Full Text
Introduction
The larval stages of the tapeworm Echinococcus granulosus mostly cause the zoonotic parasitic disease echinococcosis/ hydatidosis. The larval stage undergoes development within intermediate hosts, which may include humans, whereas the adult stage is typically found among carnivorous animals. The manifestation of clinical disease primarily arises due to the exertion of pressure resulting from the progressive enlargement of the cyst, which occurs several years after the initial infection [1]. The renal hydatid cyst is the third most frequently encountered location, following the liver and lungs. All combined strategies to treat renal hydatids include medical treatment with albendazole, pericystectomy, and simple nephrectomy.
Case report
A 71-year-old male presented to the Department of General Surgery at Mahatma Gandhi Institute of Medical Sciences with a complaint of right-sided abdominal pain experiencing for the previous four to five months. However, the patient had never before experienced such severe pain, nausea, vomiting, difficulty urinating, or a rise in body temperature. Haematuria was also absent, and patients' medical and surgical backgrounds were insignificant.
The results of the physical examination were within normal limits. During an abdominal examination, a cystic, non-tender mass of around 20 × 10 cm extending to the right iliac crest was observed on the patient's right flank. The results of the digital rectal exam and the other systemic examination were normal. A prominent mass lesion was found in the right hypochondriac area and right iliac fossa region during the ultrasound evaluation of the abdomen and pelvis. The mass lesion also featured several cystic regions. Normal values were found for the complete blood count, the renal function test, and the liver function test. Focal calcified ruptured hydatid cysts were found in the right half of the abdomen, as shown on the contrast computed tomography (CT) scan of the abdomen and pelvis (Figure 1). The lesion was compressing and displacing the liver, gall bladder, right kidney, right ureter and IVC anterosuperiorly, pancreas, celiac trunk and abdominal aorta medially and surrounding small and large bowel loops peripherally. The right kidney was dilated, and the right cortex was thinner than normal because of the compression. The left kidney, liver, and lungs showed no signs of a similar lesion.
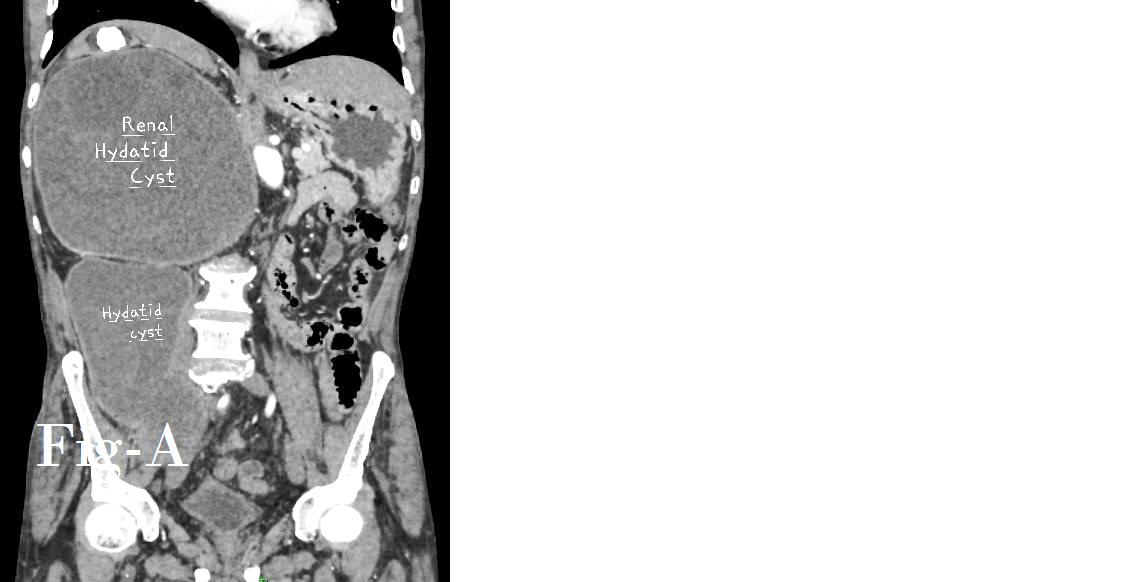
Figure 1a: CECT images in coronal section.
