Full Text
Introduction
Globus pharyngeus, earlier called globus hystericus, is the persistent or intermittent sensation of pain, uncomfortable feeling, or lump or foreign body sensation in the throat. It contributes to approximately 4% of otolaryngology visits [1]. Originally, it was termed as globus hystericus, because no cause was identified in the majority, and it was attributed to psychological factors.
The etiology is varied, and no cause can be identified in 50% of patients. Inflammatory causes include enlarged tonsils and pharyngitis. Other causes include gastroesophageal reflux disease (GERD), esophageal neoplasms, motility disorders, hypertrophy of base of tongue, thyroid disorders, retroverted epiglottis, and heterotopic gastric mucosa in the esophagus [1-3].
Investigation protocol in patients with globus pharyngeus keeps evolving owing to varied potential etiologies. Cervical ultrasonography is a simple, non-invasive tool in the evaluation of globus pharyngeus. It is useful in the identification of thyroid disorders, enlarged nodes, and carotid artery pathologies which are not evident by clinical examination and laryngoscopy. The study was conducted to evaluate the role of cervical ultrasonography as a first-line diagnostic tool in the assessment of patients presenting with globus pharyngeus.
Methods
The study was designed to assess the usefulness of cervical ultrasonography as a first-line tool in evaluating patients with globus pharyngeus. The prospective study was conducted with 50 patients who were referred from an otolaryngologist in 2024 after obtaining Ethics Committee approval. The patients had normal findings on clinical examination and laryngoscopy. Patients with palpable lymph nodes, large goitre, and vocal cord palsy were excluded from the study.
Adult patients with complaints of pain, lump in the throat, discomfort, and foreign body sensation were included in the study. All 50 patients (women, 36; men, 14) had normal findings on clinical examination and laryngoscopy.
Cervical ultrasonography was done with the Mindray DC-8 ultrasonography system with the high frequency linear transducer. Written consent was obtained from all patients.
Serum T3, T4, and TSH, and thyroid antibodies were estimated by the clinician for thyroiditis cases and the results confirmed. Fine needle aspiration cytology (FNAC) of neck nodes were done for thyroid nodules or planned for follow up, as indicated by the TIRADS score. All the neck nodes were examined further by FNAC.
Results
In our study of 50 patients, 28 (56%) showed positive findings on ultrasonography, while 22 (44%) had normal results. The majority of positive cases were related to thyroid disorders, with 16 patients (32%) presenting diffuse thyroid lesions and six patients (12%) showing focal thyroid nodules. Among those with nodules, four were classified as TIRADS 3, one as TIRADS 2 (colloid cyst), and one as TIRADS 4. Other findings included lymphadenopathy in four patients (8%), carotidynia in one patient (2%), and submandibular duct calculus with sialadenitis in another (2%). Of the 50 patients, 28 (56%) had positive findings on ultrasonography and 22 (44%) had normal findings.
Most patients with positive ultrasonography findings had thyroid disorders (Table 1). Sixteen patients had diffuse thyroid lesions and six patients had focal thyroid nodules. Four patients had lymphadenopathy, one patient had carotidynia, and one patient had submandibular duct calculus with sialadenitis. In patients with thyroid nodules, four had TIRADS 3 nodules, one had colloid cyst (TIRADS 2) and one had TIRADS 4 nodule. Sixteen patients had diffuse thyroid lesions (32%) and six patients had focal thyroid nodules (12%). Four patients had lymphadenopathy (8%), one patient had carotidynia (2%), and one patient had submandibular duct calculus with sialadenitis (2%) (Figure 1).
In this study, four patients had lymphadenopathy. One patient had necrotic lymph nodes, which subsequently on FNAC was proved to be metastatic squamous cell carcinoma. Lymph nodes in other patients were diagnosed to be tuberculous nodes.
A middle aged woman had eccentric wall thickening in the left common carotid artery, which was tender, with minimal luminal narrowing, and was subsequently diagnosed as carotidynia.
