Full Text
Introduction
Spinal deformity is defined as an abnormal curvature of the spine. Scoliosis represents an abnormal curvature in the coronal plane, kyphosis refers to abnormality in the sagittal plane, and a combination of both is termed kyphoscoliosis [1].
Scoliosis is broadly classified into two types: compensatory (non-structural) and structural. In compensatory scoliosis, the primary abnormality lies outside the spine, such as hip contractures or limb length discrepancies that lead to a secondary spinal curvature. In contrast, structural scoliosis arises from intrinsic abnormalities of the vertebral column. The etiologies of structural scoliosis include idiopathic, congenital, neuromuscular, and syndromic causes such as Marfan syndrome and neurofibromatosis [1].
Idiopathic scoliosis is the most common type, accounting for nearly 80% of all cases. The majority are mild, with Cobb’s angle <10–20°, and often require no active treatment. While minor curves (<10°) occur equally in males and females, progressive curves requiring intervention are more frequent in females, with a female-to-male ratio of approximately 7:1 [2]. Clinically, affected children may present with spinal deformity, asymmetry of body parts (uneven shoulders, pelvic tilt, or limb length discrepancy), or back pain. The earliest clinical sign is often posterior chest wall asymmetry, best appreciated during the forward-bend test. Other findings include shoulder or breast level asymmetry and unilateral pelvic prominence. A thorough neurological examination is essential to exclude conditions such as tethered cord or other spinal anomalies. Additionally, careful examination for cutaneous markers including café-au-lait spots, sacral dimples, hair tufts, or hemangiomas is crucial [1,2].
Diagnosis is based on radiographic evaluation of the spine in posteroanterior (PA) and lateral views, with Cobb’s angle used to quantify the degree of curvature. Magnetic resonance imaging (MRI) of the spine is indicated when neurological involvement or an underlying intraspinal abnormality is suspected [1,2].
Management primarily aims to prevent progression of the deformity. Bracing (for skeletally immature patients with deformity <45°), serial body casting, and surgical correction (with or without implants) constitute the main treatment options, tailored according to the underlying etiology [1,2].
This case series presents three children with scoliosis of different etiologies, highlighting their clinical presentations, imaging findings, and management strategies. The purpose of this report is to emphasize the need for improved awareness among pediatricians and to address the challenges faced by orthopedicians in treating skeletally immature patients. A multidisciplinary approach involving pediatricians, orthopedicians, physiotherapists, and nutritionists is recommended to optimize patient care.
Case presentations
Case 1:
A 15-year-old child presented with back pain for the past one year, which had worsened over the preceding one and a half months. The pain was localized mainly to the left lower back and was aggravated by sitting and lying supine. The child had a gradually progressive scoliosis of the lumbosacral spine since birth. On examination, there was a prominent left buttock with left-sided lumbar scoliosis. No dysmorphic or syndromic features were noted, and there was no involvement of other bones or joints. Investigations ruled out tuberculosis and ankylosing spondylitis.
Computed tomography (CT) of the lumbosacral spine revealed levoscoliosis at the L3–L4 level with a Cobb’s angle of 52°, along with reduced intervertebral disc spaces, consistent with a diagnosis of idiopathic scoliosis (Figure 1). The child underwent surgical correction with corrective osteotomy and placement of cobalt–chrome rods and pedicle screws between L3–L4 and S1–S2 under image intensifier (IITV) guidance. Wound closure was performed with drain placement, and one unit of packed red blood cells (PRBC) was transfused intraoperatively. The postoperative period was uneventful, and the child recovered well.
