Original Research
2021
December
Volume : 9
Issue : 4
Reclassification and histopathological study of vascular anomalies according to ISSVA (2018 revision) classification
Chilukuri S, Kallam AR, Gudeli V, Kolusu KVVR, Natukula K
Pdf Page Numbers :- 204-210
Swathi Chilukuri1,*, Anji Reddy Kallam2, Vahini Gudeli1, Veera Venkata Rakesh Kumar Kolusu1, and Kirmani Natukula3
1Department of Pathology, Alluri Sitarama Raju Academy of Medical Sciences, Eluru-534005, Andhra Pradesh, India
2Department of Plastic Surgery, Alluri Sitarama Raju Academy of Medical Sciences, Eluru-534005, Andhra Pradesh, India
3Multi Disciplinary Research Unit (MRU), Andhra Medical College, Visakhapatnam-530002. Andhra Pradesh, India
*Corresponding author: Dr. Swathi Chilukuri, Associate Professor, Department of Pathology, Alluri Sitarama Raju Academy of Medical Sciences, Eluru-534005, Andhra Pradesh, India. Tel.: +91-9394677522; Email: saiswathi25@gmail.com
Received 1 July 2021; Revised 27 August 2021; Accepted 6 September 2021; Published 16 September 2021
Citation: Chilukuri S, Kallam AR, Gudeli V, Kolusu KVVR, Natukula K. Reclassification and histopathological study of vascular anomalies according to ISSVA (2018 revision) classification. J Med Sci Res. 2021; 9(4):204-210. DOI: http://dx.doi.org/10.17727/JMSR.2021/9-31
Copyright: © 2021 Chilukuri S et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Vascular anomalies (VAs) represent a spectrum of disorders from simple birthmarks to life-threatening entities. Consistency in the terminology of vascular anomalies and diagnosis by routine histology is necessary for the proper diagnosis and clinical management.
Aim: The present study aimed to classify the vascular anomalies according to the 2018 revised classification of ISSVA and to evaluate the role of GLUT-1 (glucose transpoter protein isoform 1) immunomarker as a complementary tool to aid in differentiating vascular anomalies.
Materials and methods: In this retrospective study, clinical records of 47 cases reported as vascular anomalies from January 2017 to June 2019 were retrieved from the Department of Pathology, ASRAM Medical College, Eluru. The cases were analyzed based on findings of histochemical stains such as Verhoeff-van Gieson (VVG) and classified as per ISSVA. Further immunohistochemistry studies of GLUT-1 were done.
Results: Of 47 patients, the male to female ratio was found to be 1.06:1 and 46.80% of cases were vascular tumors, whereas 53.19% cases were vascular malformations in this study. Of 22 cases histologically diagnosed as vascular tumors, 06 cases were infantile hemangiomas and showed immunopositivity with GLUT-1 marker and the rest of vacular tumors and malformations were immuno negative for GLUT-1.
Conclusion: ISSVA classification provides a framework for understanding the morphology, guiding the treatment plan and prognosis. In addition to this, GLUT-1 precisely differentiated infantile hemangioma from other vascular tumors and malformations.
Keywords: vascular anomalies; GLUT-1, infantile hemangioma; vascular malformation; vascular tumors
Full Text
Introduction
Vascular anomalies are a diverse group of disorders that include tumors and malformations [1] which are often found in children and young adults. These anomalies may arise from arteries, veins, lymphatic vessels, and/or capillaries which are infrequent and complex in diagnosis and treatment. The term ‘hemangioma’ is commonly used by many authors for vascular tumors as well as malformations despite the differences in evolution, clinical course, morphology, and treatment whereas others continue to use the term cavernous hemangioma for venous malformation and port-wine stain for capillary malformation [2], venous malformation, and arterio venous malformations (AVM) [3], thus perpetuating the nostalgic confusion and the attendant problems.
