Case Report
2026
March
Volume : 14
Issue : 1
A case report on Primigravida with large unilocular benign ovarian cyst
Kunnaiah A
Pdf Page Numbers :- 42-44
Anitha Kunnaiah1,*
1Department of Gynecology, Yashoda Hospitals, Hitec City, Hyderabad, Telangana 500081, India
*Corresponding author: Dr. Anitha Kunnaiah, Senior Consultant Obstetrician & Gynaecologist, Laparoscopic & Robotic Surgeon, and Infertility Specialist, Department of Gynaecology, Yashoda Hospitals, Hitec City, Hyderabad, Telangana 500081, India. Email: anithak11422@gmail.com
Received 16 September 2025; Revised 17 November 2025; Accepted 28 November 2025; Published 9 December 2025
Citation: Kunnaiah A. A case report on Primigravida with large unilocular benign ovarian cyst. J Med Sci Res. 2026; 14(1):42-44. DOI: http://dx.doi.org/10.17727/JMSR.2026/14-8
Copyright: © 2026 Kunnaiah A et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Ovarian cysts in pregnancy are common. These are mostly benign and asymptomatic and are diagnosed incidentally using ultrasound as part of antenatal checkup or diagnosed symptomatically. Surgical management is done in case of cysts of large size to prevent complications and protect pregnancy. A 34-year-old primigravida with 24 weeks gestation presented with abdominal distension and heaviness. Ultrasonography revealed a large left ovarian cyst. The patient was surgically managed with laparoscopic left salpingo-oophoretomy. The post operative period remained uneventful, and patient was discharged within 24-hours with fetus in good condition and due for delivery. Surgical management of large ovarian cysts during pregnancy can improve outcomes for both the mother and the fetus. Laparoscopic techniques which are minimally invasive are preferred as they ensure fast recovery and fetal safety.
Keywords: ovarian cyst; pregnancy; laparoscopic salpingo-oophorectomy; benign unilocular ovarian cyst
Full Text
Introduction
Ovarian cysts are the fluid filled structures which form within or on the ovary and are mostly benign or malignant. Ovarian cysts are commonly detected during pregnancy and the increased incidence can be attributed to the use of ultrasonography in pregnancy [1].
In most cases, ovarian cyst in pregnant women may be asymptomatic while some may experience abdominal pain in case of large cyst. Although the ovarian cyst might be identified by ultrasonography and is clinically suspected when an abdominal mass feels distinct from gravid uterus or when pelvic-abdominal mass is larger than the expected gestation period [2].
Majority of ovarian cysts that arise during pregnancy are typically benign and maybe functional in nature. Surgical management of ovarian masses can be done if patient has any acute symptoms or if the size of the mass is greater than 5cm [3]. Laparoscopic procedures can be used to surgically treat big ovarian cysts during pregnancy, although can present clinical challenges and pose risks [4]. For surgical procedures during pregnancy, second trimester is considered as the safest period [5]. Laparoscopic surgery ensures early recovery as it involves minimal invasion and less pain [6].
In this case report, a primigravida with 24 weeks gestation who has been diagnosed with large left unilocular benign cyst is discussed. This case was surgically managed with left salpingo-oopherectomy following cyst aspiration. We emphasize that the timely and minimally invasive surgical procedure enabled patient ambulation on the same day and be discharged within 24 hours with due for delivery.
Case report
A 34-year-old primigravida at 24 weeks of gestation presented with symptoms of abdominal distension and heaviness, along with lower back pain. There were no reports of vaginal leakage, vaginal bleeding, or spotting. Her menstrual cycles were regular. Her obstetric history was uneventful. She had no known medical or surgical illnesses. All necessary investigations were done. Ultrasound revealed a large left ovarian cyst of 10x9 cm. On examination patient was conscious and coherent. Vital signs were satisfactory. Abdominal examination revealed a palpable mass approximating 32 weeks size. Fetal heart rate was good.
The patient was diagnosed with a large unilocular benign cyst and was advised and scheduled for surgery. A laparoscopic left salpingo-oophorectomy was performed under general anesthesia and strict aseptic conditions. A safe entry was achieved using a primary 5 mm optic trocar (Figure 1), and pneumoperitoneum was established. Under direct vision, two 5 mm left lateral ports, and one right lateral port were created. The ovarian cyst was punctured and the cystic fluid was aspirated and collected. Following the aspiration of the cyst, drainage was performed to reduce the size of the cyst and prevent wall spill. Drained ovarian cystic fluid was of 1000ml (Figure 2). After decompressing the cyst, the left salpingo-oophorectomy was carried out, left ovarian cyst wall with fallopian tube and ovary retrieved from umbilical port of 10 mm (Figure 3a, 3b). Thorough irrigation and suction were conducted, and no active bleeding was observed.
