Orginal Research
2024
September
Volume : 12
Issue : 3
Vaccination awareness in adult patients at a tertiary care hospital
Kanugula S, Kanakabhushanam GVVS, Sony A, Gomasa M
Pdf Page Numbers :- 207-212
Shivaraju Kanugula1,*, Kanakabhushanam GVVS2, Avirendla Sony1, and Mahesh Gomasa1
1Department of General Medicine, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India
2Department of Obstetrics and Gynaecology, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India
*Corresponding author: Dr. Shivaraju Kanugula, Department of General Medicine, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India. Email: shivaraju.doctor@gmail.com
Received 8 May 2024; Revised 19 June 2024; Accepted 24 June 2024; Published 30 June 2024
Citation: Kanugula S, Kanakabhushanam GVVS, Sony A, Gomasa M. Vaccination awareness in adult patients at a tertiary care hospital. J Med Sci Res. 2024; 12(3):207-212. DOI: http://dx.doi.org/10.17727/JMSR.2024/12-39
Copyright: © 2024 Kanugula S et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: As global birth rates decline and life expectancies rise, the geriatric population is rapidly increasing. The growing geriatric population worldwide necessitates improved vaccination awareness among older adults to mitigate the increased risk of infectious diseases due to immunosenescence - the gradual deterioration of the immune system with age. The main objective of our study was to create awareness, explain the benefits of adult vaccination and brief about the CDC recommended vaccinations and their schedules.
Methods: This is a cross-sectional observational study conducted for 3 months on outpatient basis through a pamphlet survey in around 150 patients.
Results: 64.6% of patients completed their Signal-to-Noise Ratio (SNR). Secondary level education and out of them 49.3% of them residing in urban areas doesn’t know about adult vaccination.
Conclusion: Findings reveal that patients' decisions are influenced by sociocultural factors, access to information, and misconceptions. The results highlight the importance of targeted immunization programs for older adults and implementing National guidelines in a country like India with highest population can prevent vaccine-preventable diseases, reduce healthcare costs, and improve public health outcomes. Enhanced education and healthcare provider engagement are recommended to address vaccine hesitancy and improve vaccination rates among the elderly, especially in underprivileged communities.
Keywords: adult vaccination; awareness; immunosenescence
Full Text
Introduction
Globally declining birth rates and rising life expectancies are contributing to the fast growing geriatric population. The Ministry of Health and Family Welfare Technical Group on Population Projection of 2019 findings indicate that the number of people aged ≥50 is predicted to more than double from 193 million in 2011 to 404 million in 2036 as shown in (Figure 1) [1].
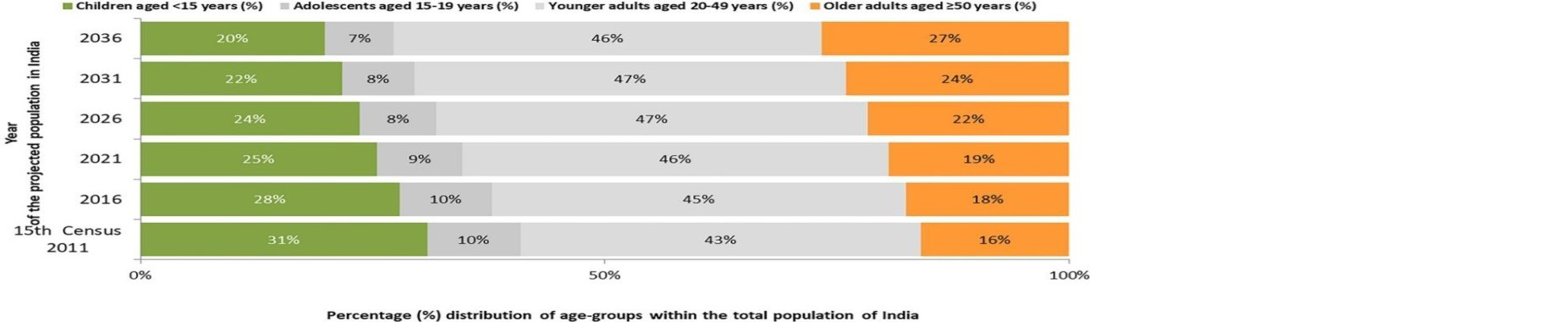
Figure 1: Distribution of age-groups within the total population of India.