The classification of vascular anomalies was first proposed by Mulliken and Glowacki in 1982 [4] and accepted by the International Society for the Study of Vascular Anomalies (ISSVA) which was revised in 2014 [5] and the latest update in 2018 [6]. This classification provides a common nomenclature for all the specialists and facilitates optimum diagnosis and treatment. The classification is based on clinical, radiological, and histopathological characteristics and divides vascular anomalies into vascular tumors (VTs) (neoplastic), vascular malformations (VMs) (non-neoplastic) and unclassified anomalies (unclear if tumor or malformation). VTs generally arise de novo and are neoplastic growths characterized by endothelial cell hyperproliferation. Lesions grow rapidly and most are not present at birth which are managed by active observation, medical, or surgical means considering the type of lesion, patient age, size,and location of the lesion [5, 7]. They are categorized into benign, borderline and malignant based on cellular behaviour. Benign vascular tumors comprise infantile hemangiomas, congenital hemangiomas, tufted angioma, spindle cell hemangioma, epithelioid hemangioma, pyogenic granuloma and others. Compared to VTs, VMs involve malformed vessels without endothelial cell proliferation and occur during the morphological development of vascular system. In contrast to the rapid growth and involution phases characteristic of VTs, VMs grow slowly, usually present at birth and become more evident as the child grows and require intervention [5, 7]. Vascular malformations are classified into simple, combined, of major named vessels, those associated with other anomalies. Their designations reflect the predominant vessel type involved. Table 1 shows the detailed ISSVA classification of vascular anomalies.
Table 1: Vascular anomalies classification according to ISSVA (2018 revision).
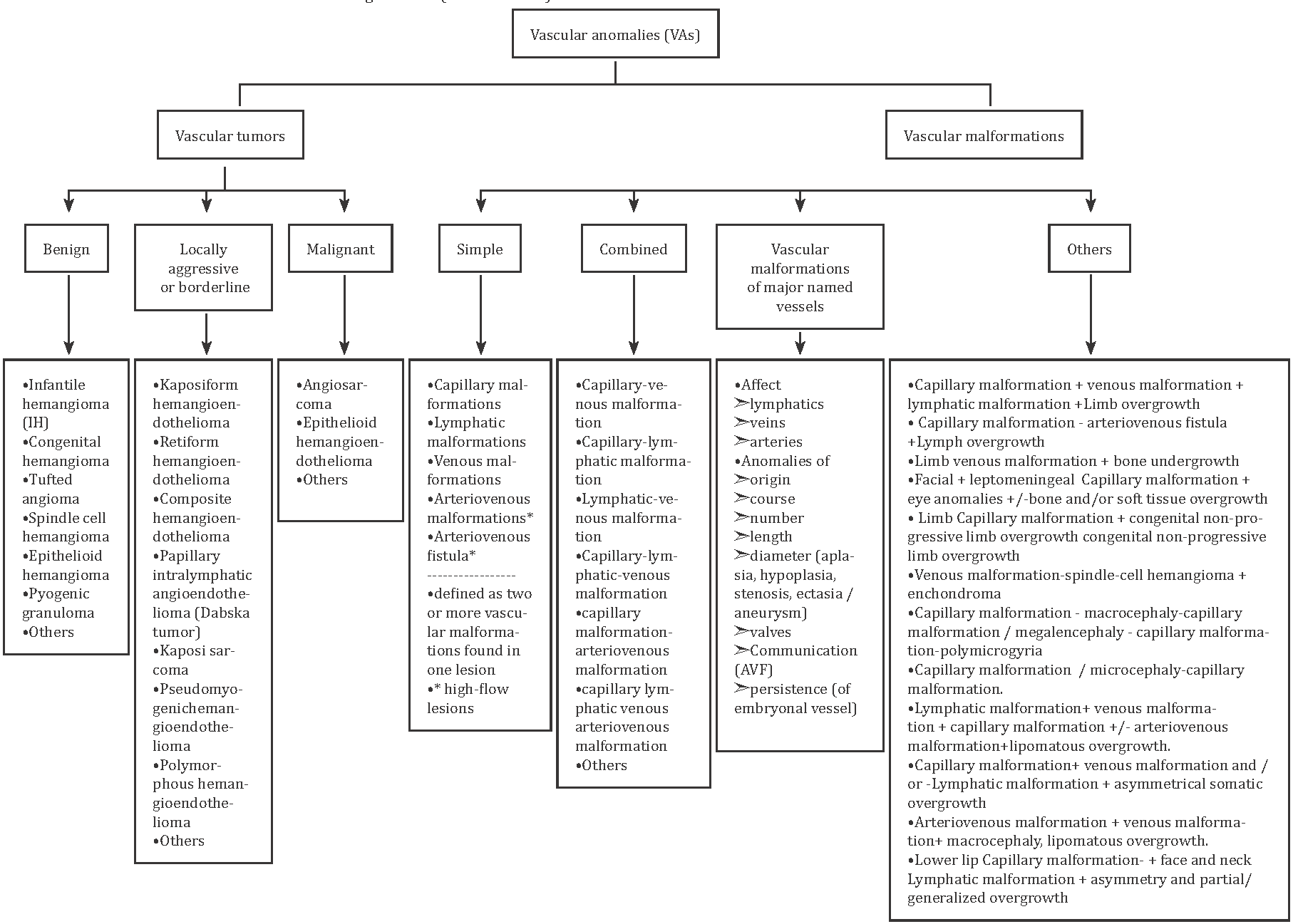
The commonly used terms such as capillary hemangioma/ port-wine stain had been replaced with capillary malformation and venous malformation for cavernous hemangioma in this classification.