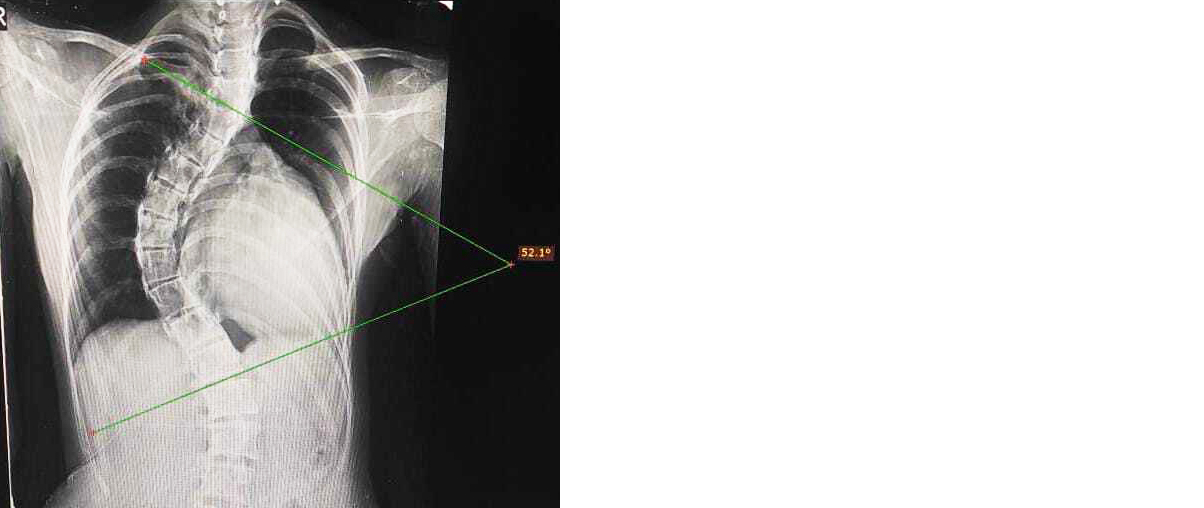
Figure 1: Chest X-ray (PA view) showing scoliosis with measurement of Cobb’s angle.
Case 2:
A 12-year-old girl with dysmorphic features presented with a history of back pain for the past one month. On examination, she had abnormal facies, a webbed neck, deformed left pinna, low-set ears, a low hairline, scoliosis, and short stature (height 123 cm, <3rd centile, below target mid-parental height; weight 22 kg, <3rd centile). The upper-to-lower segment ratio was 1:1. Pubertal maturation was delayed (Sexual Maturity Rating [SMR] stage 2). Magnetic resonance imaging (MRI) of the lumbosacral spine revealed a hemivertebra at the L4–L5 level with partial vertebral fusion (Figures 1). Thyroid function and echocardiography were normal, while serum vitamin D level was found to be insufficient.
Based on the clinical findings and imaging results, a diagnosis of Klippel–Feil syndrome with syndromic scoliosis was made. Karyotyping demonstrated a normal female karyotype, thereby ruling out Turner syndrome. The child was managed conservatively with vitamin D and calcium supplementation, nutritional support, and spinal bracing. She was advised regular follow-up in the orthopedic clinic for ongoing evaluation and further management.
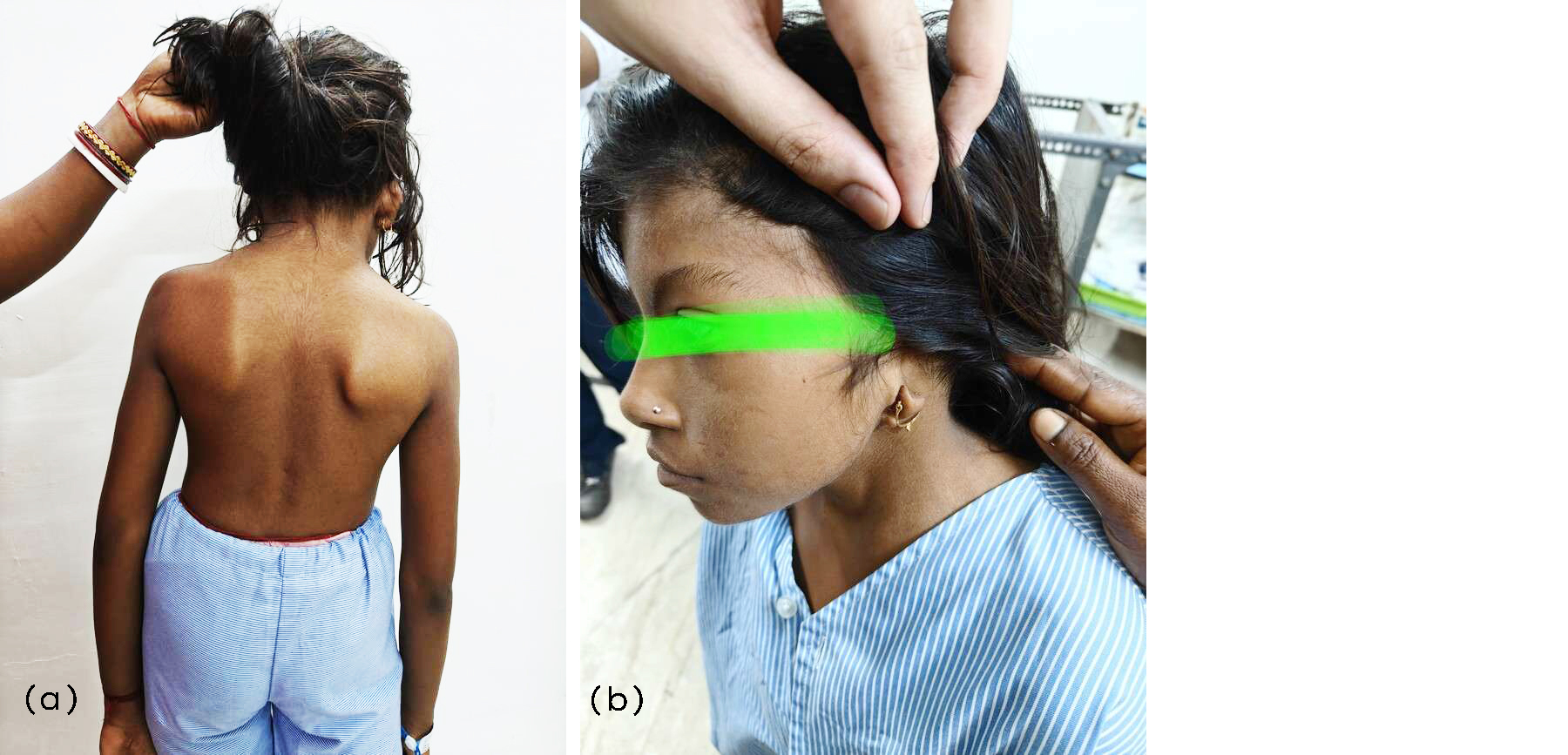
Figure 2: (a) Skeletal deformities showing scoliosis, short neck, abnormal shoulder and scapular orientation, and low hairline, (b) Deformed ear.
Case 3:
A 10-year-old female presented with back pain for the past three months, along with a history of multiple hyperpigmented skin lesions since childhood and gradually progressive spinal deformity (scoliosis). On examination, she had more than six café-au-lait macules (>5 mm) distributed over the body, along with axillary and inguinal freckling. Ophthalmological evaluation revealed iris Lisch nodules (Figure 3).