Illustrates the projected distribution of India's population by age group from 2011 to 2036. It divides the population into four categories: children under 15, adolescents aged 15-19, younger adults aged 20-49, and older adults aged 50 and above. Over time, the percentage of children and adolescents is steadily declining, from 31% in 2011 to 20% for children and from 10% to 7% for adolescents by 2036. Conversely, the proportion of older adults (aged 50 and above) is increasing, from 16% in 2011 to a projected 27% in 2036, while the younger adult population remains relatively stable around 45-47%. This suggests a significant aging of India's population over the coming decades.
As a result, by 2036, older person’s ≥50 years old will make up 27% of India's overall population. It is estimated that by 2050, there will be 2 billion older individuals worldwide, accounting for more than 20% of the total population. This is a threefold increase from the current estimate [2]. The greater incidence of infectious diseases in older adults compared to younger people is indicative of the clinical significance of immunosenescence.
Numerous biological processes, such as slow changes in immune system cell at levels, lead to immune system remodeling and modifications as we age. Some of these changes result in immunosenescence, which is a decline in immune system activities [3]. Increased vulnerability to infectious, neurological, cardiovascular, and autoimmune disorders has been linked to immunosenescence [4].
Older adults are more susceptible to infectious diseases and have weaker vaccine responses due to a decline in all these humoral and cellular immune system processes and the development of a relative immunological deficit [5]. This age group has a higher rate of comorbidities, making them the demographic most in need of preventative healthcare [6, 7].
Pneumococcal and influenza-related deaths have a significant rise in risk after age 65. The elderly are 10–30 times more likely than younger people to experience respiratory failure from influenza [8, 9]. Research indicates that the United States spends between 9-26 million dollars annually on diseases that can be prevented by vaccination. Of this amount, 80% is devoted to treating individuals who have not received a vaccination [10].
As a result, infectious diseases remain a serious global public health issue [11, 12] and numerous thousands of individuals globally have been diagnosed with vaccine-preventable illnesses (VPDs), which lead to elevated rates of morbidity, mortality, and financial difficulties [13]. The significant burden of sickness, disability, and death among older individuals in India as a result of infectious diseases was brought to light in 2009 by the Association of Physicians in India [14]. According to the association, immunization is the best and most economical approach to prevent and manage infectious illnesses in adults. Therefore, it is necessary to identify vulnerable groups and design immunization regimens specifically for older adults.
In addition, unvaccinated people have the potential to transmit infections, such as pertussis, to infants who are not vaccinated [15, 16]. Vaccination is regarded as one of the most economical public health initiatives in the world [17]. Research indicates that vaccination can prevent complications for older persons with chronic diseases and significantly lower the incidence of hospitalizations [18], admissions to cardiac and critical care units, as well as death [19].
Patients' decisions regarding vaccinations are believed to be influenced by a variety of factors, such as sociocultural influences, awareness, access to accurate information, and misconceptions. Patients' vaccine reluctance may be made worse by doctors' unfavorable views, their lack of vaccination expertise, or their disregard for preventive healthcare practices [20].
Obtaining vaccinations, reaching remote and nomadic communities, and vaccine hesitancy due to false information are notable additional obstacles [21], consequently, raising the adult immunization rate may benefit people as individuals, as families, and as a community. Additionally, adult immunization could lower healthcare expenses [22]. It is especially crucial in communities who are underprivileged. Numerous analyses have emphasized the need of increasing coverage and the fact that adult vaccination rates are low in India [23-25].
The objectives of this study was to raise awareness about adult immunizations, find out the average number of patients had awareness, explain the importance of adult vaccination, and provide brief information on CDC-recommended vaccinations and their schedules.