Intra and post operative periods were uneventful. Patient was ambulated same day and was discharged within 24 hours with due for delivery.

Figure 1: 5 mm Optic trocar.

Figure 2: 1000ml aspirated cystic fluid.
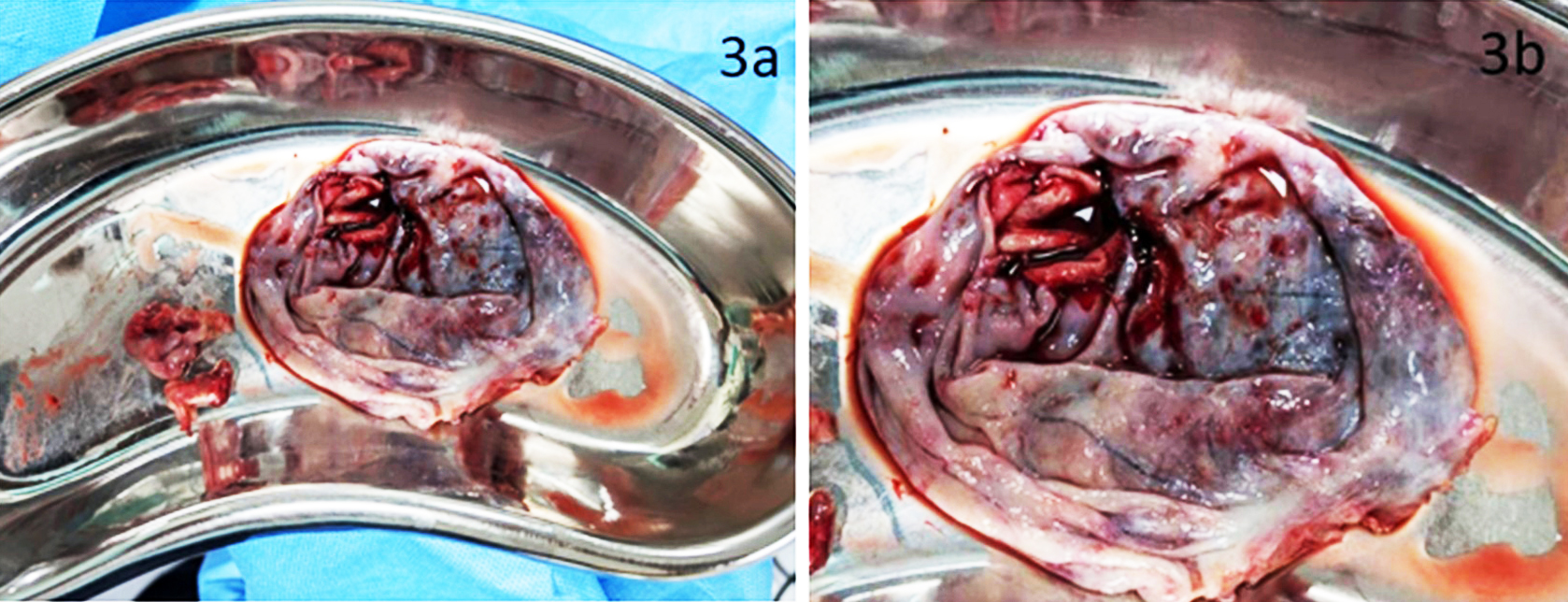
Figure 3a,b: Specimen- left ovarian cyst wall with fallopian tube and ovary retrieved from umbilical port.
Discussion
Ovarian cysts are commonly referred as ovarian masses or adnexal masses. Adnexal masses are benign and are incidentally found during pregnancy [7]. Mostly, these adnexal masses resolve on their own, but some cases might require surgical interventions such as cystectomy or salpingo-oophorectomy [8].
The present case describes the occurrence of large unilocular benign ovarian cyst in a primigravida with 24 weeks pregnancy who was presented with abdominal distension and heaviness. A similar case with similar gravidity status and symptoms was reported by Eichenberger et. al. in a case series of ovarian masses in pregnancy, where a 24-year-old primigravida with 24 weeks pregnancy, having clinical presentation of abdominal pain was diagnosed with left ovarian cyst [9].