Consistent and standard terminology of VAs is crucial for appropriate evaluation and management often requiring multidisciplinary specialists. The definitive diagnosis of VTs and VMs is important to avoid treatment failure and recurrences. Sometimes additional ancilliary studies are required besides routine histology for the differentiation of VTs and VMs. Here, we reclassified the vascular anomalies based on ISSVA classification and report our institutional experience of immunohistochemical marker GLUT-1 which distinguishes infantile haemangiomas from other histologically similar benign vascular tumors and malformations following the initial report by North and Colleagues in 1998 (2001) [8]. To further characterize the histomorphologic differences between hemangioma and AVM, special stains for elastic tissue to highlight internal elastic lamina were done.
Materials and methods
This is a retrospective study of 47 patients with diverse presentations of vascular anomalies with histopathological confirmation. Verhoeff- van Gieson stain was performed wherever necessary for the confirmation of AVM. IHC with GLUT-1 marker was done for the differentiation of vacular anomalies. This study was approved by our Institutional Ethics Committee with approval number IEC/ASR/APPROVAL/033/2019. Archived data of 47 patients with the diagnosis of vascular anomalies were accessed from the pathology department from January 2017 to June 2019.
Inclusion and exclusion criteria
Patients of all age groups ranging from 0 months to 75 years presented with vascular anomalies (benign vascular tumors which include hemangiomas and vascular malformations) proven histopathologically were included. Borderline and Malignant vascular tumors and where representative blocks were not available were excluded from the study.
Data regarding age, gender, and original histopathological diagnosis were collected and analyzed. The original diagnosis of all 47 cases was studied and categorized according to the ISSVA classification of vascular anomalies. The results obtained were further studied by immuno-profiling with GLUT-I marker for the all cases (n=47) to help in the definitive diagnosis of infantile hemangiomas.
Immunohistochemistry for GLUT-1
Paraffin block sections were deparaffinized followed by rehydration and citrate buffer antigen retrieval. All sections were protein blocked followed by incubation with primary antibody. Detection was performed using a peroxidase kit using DAB (diaminobutyric acid chromogen) system. Negative controls were processed in parallel without primary antibodies. Normal tissue immune reactivities served as internal positive control.
Statistical analysis
In the present study, results were expressed as a mean, ratio, absolute number, and percentages.