Materials and methods
The study was a cross-sectional observational study, conducted through a survey using a pamphlet that contained a questionnaire with multiple-choice answers for each question. This survey was distributed to all patients who visited our hospital between February 2024 to April 2024. The questionnaire consisted of 10 questions, all related to the awareness of adult vaccination. The study targeted participants aged 50 years and older, encompassing individuals from diverse educational backgrounds classified by International Standard Classification of Education (ISCED) -2011 [26], residential areas, and occupations. A total of 150 participants were included in the study. Prior to the initiation of the survey, informed consent was obtained from each participant. They were assured of the confidentiality of their data, and the objectives and purpose of the study were clearly explained to them.
Results
Total of 150 participants of age above 50 years were included in the study out of which <60 years of age were 70 (46.7%), ≥ 60 years were 80 (53.3%) and Mean age was 62.39 with SD of (8.68). Most of them were females participants (54.7%) while males were (45.3%) (Table 1).
Table 1: Sociodemographic details of the participants (n= 150).
|
Variables
|
Frequency
|
Percentage
|
|
Age
|
<60 years
|
70
|
46.7
|
|
≥60 years
|
80
|
53.3
|
|
Mean age (SD)
|
62.39 (8.68)
|
|
|
Gender
|
Female
|
82
|
54.7
|
|
Male
|
68
|
45.3
|
People from rural areas covered 76 (50.7%) while people living in urban were (49.3%). Of which (31.3%) of them studied till Signal-to-Noise Ratio (SNR). Secondary, (25.3%) completed Middle schooling and only (1.3%) of them were able to complete their Pre-primary (Figure 2). The participants who were settled as homemakers were found to be (48.0%), and (8.7%) were involved in business (Figure 3 & Table 2).
Table 2: Residence, education & occupation details of the participants (n= 150).
|
Variables
|
Frequency
|
Percentage
|
|
Residence
|
| |
Rural
|
76
|
50.7
|
| |
Urban
|
74
|
49.3
|
|
Education
|
| |
Level – 1 (Pre-Primary/Play school)
|
2
|
1.3
|
| |
Level – 2 (Primary school)
|
10
|
6.7
|
| |
Level – 3 (Middle scool)
|
38
|
25.3
|
| |
Level – 5 (SNR. secondary school)
|
47
|
31.3
|
|
|
Level – 6 (Bachelor’s)
|
40
|
26.7
|
|
|
Level – 7 (Master’s)
|
13
|
8.7
|
|
Occupation
|
| |
Business
|
13
|
8.7
|
| |
Employee
|
22
|
14.7
|
| |
Home maker
|
72
|
48
|
| |
Retired employee
|
43
|
28.7
|

Figure 2: Level of education.
Represents different levels of education, divided into percentages, which are Level 1 (pre-primary school -no schooling) represents 26.7%; Level 2 (primary school) is the smallest, at 8.7%. and level 6 bachelors, level 7 masters and level 8 doctorates are 0%; Level 3 (middle school 6-8th standard) follows closely, accounting for 25.3%. Level 5 (senior secondary school 11-12th standard) is the largest segment, representing 31.3%.

Figure 3: Occupation level of the participants.
48% of are home makers, 28.7% are retired employees, 14.7% are employees and 8.7% are own business.
When asked the participants whether they knew about adult vaccination only 39 (26%) of them said yes and others replied that they don’t know or were not aware of it and of the known, only 2.7% of them have taken the vaccine. 96% of them told that they knew vaccines is cost effective and reduce infections that are prevented by vaccinations. Only 10 (6.7%) of them said that they were not aware of the fact that the infections can be prevented by the vaccines. 53% of them were not aware about the most recommended vaccines by health care providers whereas 38.5% of them gave the answer as Pneumovax (Figure 4). Participants presented with diabetes (58%) which is the highest followed by hypertension (28.6%), and (0.6%) were without any ailments. After explaining them all the advantages of Adult vaccination, (98.7%) said that they will suggest to their family members (Figure 5 & Table 3).