A 25-yr-old male had a one cm calculus in the left submandibular duct ostium. The submandibular gland was enlarged and hyperaemic, representing sialolithiasis with sialadenitis.
Table 1: Details of cases with positive ultrasound findings.
|
Finding
|
Number of patients with findings
|
|
Thyroiditis
|
16
|
|
Thyroid nodules
|
6
|
|
Lymphadenopathy
|
4
|
|
Carotidynia
|
1
|
|
Submandibular duct calculus with sialadenitis
|
1
|
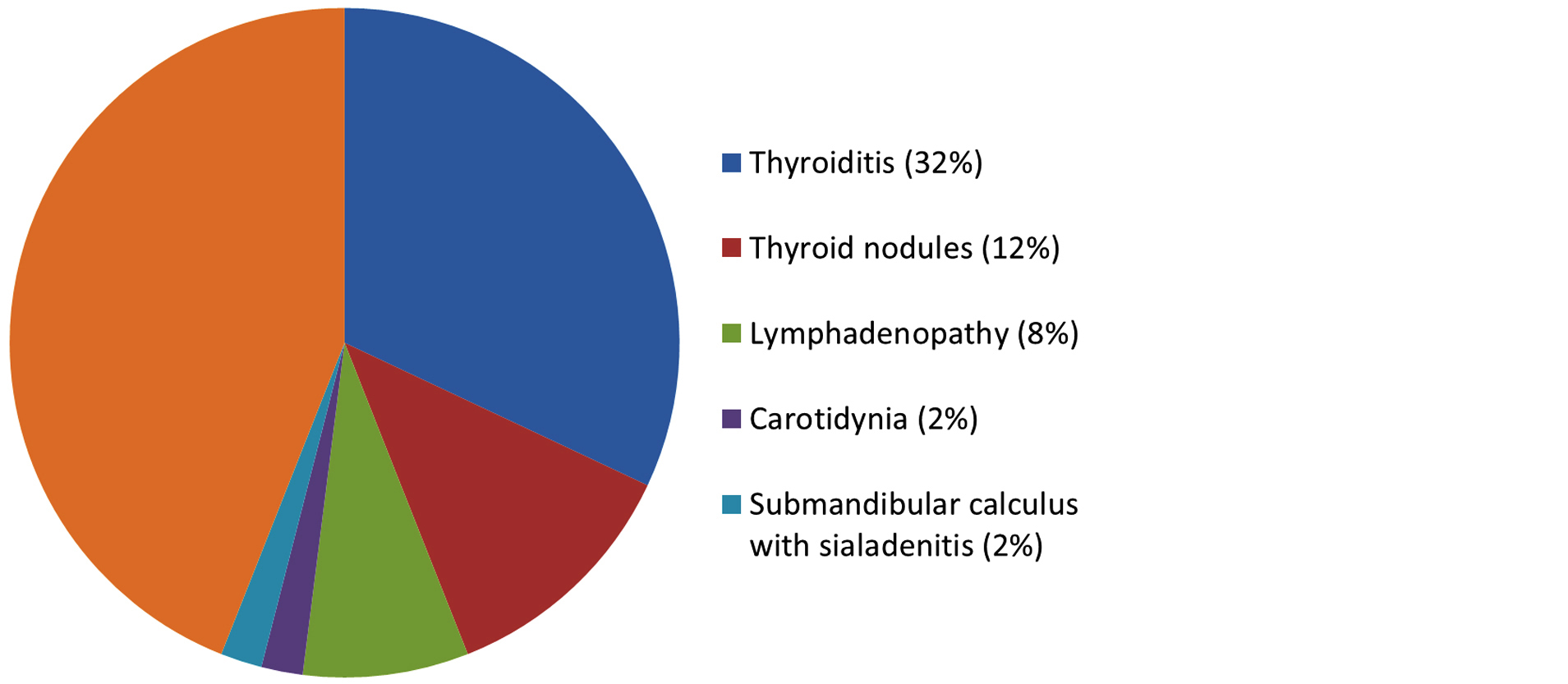
Figure 1: Pie chart showing distribution of findings in our study.