Magnetic resonance imaging (MRI) of the lumbosacral spine demonstrated a left-sided plexiform neurofibroma and mild lumbar scoliosis with left convexity, in addition to dorsal scoliosis with right convexity. Based on these findings, a diagnosis of Neurofibromatosis type 1 with scoliosis was established. There were no renal abnormalities, and blood pressure was within normal limits. The child underwent surgical excision of the neurofibroma and is currently under follow-up for hypertension screening, seizure monitoring, and regular ophthalmology and ENT evaluations.

Figure 3: Multiple café-au-lait spots and spinal plexiform neurofibroma.
Discussion
Scoliosis is a common condition in children, affecting approximately 2–3% of all teenagers [3]. The standard method for measuring spinal curvature in scoliosis is Cobb’s angle, calculated as the angle between lines drawn along the upper border of the most tilted vertebra above the curve’s apex and the lower border of the most tilted vertebra below the apex [4].
In our case series, idiopathic scoliosis was observed in a female patient. Literature suggests that early-onset idiopathic scoliosis is more common in males, whereas late-onset idiopathic scoliosis occurs more frequently in females [5]. Common causes of structural scoliosis include idiopathic scoliosis, poliomyelitis, congenital vertebral abnormalities, and neurofibromatosis. In this series, we report one case each of idiopathic scoliosis, neurofibromatosis type 1, and a genetic variant (Klippel–Feil syndrome) [6].
Congenital scoliosis arises from abnormalities in vertebral formation, fusion, or segmentation, though the exact pathophysiology remains hypothetical. Neuromuscular and genetic scoliosis are usually caused by unequal pull of abnormal muscles or nerves [2,7].