Table 3: Awareness about adult vaccination (n= 150).
|
Questionnaire
|
Yes Freq. (%)
|
No Freq. (%)
|
|
Do you know about adult vaccination?
|
39 (26)
|
111 (74)
|
|
Are you willing are to get Vaccine?
|
114 (76)
|
36 (24)
|
|
Have you taken any Vaccine before?
|
31 (20.7)
|
119 (79.3)
|
|
Do you know that taking vaccination can prevent severity of infection?
|
145 (96.7)
|
5 (3.3)
|
|
Do you agree that the vaccine is cost effective and reduce infections?
|
144 (96)
|
6 (4)
|
|
Do you know about infections that are prevented by vaccination?
|
140 (93.3)
|
10 (6.7)
|
|
Are you afraid of vaccine side-effects?
|
73 (48.7)
|
77 (51.3)
|
|
Do you suggest your family members to take vaccine?
|
148 (98.7)
|
2 (1.3)
|
|
Questionnaire
|
Answer’s Freq. (%)
|
|
How many vaccines you can name that are commonly
recommended for adults by healthcare authorities?
For example, are you able to name three, two, or
even just one of these vaccines?
|
Influvac tetra
|
57 (38.5)
|
|
Pneumovax
|
11 (7.4)
|
|
Tdap
|
2 (1.1)
|
|
Not aware
|
80 (53)
|
|
Do you suffer from hypertension (HTN), diabetes
(DM), asthma, thyroid issues, or other diseases?
Or No comorbidities
|
Diabetes
|
87 (58)
|
|
Hypertension
|
43 (28.6)
|
|
Thyroid
|
12 (8)
|
|
Asthma
|
7 (4.7)
|
|
No comorbidities
|
1 (0.6)
|

Figure 4: Can you name at least three vaccines most recommended for adults by healthcare authorities?
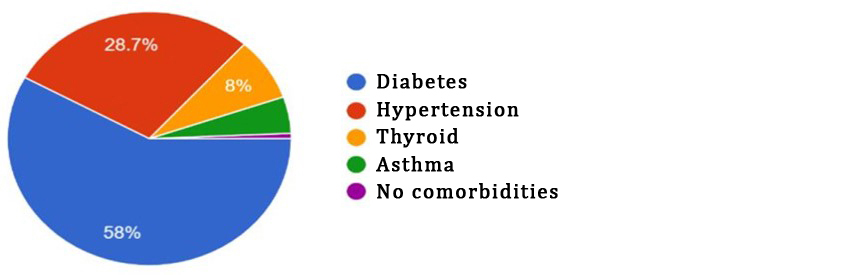
Figure 5: Do you suffer with any disease?
Table 4: Awareness level among socio-demographic variables.
|
Socio-demographic variables
|
Awareness level
|
Total
|
P value
|
|
Good (n=97)
No. (%)
|
Poor (n=53)
No. (%)
|
|
Age
|
0.144
|
| |
<60
|
41 (58.6)
|
29 (41.4)
|
70
|
|
| |
≥60
|
56 (70)
|
24 (30.0)
|
80
|
|
|
Gender
|
0.725
|
| |
Female
|
52 (63.4)
|
30 (36.6)
|
82
|
|
| |
Male
|
45 (66.2)
|
23 (33.8)
|
68
|
|
|
Occupation
|
0.942
|
| |
Business
|
9 (69.2)
|
4 (30.8)
|
13
|
|
| |
Employee
|
15 (68.2)
|
7 (31.8)
|
22
|
|
| |
Home maker
|
45 (62.5)
|
27 (37.5)
|
72
|
|
| |
Retired employee
|
28 (65.1)
|
15 (34.9)
|
43
|
|
|
Residence
|
0.157
|
| |
Rural
|
45 (59.2)
|
31 (40.8)
|
76
|
|
| |
Urban
|
52 (70.3)
|
22 (29.7)
|
74
|
|
This shows that the Female population (n=53) has more awareness than males (n=45), and people residing in urban regions n=52 (70.3%) have more knowledge about the vaccination than the people residing in rural areas n=45 (59.2%).