Transverse ultrasound image of the neck in a 36-year-old female with globus pharyngeus shows an enlarged, hypoechoic thyroid gland, suggestive of thyroiditis, with no focal lesions (Figure 2). In a 48-year-old male with globus pharyngeus, the image reveals multiple tiny hypoechoic nodules in the left thyroid lobe, indicating subacute thyroiditis, with increased vascularity (Figure 3).

Figure 2: Transverse ultrasound image of the neck in a 36-year-old female with globus pharyngeus showing an enlarged hypoechoic thyroid gland consistent with thyroiditis, without focal lesions.
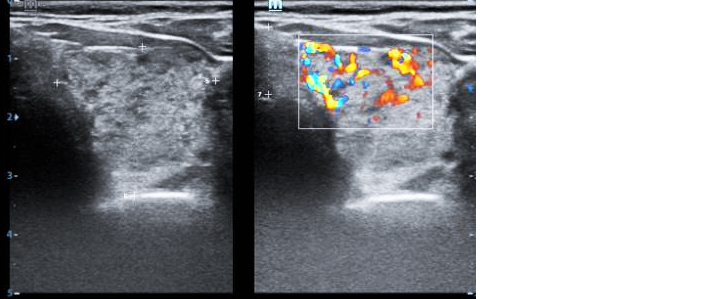
Figure 3: Transverse ultrasound image of the neck in a 48-year-old male with globus pharyngeus showing multiple tiny hypoechoic nodules in the left thyroid lobe, consistent with subacute thyroiditis and increased vascularity.
Transverse ultrasound image of the neck in a 28-year-old female with globus pharyngeus shows a well-circumscribed, solid, isoechoic nodule in the right thyroid lobe, measuring 2.2 cm. The nodule is wider than tall and classified as TIRADS 3, with follow-up suggested. The rest of the thyroid is normal (Figure 4). Transverse ultrasound image of the neck in a 30-year-old female with globus pharyngeus shows a well-circumscribed, solid, hypoechoic nodule in the right thyroid lobe, measuring 1 cm. The nodule is wider than tall and classified as TIRADS 4, with follow-up ultrasound suggested. The rest of the thyroid is normal (Figure 5). Ultrasound images of the neck in a 42-year-old female with globus pharyngeus reveal eccentric wall thickening in the right common carotid artery, with no calcification or stenosis. Grey scale (Figure 6a) and Colour Doppler (Figure 6b) images at the carotid bifurcation show eccentric wall thickening and colour flow within the lumen.
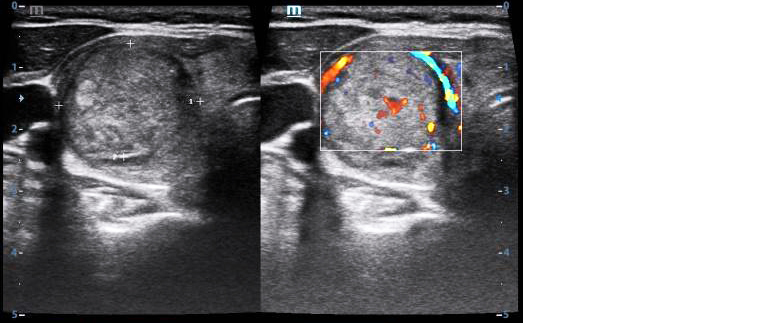
Figure 4: Transverse ultrasound image of the neck in a 28-year-old female with globus pharyngeus showing a 2.2 cm TIRADS 3 nodule in the right thyroid lobe, with normal thyroid echoes.
