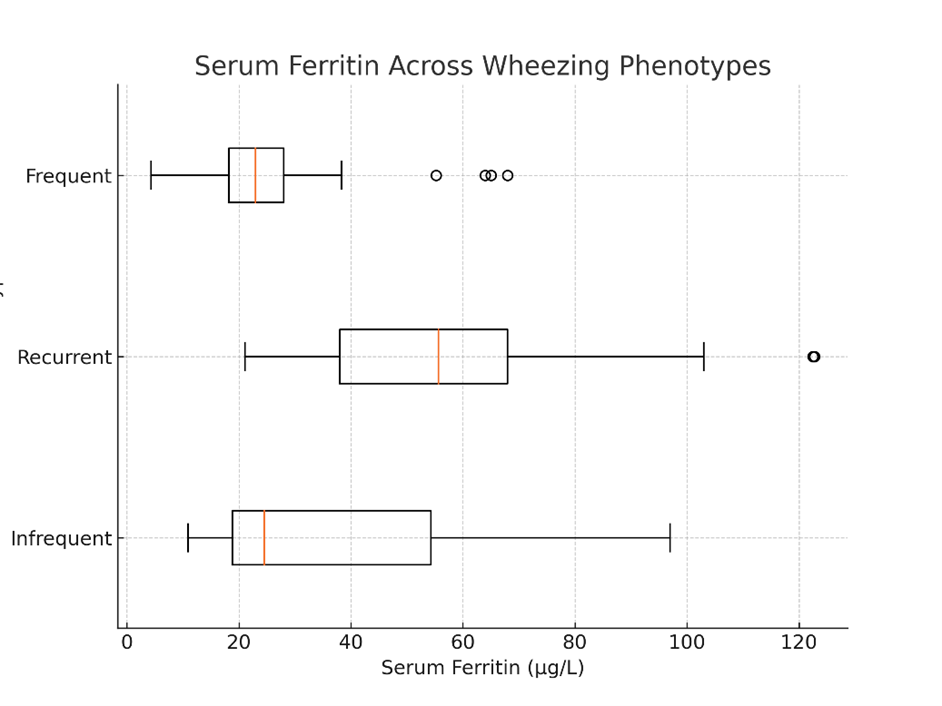
Figure 1: Boxplot illustrating the distribution of serum ferritin levels across the three wheezing phenotypes.
Discussion
In our study, the participants had a mean age of 4.97 ± 2.95 years, with an age range of 1–12 years. Of the total 96 cases, 63.5% were male and 36.5% were female. These findings are comparable to those reported by Agarwal et al. [8], in which the mean age was 2.49 ± 0.88 years and 62% of participants were male. Similarly, Ahmmad et al. [3] reported a male-to-female ratio of 1.6:1 in their study population.
In the present study, 33.3% of participants had iron deficiency anaemia (IDA), 37.5% had iron deficiency without anaemia (ID), and 29.1% had normal iron status. A cohort study by Eissa et al. [9] reported comparable findings, with significantly higher rates of IDA among asthmatic children (66%) compared with non-asthmatic controls (24%). A case–control study from Bangladesh [3] also demonstrated that the prevalence of IDA among wheezing children was 33%, compared to approximately 23% among controls. In contrast, Fida and Kamfar [10] reported a lower prevalence of IDA (19.7%) in a cohort of 117 children with asthma. This lower prevalence may be attributed to differences in age distribution, socioeconomic background, or the severity of wheezing or asthma among participants. The relatively higher prevalence observed in our cohort may reflect underlying nutritional deficiencies, variations in socioeconomic status, or a greater burden and severity of wheezing among children presenting to a tertiary-care centre.
In our study, children with frequent wheeze demonstrated significantly poorer haematological and iron indices compared to those with infrequent or recurrent wheezing. The markedly lower haemoglobin, MCV, MCH, ferritin, serum iron, and transferrin saturation, along with elevated total iron-binding capacity (TIBC), indicate a more pronounced iron-deficient state in children experiencing more frequent wheezing episodes. These findings are consistent with previous studies suggesting that iron deficiency may exacerbate airway hyperreactivity and increase susceptibility to wheezing and asthma. Elsayed and Essa [11] observed that asthmatic children with lower iron stores had more severe symptoms, while Elngar et al. [12] reported poorer pulmonary function among iron-deficient wheezers. The association observed in our study suggests that iron deficiency may contribute to the pathophysiology of recurrent wheezing, possibly through mechanisms such as impaired oxygen transport, altered immune function, and increased susceptibility to respiratory infections. Furthermore, the presence of significantly better iron indices among infrequent wheezers strengthens this association.