The predominant symptoms in this series were back pain and structural deformities, such as spinal curvature and asymmetrical shoulder height, along with disease-specific features, including neurofibroma and failure to thrive. Literature indicates that skeletal deformities and back pain are the most common reasons for medical consultation in scoliosis [1,2,8]. Pulmonary complications, such as restrictive lung disease, pes cavus, and hip dysplasia, were not observed in any of our cases.
Diagnosis of scoliosis is primarily based on spinal radiographs and Cobb’s angle measurement. Additional investigations are performed on a case-by-case basis for example, MRI of the spine in neurofibromatosis type 1 and karyotyping in Klippel–Feil syndrome [1,2,9,10].
Treatment depends on the underlying cause, skeletal maturity, curve progression, degree of curvature, time of presentation, and associated symptoms. In our first case of idiopathic scoliosis, progressive curvature since childhood with a large Cobb’s angle of 55° and associated low back pain warranted surgical correction. In the third case, scoliosis was caused by a plexiform neurofibroma, which required surgical excision. The second case, associated with vitamin D deficiency, failure to thrive, and delayed puberty, had uncertain skeletal maturity; therefore, conservative management with calcium and vitamin D supplementation along with spinal bracing was initiated, with final treatment decisions planned after follow-up [11].
Overall management of scoliosis includes thorough history-taking, clinical examination, adolescent screening, and surgical correction when indicated. Screening is recommended for adolescent girls at 10 and 13 years of age, and for boys at 14 years. Exercises and bracing are advised for those with Cobb’s angle <10° (below 10 years) or <20° (above 10 years). Surgical options include pedicle screw fixation, vertebral body tethering, vertebral body stapling, and magnetically controlled growing rods. The primary goals of surgery are to correct deformity, reduce curvature, and address rotational abnormalities [11, 12].
Conclusion
Scoliosis is a common and clinically significant condition in growing children. Curvatures exceeding 10° are considered abnormal and warrant careful evaluation, particularly if progressive, as they may lead to pain, functional limitations, and long-term complications. Early detection through routine screening during growth periods is essential, enabling timely intervention and appropriate management. Pediatricians play a critical role in recognizing early signs, coordinating multidisciplinary care, and ensuring referral to orthopedic specialists when indicated. Prompt assessment and individualized treatment strategies can improve functional outcomes and quality of life in affected children.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Menon PSN, Ramji S, Lodha R, Gupta P. PG Textbook of Pediatrics: Systemic Disorders and Social Pediatrics. Vol 3. New Delhi: Jaypee Brothers Medical Publishers; 2015.
[2] Kliegman RM, St Geme JW. Nelson Textbook of Pediatrics. 21st ed. Philadelphia: Elsevier; 2024.
[3] Marinov D, Dimitrova T. A case–control study on body composition of teenagers with adolescent idiopathic scoliosis. Eur J Public Health. 2021; 31:165–505.
[4] Napierkowski DB. Scoliosis: a case study in an adolescent boy. Orthop Nurs. 2007; 26:147–155.
[5] Gummerson NW, Millner PA. Scoliosis in children and teenagers (II). Orthop Trauma. 2011; 25:403–412.
[6] James JI. Scoliosis in children. Br J Radiol. 1954; 27:511–523.
[7] James JI. The etiology of scoliosis. J Bone Joint Surg Br. 1970; 52:410–419.
[8] Achar S, Yamanaka J. Back pain in children and adolescents. Am Fam Physician. 2020; 102:19–28.
[9] Calloni SF, Huisman TA, Poretti A, Soares BP. Back pain and scoliosis in children: when to image, what to consider. Neuroradiol J. 2017; 30:393–404.
[10] Ng SY, Bettany–Saltikov J. Imaging in the diagnosis and monitoring of children with idiopathic scoliosis. Open Orthop J. 2017;11:1500–1511.
[11] Janicki JA, Alman B. Scoliosis: review of diagnosis and treatment. Paediatr Child Health. 2007; 12:771–776.
[12] Cheung ZB, Selverian S, Cho BH, Ball CJ, Cho SK. Idiopathic scoliosis in children and adolescents: emerging techniques in surgical treatment. World Neurosurg. 2019; 130:737–742.