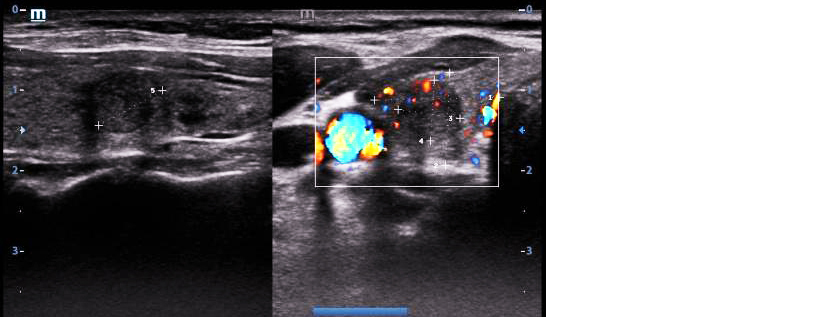
Figure 5: Transverse ultrasound image of the neck in a 30-year-old female with globus pharyngeus showing a 1 cm TIRADS 4 hypoechoic nodule in the right thyroid lobe.
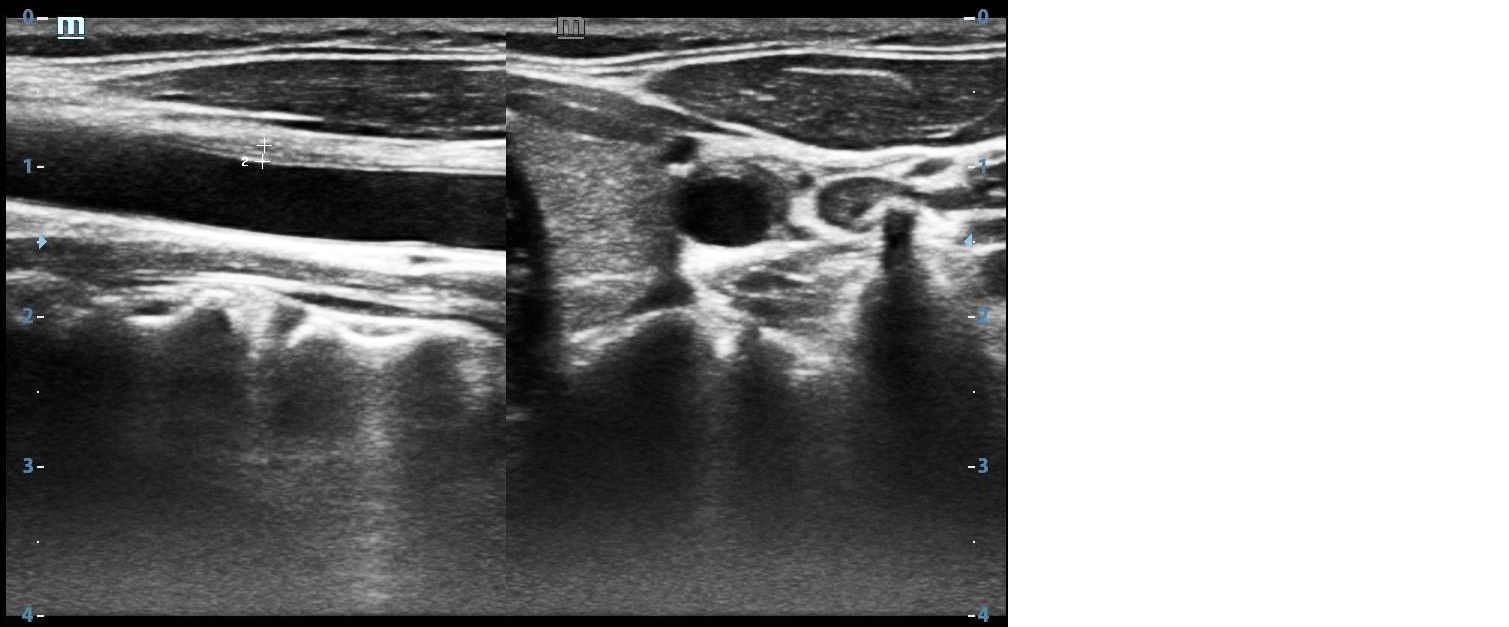
Figure 6a: Ultrasound images of the neck in a 42-year-old female with globus pharyngeus showing eccentric wall thickening in the right common carotid artery, without calcification or stenosis.