Discussions
In this study we found that most of participants were aware of the benefits of the vaccination (96%) but doesn’t know about adult vaccination (26%) which is due to the lack of awareness. A survey conducted proved that >80% of adults were lacking awareness about adult vaccination [25]. Over two-thirds of Indian adults are unaware of adult immunization, and many still believe that vaccines are intended for children [27]. The existing gap in adult vaccine coverage is ascribed to a lack of awareness and understanding about the benefits of immunization, doubts regarding costs and benefits, low vaccine effectiveness in the elderly, accessibility, and inconsistent recommendations by healthcare practitioners [28]. Establishing specialized adult vaccination facilities for adults, the elderly, adolescents, pregnant women, travelers, people with chronic health issues, and healthcare professionals is vital for raising awareness about the importance of adult vaccination. To close the gap between projected and actual adult immunization rates, consider non-traditional vaccination delivery facilities with walk-in services and extended hours [29]. Though 35.4% of the participants completed their graduation but due to lack of awareness only 2.7% of them have taken vaccination. 58% of them suffering with diabetes, 28.6% with Hypertension while only 0.6% were having no comorbidities, which is a very negligible. Vaccination, a crucial public health policy, received lower attention in our clinical practice. Regarding the safety concerns, there is a significant result of 89% of patients are worried about the safety of vaccination, probably the concerned treating physician and other healthcare personnel should take extra time in explaining the safety, benefits of vaccination and the cost effectiveness.
The limitations of our study are that the sample size should need huge number of participants for better and adequate conclusion and the post vaccination side effects were not studied in this survey.
Conclusions
Many countries like US, Australia and UK had adopted life course immunization for geriatric population, as adult vaccination is an important contributor to healthy living. However. Creating awareness and boosting adult vaccination in India not only reduces burden of the hospital admissions but also decrease mortality rates while enhancing quality of life. Recognizing the urgent need for collaboration, the Association of physicians of India brought Conducting creating unified immunization guidance for India, with a focus on an adult immunization and future vaccines [30].
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Census of India 2011. Population projections for India and States 2011-2036. Report of the technical group on population projections, November 2019. National Commission on Population. Ministry of Health and Family Welfare, Government of India. Available from: https://nhm.gov.in/New_Updates_2018/Report_Population_Projection_2019.pdf.
[2] Ellen ME, Panisset U, de Carvalho IA, Goodwin J, Beard J. A knowledge translation framework on ageing and health. Health Policy. 2017; 121:282–291.
[3] Fulop T, Dupuis G, Witkowski JM, Larbi A. The role of immunosenescence in the development of age-related diseases. Rev Invest Clin. 2016; 68:84–91. [4] Xu W, Wong G, Hwang YY, Larbi A. The untwining of immunosenescence and aging. Semin Immunopathol. 2020; 42:559–572.
[5] Crooke SN, Ovsyannikova IG, Poland GA, Kennedy RB. Immunosenescence and human vaccine immune responses. Immun Ageing. 2019; 16:25.
[6] World Health Organization. Proposed working defnition of an older person in Africa for the MDS Project. Available from: https://www.who.int/healthinfo/survey/ageingdefnolder/en.
[7] Esposito S, Principi N, Rezza G, Bonanni P, Gavazzi G, et al. Vaccination of 50+ adults to promote healthy ageing in Europe: the way forward. Vaccine. 2018; 36:5819–24.
[8] Smetana J, Chlibek R, Shaw J, Splino M, Prymula R. Influenza vaccination in the elderly. Hum Vaccin Immunother. 2018; 14:540–549. [9] Gatwood J, Shuvo S, Hohmeier KC. Pneumococcal vaccination in older adults: an initial analysis of social determinants of health and vaccine uptake. Vaccine. 2020; 38:5607–5617.