Results
Of 47 patients, 24 patients were males and 23 patients were females. The Male-Female ratio was 0.85:1 in VT group and 1.27:1 in the VM group. Male incidences were higher (56 %) in VM group than VT (45.45%). Female cases were predominant in VT group (54.55%) compared to VM (44%). Age ranging from 0 months to 75 years was considered in this study and VM were more common (23 cases) than VT in below 40 years of age group and a higher number of VTs (8 cases) were found in the age group of 40 and above when compared to VMs (Figure 1) .
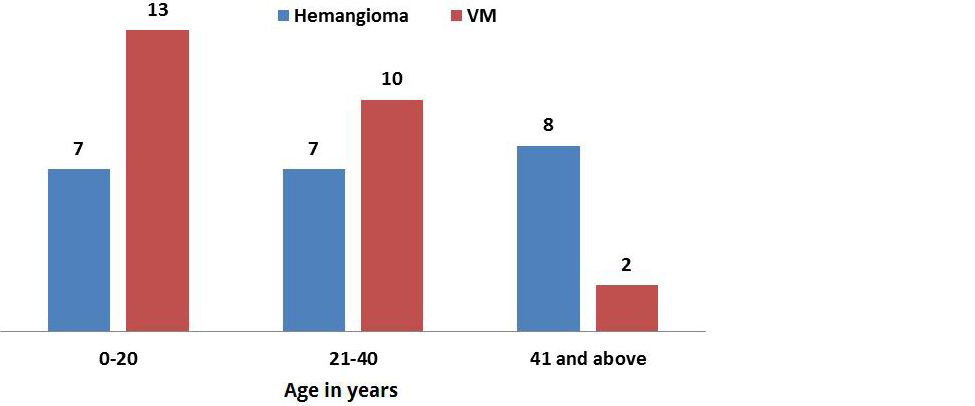
Figure 1: Graph showing age distribution in vascular anomalies.
In the present study, the most common site of VA was the head and neck region (55.3%) followed by extremities. Standard histopathology examination revealed 47 cases as, 11 cases of capillary Hemangioma, 9 cases each of cavernous hemangioma, Pyogenic granuloma, lymphangioma, and 8 cases of venous angioma and 1 case of AVM. Further, we reclassified these 47 cases according to updated ISSVA classification as 22 cases of vascular tumors and 25 cases of vascular malformations (Table 2).
Table 2: Showing the demographic, histopathological and ISSVA classification of cases with immune positivity of GLUT-1 marker in cases.
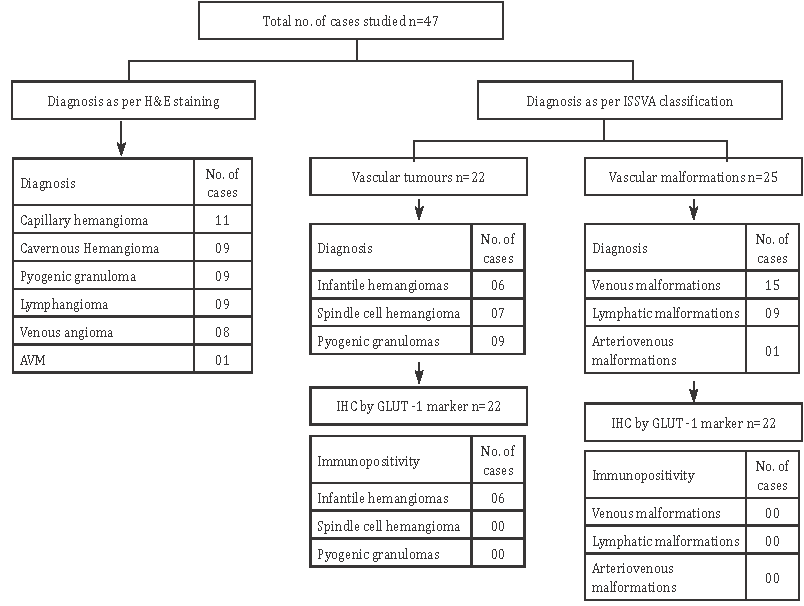
Out of 22 vascular tumors, infantile hemangiomas were 06 (Figure 2), spindle cell hemangiomas were 7 and pyogenic granulomas were 9. Of 25 vascular malformations, 15 cases were venous malformations (Figure 3), 09 cases were Lymphatic malformations (Figure 4), and 1 case of Arteriovenous malformation (Figure 5). Further, all the samples were studied with elastic tissue stain for the confirmation of AVM’s (Figure 6). IHC with GLUT-1 marker was performed on all the 6 infantile hemangiomas and remaining other cases of VTs and VMs which confirmed the positivity in all cases of infantile hemangiomas (6 cases) (Figure 7a) and the result was negative (Figure 7b) in the remaining group of vascular tumors and malformations. Figure 1 illustrates the overall results of the present study.