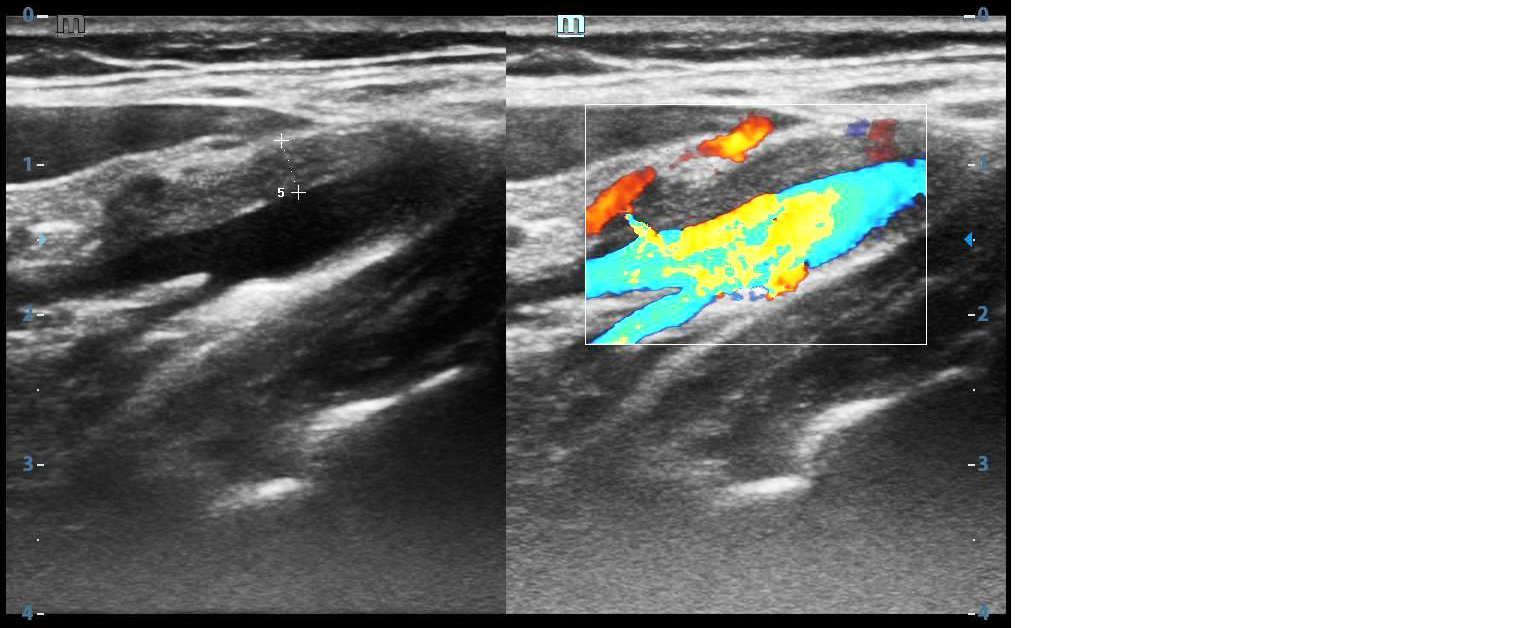
Figure 6b: Grey scale and Colour Doppler images showing eccentric wall thickening and colour flow within the lumen at the carotid bifurcation.
Ultrasound images of the neck in a 52-year-old male with globus pharyngeus show an enlarged lymph node with liquefactive changes. FNAC confirmed squamous cell carcinoma deposits (Figure 7). In a 25-year-old male with pain, ultrasound of the left submandibular region reveals a 1.2 cm hyperechoic calculus with posterior shadowing and a dilated duct. Colour Doppler shows a hypoechoic, hyperaemic submandibular gland, consistent with sialadenitis (Figure 8).