Iron status differed significantly across wheezing phenotypes in our study. Children with frequent wheeze had the highest prevalence of IDA (51.1%), while recurrent wheezers more commonly exhibited iron deficiency without anaemia. Infrequent wheezers showed the most favourable iron profile, with nearly two-thirds (62.5%) having normal iron status. Similar observations have been reported in other studies. Elsayed and Essa [11] found that children with asthma had significantly lower haemoglobin, serum iron, and ferritin levels, with worsening iron status corresponding to increased asthma severity. Ali et al. [13] reported that iron-deficient children had poorer lung function and worse asthma control. Additionally, a Mendelian randomization study by Li et al. [4] suggested that iron deficiency anaemia may have a causal role in the development of asthma. The consistency between these findings and our results suggests that iron deficiency may contribute to increased severity or frequency of wheezing episodes. The observation that children with infrequent wheeze had better iron status further indicates that adequate iron levels may have a protective role against frequent wheezing. These findings highlight the importance of assessing iron status in children with recurrent wheeze and considering early correction of iron deficiency to improve respiratory outcomes.
A significant negative correlation was observed between serum ferritin levels and wheezing severity. Ferritin levels decreased progressively from infrequent to recurrent and frequent wheezing, with the lowest levels observed in children with the highest frequency of wheezing episodes. This finding indicates a meaningful association between iron status and wheezing frequency. Children with more frequent wheezing had markedly lower ferritin levels, suggesting that iron deficiency may contribute to increased airway vulnerability and recurrent respiratory symptoms. This correlation further supports the potential role of iron status assessment and correction in the management of children with recurrent wheezing.
Overall, our findings demonstrate a strong association between iron deficiency and wheezing in children, particularly among those with more frequent episodes. The consistently poorer iron indices observed in frequent wheezers, along with the significant negative correlation between ferritin levels and wheezing severity, suggest that iron deficiency may play an important role in the clinical expression of wheeze. Although the cross-sectional design of our study does not permit causal inference, the similarity of our findings with previous studies supports the potential clinical relevance of routine iron status assessment in children with recurrent wheezing. Early identification and correction of iron deficiency may represent a simple and cost-effective strategy to improve respiratory outcomes in this population. Further longitudinal studies with larger sample sizes are required to clarify causal relationships and to determine whether iron supplementation can reduce the frequency or severity of wheezing episodes.
Limitations: This study has several limitations. The sample size was small and from a single centre, limiting generalisability. Its cross-sectional design prevents causal inference. Despite excluding children with elevated CRP, subclinical inflammation may have affected ferritin levels. Wheezing classification relied on parental recall, introducing bias. Additionally, dietary, socioeconomic, and environmental factors were not assessed and may have influenced findings.
Conclusion
This study shows that iron deficiency is highly prevalent among children with wheezing, with 33.3% having iron deficiency anaemia and 37.5% having iron deficiency without anaemia. A strong association was observed between iron status and wheezing severity, with frequent wheezers showing the poorest iron profile and infrequent wheezers the most favourable. The progressive decline in ferritin levels with increasing wheezing frequency supports this relationship. Although causality cannot be established, these findings highlight the importance of routine iron assessment. Early detection and correction of iron deficiency may improve respiratory outcomes. Further longitudinal studies are needed to confirm these findings.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Zhou Y, Tong L, Li M, Wang Y, Li L, et al. Recurrent wheezing and asthma after respiratory syncytial virus bronchiolitis. Front Pediatr. 2021; 9:649003. [2] World Health Organization. Anaemia in women and children: WHO Global Health Observatory data repository. 2019; Available from: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children.
[3] Ahmmad BN, Sarker S, Hossain MM, Parvin R, Alam AS, et al. Role of iron deficiency anaemia as a risk factor for wheeze associated respiratory tract infection in children. Med Res Chronicles. 2023; 10:132–138.
[4] Li M, Chen Z, Yang X, Li W. Causal relationship between iron deficiency anemia and asthma: a Mendelian randomization study. Front Pediatr. 2024; 12:1362156.
[5] Castro-Rodriguez JA, Holberg CJ, Wright AL, Martinez FD. A clinical index to define risk of asthma in young children with recurrent wheezing. Am J Respir Crit Care Med. 2000; 162:1403–1406.
[6] World Health Organization. Guideline on use of ferritin concentrations to assess iron status in individuals and populations. Geneva: WHO; 2020.
[7] World Health Organization. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva: World Health Organization; 2011.
[8] Agrawal A, Gupta R, Sodhi KD, Raghav V. Is iron deficiency anaemia a risk factor for wheeze associated respiratory tract infection in children. J Nepal Paediatr Soc. 2014; 34:195–199.
[9] Eissa SA, Mohammad AA, Ibrahim SA, Abd-Elgwad ER, Soliman NS. Iron deficiency anemia as a risk factor in childhood asthma. Egypt J Chest Dis Tuberc. 2016; 65:733–737.
[10] Fida NM, Kamfar HZ. Is iron deficiency anemia a risk factor in asthmatic children? J King Abdulaziz Univ Med Sci. 2013; 20:3–14.
[11] Elsayed W, Essa E. Iron deficiency anemia, serum iron in children with bronchial asthma. Zagazig Univ Med J. 2017; 23:1–1.
[12] Elngar EF, Mesbah BE, Abdella A, Salem N. Assessment of iron deficiency anemia as a prognostic factor for childhood asthma. EC Paediatrics. 2019; 8:127–136.
[13] Ali HA, Deraz TE, Ibrahim NR, Mohamed YH, Ahmed AH. The role of iron status in pediatric asthma severity. J Blood Disord. 2020; 7:1059.