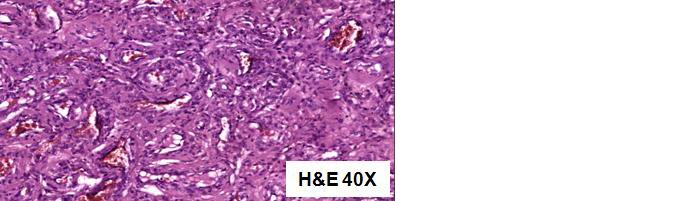
Figure 2: Infantile hemangioma- Composed of lobules of closely packed capillaries lined by plump endothelial cells.
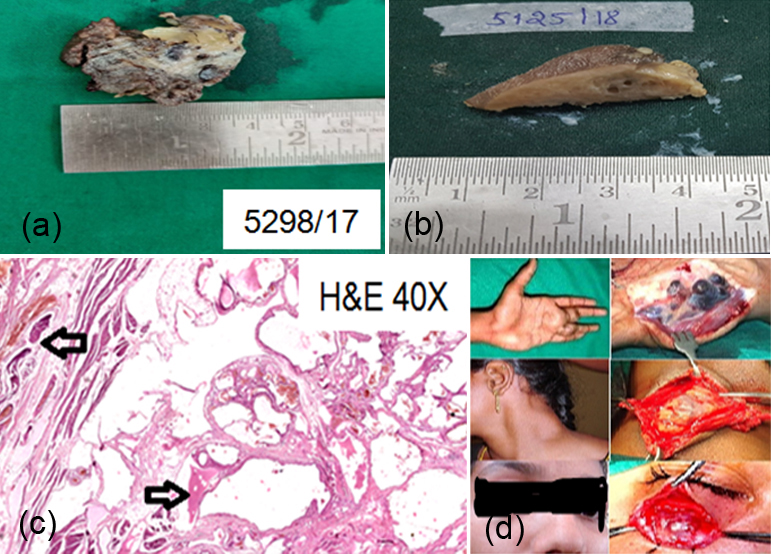
Figure 3a-d: Venous malformation- Large malformed, irregular venous channels with muscular walls with internal organizing thrombi.
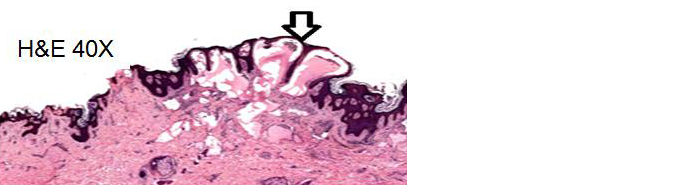
Figure 4: Lymphatic malformation- Papillary dermis is expanded by thin-walled lymphatic channels, accompanied by verruciform hyperplasia.
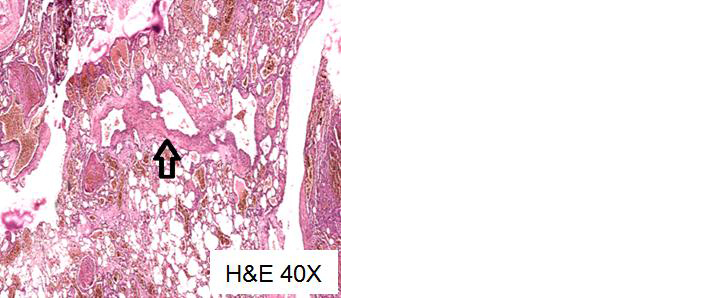
Figure 5: Arteriovenous malformation- Large and tortuous arteries, thick and thin walled veins are present.