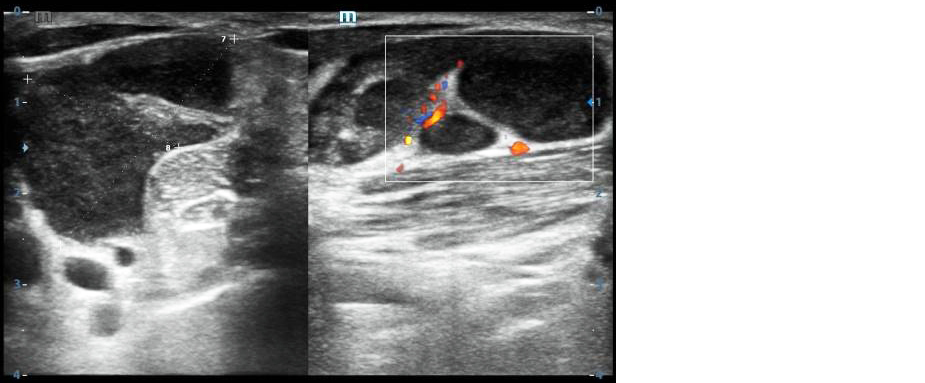
Figure 7: Ultrasound images of the neck in a 52-year-old male with globus pharyngeus showing an enlarged lymph node with liquefactive changes, confirmed as squamous cell carcinoma by FNAC.
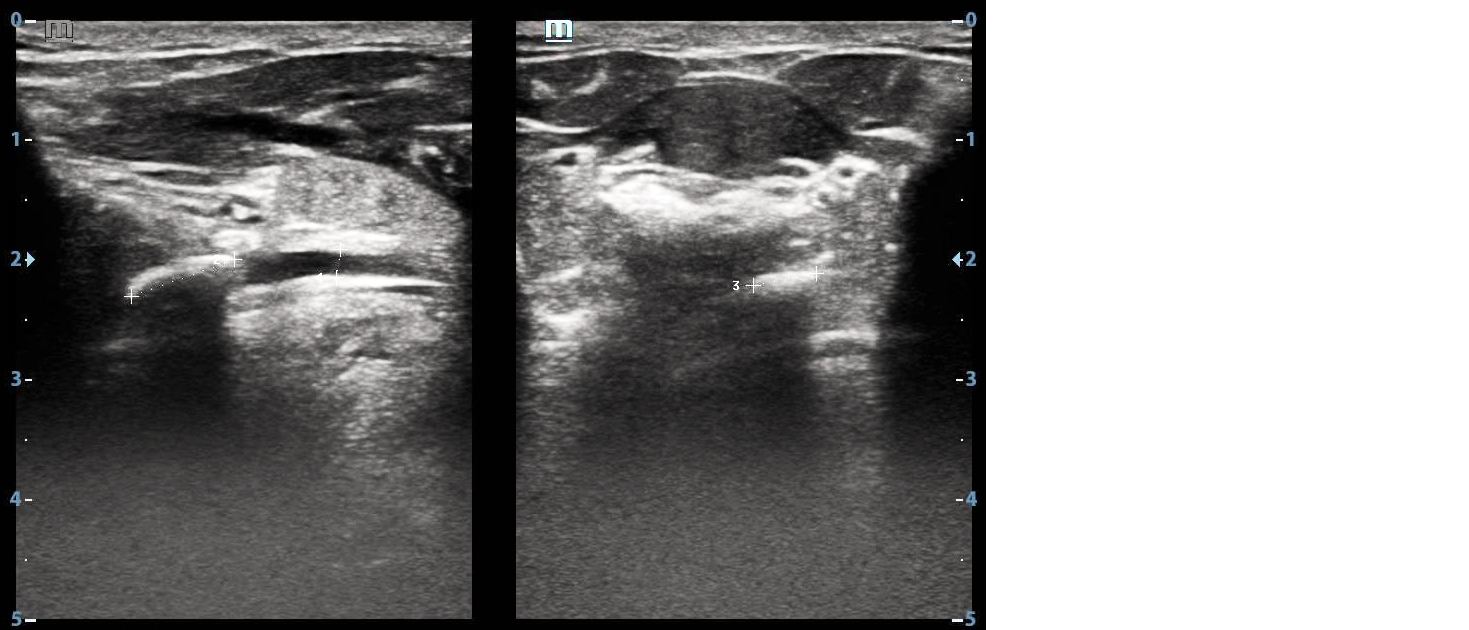
Figure 8a: Ultrasound images of the left submandibular region in a 25-year-old male with pain showing a 1.2 cm hyperechoic calculus with shadowing and a dilated duct.