[10] Ozawa S, Portnoy A, Getaneh H. Modeling the economic burden of adult vaccine- preventable diseases in the United States. Health Aff. 2016; 35:2124–2132.
[11] Fonkwo PN. Pricing infectious disease. The economic and health implications of infectious diseases. EMBO Rep. 2008; 9:S13–17.
[12] Khabbaz RF, Moseley RR, Steiner RJ, Levitt AM, Bell BP. Challenges of infectious diseases in the USA. Lancet. 2014; 384:53–63.
[13] Tan L. Adult vaccination: now is the time to realize an unfulfilled potential. Hum Vaccin Immunother. 2015; 11:2158–66. [14] Mohan A, Sharma SK, Singal RK, Agarwal AK. Adult immunization (monograph). Mumbai: Association of Physicians of India; 2009. Available from: https://www.jaypeedigital.com/book/9788184486735
[15] Dardis MR, Koharchik LS, Dukes S. Using the health belief model to develop educational strategies to improve pertussis vaccination rates among preschool staff. NASN Sch Nurse. 2015; 30:20–25.
[16] Nieves DJ, Heininger U. Bordetella pertussis. Microbiol Spectr. 2016; 4.
[17] Lahariya C, Bhardwaj P. Adult vaccination in India: Status and the way forward. Hum. Vaccines Immunother. 2020; 16:1508–1510.
[18] Sung LC, Chen CI, Fang YA, Lai CH, Hsu YP, et al. Infuenza vaccination reduces hospitalization for acute coronary syndrome in elderly patients with chronic obstructive pulmonary disease: a population-based cohort study. Vaccine. 2014; 32:3843–3849.
[19] Hung IF, Leung AY, Chu DW, Leung D, Cheung T, et al. Prevention of acute myocardial infarction and stroke among elderly persons by dual pneumococcal and influenza vaccination: a prospective cohort study. Clin Infect Dis. 2010; 51:1007-1016.
[20] Ozisik L, Basaran NC, Oz SG, Guven GS, Tanriover MD. Perceptions and attitudes of patients about adult vaccination and their vaccination status: still a long way to go? Med Sci Monit. 2017; 23:3178–3184.
[21] Gurnani V, Haldar P, Aggarwal MK, Das MK, Chauhan A, et al. Improving vaccination coverage in India: lessons from Intensifed Mission Indradhanush, a cross-sectoral systems strengthening strategy. BMJ. 2018; 363:k4782.
[22] Tan L. Adult vaccination: now is the time to realize an unfulfilled potential. Hum Vaccin Immunother. 2015; 11:2158–66.
[23] Mehta B, Chawla S, Kumar V, Jindal H, Bhatt B. Adult immunization: the need to address. Hum Vaccin Immunother. 2014; 10:306–309.
[24] Verma R, Khanna P, Chawla S. Adult immunization in India: importance and recommendations. Hum Vaccin Immunother. 2015; 11:2180–82.
[25] Rathi A, Sharma S. Vaccine preventable diseases in Indian adults - burden & prevention. Infect Dis Diag Treat. 2017; J102.
[26] International Standard Classification of education ISCED 2011. Available from: https://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf
[27] Aggarwal KK. Majority of Indians are unaware of adult vaccinations. Available from: http://blogs.kkaggarwal.com/2017/11/vaccinations
[28] de Gomensoro E, Del Giudice G, Doherty TM. Challenges in adult vaccination. Ann Med. 2018; 50:181–192.
[29] Ghia CJ, Rambhad GS. Developing adult vaccination ecosystem in India: Current perspective and the way forward. Health Serv Res Manag Epidemiol. 2021; 8:23333928211030791.
[30] Mathur G, Vora A. Indian consensus guidelines on adult immunization inauguration of the Indian consensus guidelines on adult immunization by the honorable vice president of India Shri Jagadeep Dhanakar on the 22nd February at APICON 2024, New Delhi.