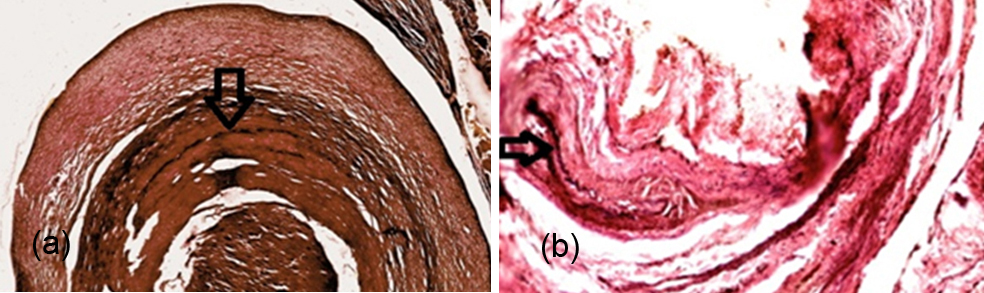
Figure 6a,b: AVM- Elastic stain highlights the disruption of elastic lamina characteristic of arteries (Verhoeff- van Gieson stain).
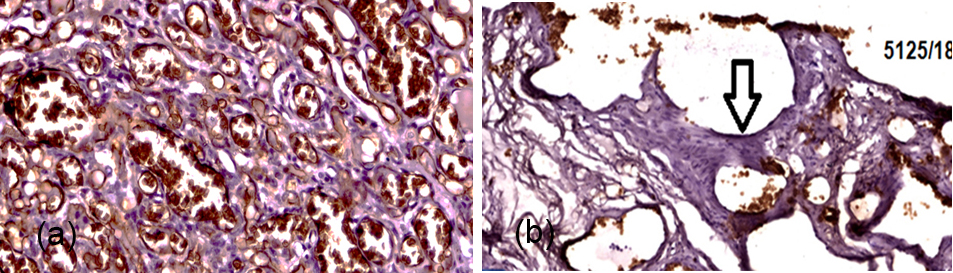
Figure 7: (a) GLUT-1 Positivity in endothelial cells in case of infantile hemangiomas, (b) GLUT-1 Negativity in endothelial cells in other cases of vascular anomalies.
Discussion
Vascular anomalies represent a spectrum of disorders that comprise tumors and malformations and can present as a simple birthmark to life-threatening entities. Vascular tumors are true tumors with the characteristic feature of rapid growth in vascular endothelium.
Vascular malformations comprise vascular dysmorphogenesis and normal endothelial growth. Misdiagnosis of vascular malformation as vascular tumor may lead to treatment failure and recurrences. Hence, a definitive diagnosis of both these lesions is essential. Few studies that used elastic tissue stains for differentiating hemangiomas and vascular malformations confirmed the definitive diagnosis. Adegboyega et al. [9] reclassified 12 of 101 cases of hemangiomas as AVMs and 2 of 66 cases of AVMs as hemangiomas. Similar way Pawane et al. [10] reclassified 10 of 60 cases of hemangiomas as AVMs. We also reclassified 3 cases of venous malformations as AVMs.
North et al. [11] introduced a new immunohistochemistry marker in the year 2000, Glucose transporter protein (GLUT1) which was proven for its sensitivity and specificity that can be used for the confirmation of IHs and also has proven useful as a complementary tool for assessment of differential diagnosis between various VAs and the prognosis of certain types of tumors [12-14]. In this study, he reported that intense immunoreactivity for GLUT-1 in IH, and no immunoreactivity was observed in any other type of VMs. We also found that all 6 cases of infantile hemangioma were positive for GLUT-1 which was similar to other studies. Mo et al., [15] concluded that GLUT-1 is an effective tool for differentiating between hepatic IHs and VMs. Oliveira et al. [16] analyzed the IHC expression of 30 cases each of oral hemangiomas and pyogenic granulomas. IHC was positive in 7 cases of hemangiomas, confirming as IHs, and the remaining cases were reclassified as PG or VM.