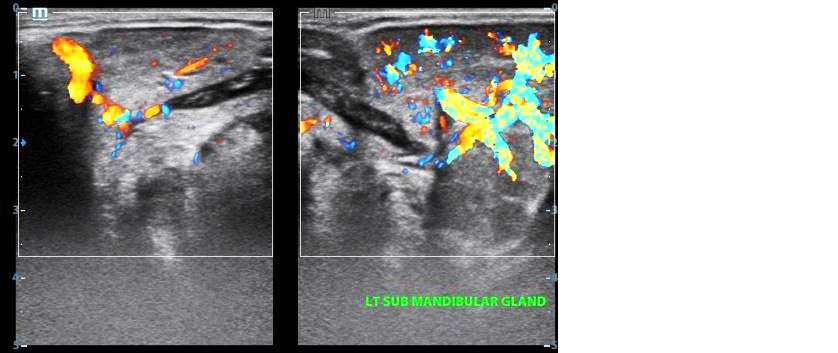
Figure 8b: Colour Doppler image showing a hypoechoic, hyperaemic left submandibular gland, consistent with sialadenitis, in the same patient as Figure 8a.
Discussion
Globus pharyngeus, earlier called globus hystericus, is the persistent or intermittent sensation of pain, uncomfortable feeling, or lump or foreign body sensation in the throat [1]. It contributes between 4% and 5% of otolaryngology outpatient visits. The etiology is varied, and includes gastroesophageal reflux disease, inflammatory disorders, motility disorder, anatomical variants, neoplasia, stress, and psychological factors. In 50% of patients, no cause is identified [3].
Various investigations in the armamentarium of physicians for the evaluation of patients with globus pharyngeus include endoscopy, ultrasonography, barium studies, contrast-enhanced computed tomography (CECT), and esophageal manometry. We intended to explore the role of ultrasonography in patients who had normal findings on clinical examination and laryngoscopy. Clinical examination and laryngoscopy can identify inflammatory disorders, hypertrophy of the base of the tongue, retroverted epiglottis, vocal cord palsy, and mucosal mass lesions of pharynx and larynx.
Ultrasonography is a widely available non-invasive tool. Of the 50 patients who were referred to us, 28 patients (56%) had findings on ultrasonography in our study. Patients with thyroid disorders form the majority of the group with findings. 16 patients had diffuse lesions and 6 had focal nodules. Majority of the diffuse lesions were thyroiditis and one patient had multinodular goitre. In patients with thyroid nodules, four had TIRADS 3 nodules, one had colloid cyst under TIRADS 2 and one had two TIRADS 4 nodules.
In a study by Nam et al in 2015, of 175 patients with globus symptoms and thyroid nodules, it was found that nodules >3 cm and those that located anterior to trachea showed higher tendency for globus symptoms [4]. In our study, the patient with colloid cyst had >3 cm nodule extending anterior to trachea.
In a study by P Burns and C Timon, 58 of 200 patients who underwent thyroid surgery had globus symptoms preoperatively. Post surgery, symptoms resolved in 80% of patients. Of these, patients with inflammation histologically showed the greatest improvement [5]. In our study, imaging features of thyroiditis are seen in 16 (32%) patients, correlating with their results.
Salivary gland hypofunction leading to dry mouth has been found to exaggerate the symptoms of globus pharyngeus [6]. One patient had calculus disease with sialadenitis in our study. Both dry mouth (due to sialolith) and swelling and pain (due to sialadenitis) might have contributed to the globus symptom in our patient.