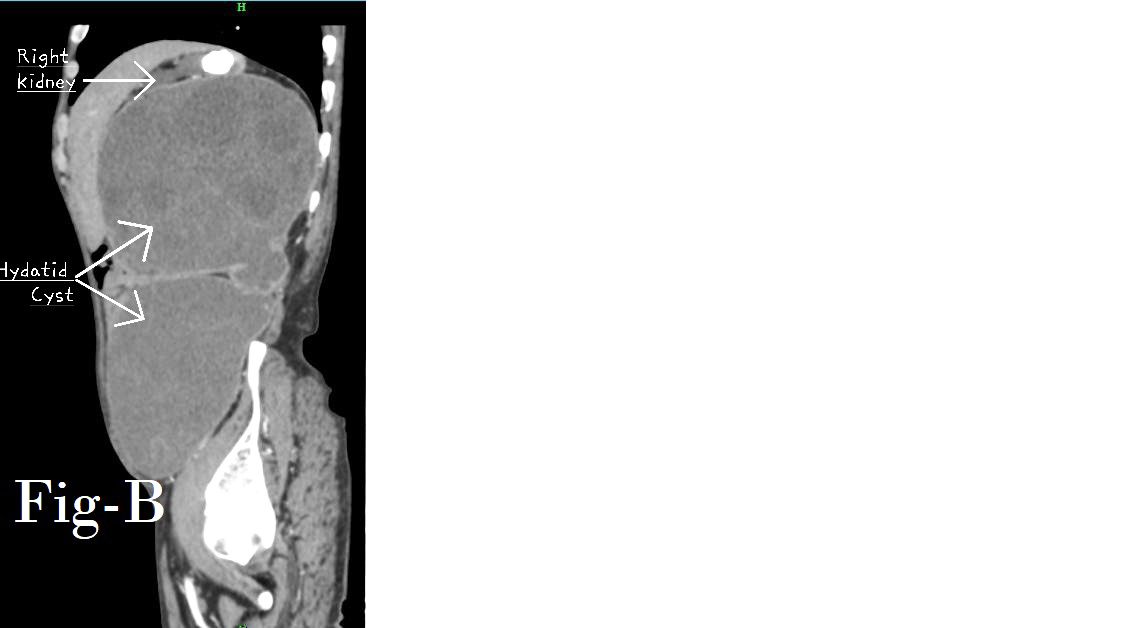
Figure 1b: CECT images in sagittal section showing kidney displaced cephalad by hydatid cyst.
The risk of rupture from such a huge cyst led to the decision to proceed with surgical intervention. Before surgery, the patient received albendazole for two weeks. Since the DTPA scan indicated that the right kidney was nonfunctional, an open right nephrectomy was planned. On exploration, a large cystic structure was found in the right iliac area, while another was found in the right hypochondriac area. The incision was made, and the cyst's contents were drained. A scolicidal agent consisting of 20% hypertonic saline solution was used to prevent the spillage of contents. A partial cystectomy was done. After the cyst was drained, the right kidney could be visualised. In particular, the right kidney's upper pole was firm, and the cyst wall stuck tenaciously to the organ. The decision to perform a simple nephrectomy was taken. The right hypochondrium and pelvic drain were inserted. The postoperative period was uneventful. The patient took albendazole for four weeks postoperatively. The diagnosis of hydatid cyst disease was confirmed by histopathology. Imaging performed at 6-month and 1-year intervals after surgery showed no evidence of a recurrence.
Contrast enhanced computed tomography (CECT) shows, focally calcified cystic lesion with a multiloculated cyst within, giving a honeycomb appearance of size 20.1 x 16.6 x 14.6 cm, volume 2547 ml seen in the right hypochondriac and right lumbar region (Figure 2). Cystic lesion of approximately 16.2 x 12.6 x 12.5 cm, volume 1334 ml, in the right lumbar and right iliac fossa region along the right iliopsoas muscle, showing a linear serpentine membrane. Both cystic lesions were communicating with each other.
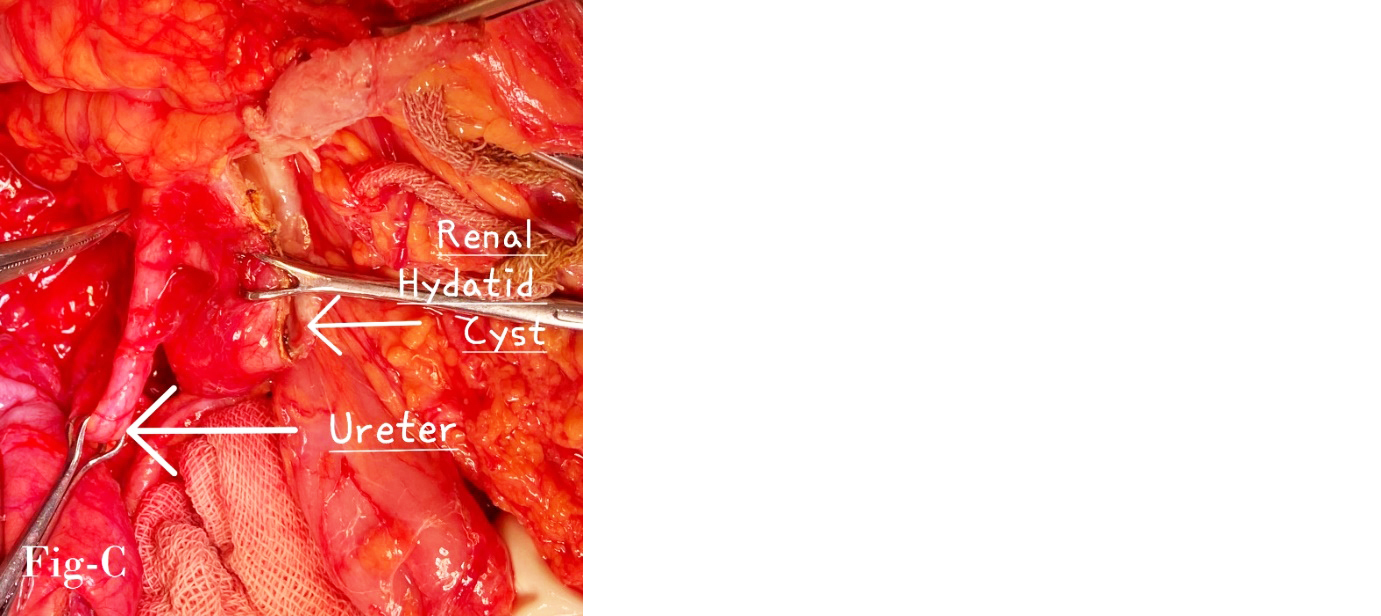
Figure 2: Intraoperative picture showing renal hydatid cyst.