Conclusion
Vascular anomalies are a spectrum of disorders and have always been misdiagnosed in recent years. ISSVA provides a standard terminology for vascular anomalies which should be followed by multidisciplinary specialists to eliminate diagnostic and therapeutic errors. Advances in immunohistochemistry with GLUT1 like markers can be used for the differentiation o f vascular anomalies which helps the clinician to treat a patient. Thus, GLUT1 is a definitive and diagnostic marker for infantile hemangiomas.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Chang MW. Updated classification of hemangiomas and other vascular anomalies. Lymphat Res Biol. 2003; 1(4):259–265.
[2] Gampper TJ, Morgan RF. Vascular anomalies: hemangiomas. Plast Reconstr Surg. 2002; 110(2):572–585.
[3] Rydh M, Malm M, Jernbeck J, Dalsgaard CJ. Ectatic blood vessels in port wine stains lack innervation: possible role in pathogenesis. Plast Reconstr Surg. 1991; 87(3):419–422.
[4] Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982; 69(3):412–422.
[5] Merrow AC, Gupta A, Patel MN, Adams DM. 2014 revised classification of vascular lesions from the international society for the study of vascular anomalies: Radiologic-pathologic update. Radiographics. 2016; 36(5):1494–516.
[6] ISSVA classification of vascular anomalies ©2018 International Society for the study of vascular anomalies. Accessed 22 June 2021, Available from: https://www.issva.org/UserFiles/file/ISSVA-Classification-2018.pdf.
[7] Steiner JE, Drolet BA. Classification of vascular anomalies: An update. Semin Intervent Radiol. 2017; 34(3):225–232.
[8] North PE, Waner M, Mizeracki A, Mihm MC. GLUT-1: A newly discovered immunohistochemical marker for juvenile heangiomas. Hum Pathol. 2000; 31(1):11–22. [9] Adegboyega PA, Qiu S. Hemangioma versus vascular malformation: presence of nerve bundle is a diagnostic clue for vascular malformation. Arch Pathol Lab Med. 2005; 129(6):772–775.
[10] Pawane PA, Gangane N. Hemangiomas versus arterio-venous malformations: Role of elastic stains and mast cell density. Indian J Pathol Microbiol. 2014; 57(2):191–195.
[11] North PE, Waner M, Mizeracki A, Mrak RE, Nicholas R, et al. A unique microvascular phenotype shared by juvenile hemangiomas and human placenta. Arch Dermatol. 2001; 137(5):559–570.
[12] Filho TJS, Oliveira DHIP, Moura IS, Medeiros LKS, Gonzaga AKG, et al. Importance of GLUT1 in differential diagnosis of vascular anomalies. J Vasc Bras. 2015; 14:168–176.
[13] Vugt LJV, Vleuten CJMV, Flucke U, Blokx WAM. The utility of GLUT1 as a diagnostic marker in cutaneous vascular anomalies: A review of literature and recommendations for daily practice. Pathol Res Pract. 2017; 213(6):591–597.
[14] Huang L, Nakayama H, Klagsbrun M, Mulliken JB, Bischoff J. Glucose transporter 1-positive endothelial cells in infantile hemangioma exhibit features of facultative stem cells. Stem Cells. 2015; 33(1):133–145.
[15] Mo JQ, Dimashkieh HH, Bove KE. GLUT1 endothelial reactivity distinguishes hepatic infantile hemangioma from congenital hepatic vascular malformation with associated capillary proliferation. Hum Pathol. 2004; 35(2):200–209.
[16] Oliveira DH, Silveira EJ, Medeiros AM, Alves PM, Queiroz LM. Study of the etiopathogenesis and differential diagnosis of oral vascular lesions by immunoexpression of GLUT-1 and HIF-1α. J Oral Pathol Med. 2014; 43(1):76–80.