Kinking of the carotid artery has been found in a patient with globus pharyngeus [7]. In our study, one patient had eccentric wall thickening of the left common carotid artery. It was tender with minimal luminal narrowing. Inflammatory markers were not elevated, without flow disturbance. A diagnosis of carotidynia was made. Carotidynia is a rare vascular disorder and is usually self-limiting [8]. Carotidynia has to be differentiated from atherosclerosis (concentric wall thickening with calcification and flow disturbance) and vasculitis (elevated inflammatory markers). Treatment is supportive, with non-steroidal anti-inflammatory drugs and reassurance.
Enlarged lymph nodes as a cause of globus sensation was reported in patients with lymphoma [9]. In our study, four patients had lymphadenopathy. One patient had necrotic lymph nodes, which subsequently on FNAC was proved to be metastatic squamous cell carcinoma. Other patients had Tuberculous nodes.
In our study, 56% of patients with globus pharyngeus had positive findings on ultrasonography. In a similar study of 75 patients by Fukuhara et al (2021), structural abnormalities were observed in 60.8 % of the patients [2].
Malcomson identified GERD as the cause for globus pharyngeus in 60% of patients [10]. We suggest that in the absence of positive findings on ultrasonography, patients can be prescribed a trial of proton pump inhibitors for six weeks to tackle GERD. Patients with persistent symptoms can undergo CECT and invasive procedures including endoscopy and esophageal manometry.
In patients with acute onset dysphagia and odynophagia, esophageal manometry, endoscopy, and/or CECT are advisable.
Limitations: It is a single-center study with a small sample size, consisting of patients referred from our institution. Larger, multicenter studies are needed to further evaluate the role of cervical ultrasonography as a first-line tool in the assessment of patients with globus pharyngeus.
Conclusion
Ultrasonography is an excellent first line tool in the evaluation of globus pharyngeus. It detects thyroid disorders, lymphadenopathy, carotid lesions and salivary gland disorders. Ultrasonography is non-invasive and helps arrive at a diagnosis in over 50% of patients. Further clinical studies are needed to assess the long-term outcomes of patients with carotidynia presenting with globus symptoms.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Chauhan N, Sharma S, Kaushal D. An insight into globus pharyngeus: a diagnostic dilemma. IP J Otorhinolaryngol Allied Sci. 2022; 5:62–63.
[2] Fukuhara T, Matsuda E, Ogawa A, Donishi R, Koyama S, et al. Use of cervical ultrasonography in globus sensation investigation: a retrospective cohort study. Yonago Acta Med. 2021; 64:360–363.
[3] Lee BE, Kim GH. Globus pharyngeus: a review of its etiology, diagnosis and treatment. World J Gastroenterol. 2012; 18:2462–2471.
[4] Nam IC, Choi H, Kim ES, Mo EY, Park YH, et al. Characteristics of thyroid nodules causing globus symptoms. Eur Arch Otorhinolaryngol. 2015; 272:1181–1188.
[5] Burns P, Timon C. Thyroid pathology and the globus symptom: are they related? A two year prospective trial. J Laryngol Otol. 2007; 121:242–245.
[6] Baek CH, Chung MK, Choi JY, So YK, Son YI, et al. Role of salivary function in patients with globus pharyngeus. Head Neck. 2010; 32:244–252.
[7] Lim LY, Mat Lazim N. Carotid artery and globus: how are they related? J Pioneering Med Sci. 2018; 8:41–43.
[8] Abbasi A, Khan MAB. Carotidynia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560841
[9] Varghese SS, Varghese A, Paul PAM, Dhawan K, Gupta P. Laryngeal anaplastic lymphoma kinase-positive B-cell lymphoma: patient report and review. Indian J Otolaryngol Head Neck Surg. 2023; 75:2328–2333.
[10] Malcomson KG. Globus hystericus vel pharyngis (a reconnaissance of proximal vagal modalities). J Laryngol Otol. 1968; 82:219–230.