Discussion
The hydatid cyst is a cystic structure that develops in different organs due to the formation of oncospores from the Echinococcus tapeworm within the organ. Oncospores undergo egg maturation and subsequently develop into hydatid cysts, representing the infective stage, among intermediate hosts, including humans. The transmission of infection occurs when individuals ingest eggs present on contaminated vegetables or unprotected food items or when they inhale dust particles containing eggs. Following ingestion by the intermediate host, the oncospores infiltrate the gastrointestinal wall and then enter the bloodstream via the portal circulation, leading to its migration to the liver. Alternatively, it may travel through the lymphatic system to the lungs, the most frequently encountered sites for the development of hydatid cysts. However, in certain instances, the oncospores may evade this typical route and disseminate throughout the systemic circulation, ultimately establishing themselves in other organs, such as the kidney [1].
The incidence of renal involvement in total hydatid disease is reported to be 2-3%, which is significantly lower when compared to the involvement of the liver and lungs. The occurrence of isolated renal hydatid disease is exceptionally rare [2].
The field of radiology holds considerable importance in the process of diagnosing and assessing the progression of disease. Plain radiographs have the potential to detect a circular calcification in the vicinity of the impacted kidney. Ultrasound exhibits greater sensitivity due to its ability to provide a more comprehensive assessment of the mass, encompassing a more precise estimation of its dimensions, surface characteristics, the existence of daughter cysts, and other concomitant regional abnormalities. In contrast, the CT scan is considered a more precise diagnostic modality due to its ability to precisely determine the dimensions and location of the lesion, as well as its relationship with adjacent tissue. This can be especially advantageous during the preoperative planning stage when surgical intervention is being considered, as it allows for a comprehensive assessment of the renal hydatid cyst [3].
Renal hydatid cysts can remain asymptomatic for extended periods with no discernible clinical manifestations. The delay in diagnosis due to the absence of symptoms results in irreversible harm to the affected organs, potentially leading to organ loss in unfortunate cases. Diagnosing hydatid cysts in the kidney requires a combination of diagnostic methods, including clinical history, serological analysis, urine analysis, and radiological imaging. These methods collectively confirm the presence of the disease by detecting the hydatid cyst, its layers, or the protoscolex.
A combination of medical and surgical intervention is required to address renal hydatid cysts. The PAIR (puncture-aspiration-injection-re-aspiration) technique has proven an effective therapeutic method for renal hydatid cysts. However, in cases where the cysts exceed 6 cm in size, inserting a subcutaneous drain and evacuating the cyst contents multiple times is necessary. This precaution is taken to reduce the risk of infection, as the fluid within the hydatid cyst contains protoscolices. The choice of treatment modality is contingent upon the specific characteristics and dimensions of the cyst. Additionally, providing a scolicidal agent before the surgical procedure is necessary to mitigate the potential for infection [4].
Conclusion
This study suggests that a combination of techniques, including clinical history, urine analysis, and radiological imaging, may be necessary to identify a renal hydatid cyst. It is necessary to administer scolicidal medications before surgery for effectively remove a cyst. The optimal therapeutic approach involves surgical intervention for the removal of a hydatid cyst located in the kidney while ensuring minimal risk of cyst rupture.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Basnet P, Chapagain S, Neupane R, Thapa A. Rare encounter of renal hydatid cyst: A case report. J Nepal Med Assoc. 2021; 59:716–718.
[2] Parajuli P, Pradhan MM, Chapagain S, Luitel BR, Chalise PR et al. Isolated renal hydatid cyst: A rare case report. Urol Case Rep. 2021; 35:101525.
[3] Taei THA, Mail SAA, Thinayyan AHA, Alsetrawi A. Renal hydatid cyst: A case report. Radiol Case Rep. 2022; 17:2063–2066.
[4] Reza HAM, Rreza G, Nastaran B, Mousa MH. Renal hydatid cyst: A rare infectious disease. Oxf Med Case Rep. 2019; 2019:114–116.