Ovarian cysts in pregnant women are generally asymptomatic; however, symptoms may arise in case of cyst enlargement or cyst complications. Torsion, rupture, hemorrhage or mass effect are the common complications of ovarian cyst [10]. Abdominal distension and heaviness being the symptoms, it was indicative of cyst exerting pressure on surrounding tissue.
In view of preventing any further risks or complications and after thorough diagnosis of the case, patient was indicated for laparoscopic salpingo-oophorectomy. Procedures like laparoscopic salpingo-oophorectomy show advantages over traditional methods as they effectively manage ovarian masses with minimal complications, relatively reduced blood loss and faster recovery [11]. The patient of present case was surgically managed with laparoscopic salpingo-oopherectomy after cyst aspiration. A study conducted by Albobaid et al. reported five cases of large ovarian cysts where laparoscopy was used for surgical management. Laparoscopic salpingo-oophorectomy was performed after cyst draining in some cases and the study stated the significance and effectiveness of laparoscopic surgical management in suitable patients [12].
In our case, during the laparoscopic procedure gravid uterus was protected carefully and potential risks to maternal and fetal health were mitigated, thus demonstrating the feasibility and safety of laparoscopy in the case of large benign unilocular cyst in pregnant women. Similarly, Kurihara et al, also concluded in their study that laparoscopic surgery for ovarian cyst is effective and safe with no negative impact on pregnancy outcome [13].
Conclusion
Ovarian cysts in pregnancy are relatively common and can be managed surgically based on their size. Large ovarian cysts are mostly benign. These ovarian cysts are diagnosed incidentally during ultrasound or by performing ultrasound on the basis of patient’s symptoms. Timely surgical intervention through minimally invasive laparoscopic procedure ensures not only the effective management of ovarian cyst but also safety of ongoing pregnancy.
Acknowledgements
Management Yashoda Hospitals and Dr. Amidyala Lingaiah (Director-Medical Services) for the continuous support.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Bhagat N, Gajjar K. Management of ovarian cysts during pregnancy. Obstet Gynaecol Reprod Med. 2022; 32:205–210.
[2] Abdelhafez MA, Ahmed KA, Daud MNM, Jeffree MS, Eldiastey AMA, et al. Ovarian cysts and pregnancy: what is new? A literature review. J South Asian Feder Obstet Gynaecol. 2025; 16:268–274.
[3] Acharya K, Poudel D, Dahal S, Kuikel S, Adhikari A. A case of huge ovarian cyst in second trimester: A rare case report. Ann Med Surg (Lond). 2022; 82:104765.
[4] Martone S, Troìa L, Luisi S. Adnexal masses during pregnancy: management for a better approach. Gynecol Surg. 2021; 18:1–8.
[5] Manvi MR, Deshpande R. Ovarian mass in pregnancy: case series. Int J Reprod Contracept Obstet Gynecol. 2020; 9:4290–4294.
[6] Eltabbakh GH, Charboneau AM, Eltabbakh NG. Laparoscopic surgery for large benign ovarian cysts. Gynecol Oncol. 2008; 108:72–76.
[7] Senarath S, Ades A, Nanayakkara P. Ovarian cysts in pregnancy: a narrative review. J Obstet Gynaecol. 2021; 41:169–175.
[8] Jamdade K, Gajjar K. Management of ovarian cysts and cancer in pregnancy. Obstet Gynaecol Reprod Med. 2025; 35:128–137.
[9] Eichenberger–Gautschi T, Smith A, Sayasneh A. Ovarian masses in pregnancy: a single centre retrospective study. BJMP. 2018; 11:1109. [10] Zvi MB, Thanatsis N, Vashisht A. Ovarian cysts in pregnancy. Gynaecol Obstet. 2023; 1:1–3.
[11] Ojha V, Singhal VK, Alaswad FD, Sarfraz NS. Laparoscopic surgery in the management of ovarian masses. Obstet Gynecol Res. 2025; 8:25–30.
[12] Alobaid A, Memon A, Alobaid S, Aldakhil L. Laparoscopic management of huge ovarian cysts. Obstet Gynecol Int. 2013; 2013:380854.
[13] Kurihara K, Minagawa M, Masuda M, Fukuyama M, Tanigaki K, et al. The evaluation of laparoscopic surgery on pregnant patients with ovarian cysts and its effects on pregnancy over the past 5 years. Gynecol Minim Invasive Ther. 2018; 7:1–5.