Full Text
Introduction
Gastrointestinal tract malignancies are one among the most common type of malignancies which are affecting the people worldwide [1]. India is a developing country with one of the most diverse population and diet in the world. Cancer rates are lower in India as compared to western countries but are rising because of increasing migration of rural population to cities, increasing life expectancy and changing life style [2].
In India, esophageal cancer is the fourth most common cause of cancer-related deaths. Approximately, 47,000 new cases and 42,000 deaths are reported each year in India due to esophageal cancer [3]. Majority of the esophageal malignancies are squamous in origin while incidence of adenocarcinoma is on constant rise due to the changing lifestyle. The malignancies located in esophagus are generally associated with poorer prognosis [3]. The incidence of esophageal cancer in India is moderately high, associated with diets and lifestyles. According to a data from National Cancer Registry, esophageal cancer is the second most common cancer among males and the fourth most common cancer among females [4]. Risk factors for esophageal carcinoma include age 45 – 70 years, Male gender, tobacco, alcohol, Barrett’s esophagus, diet/ nutrition, obesity, achalasia, plummer-vinson or Paterson-Kelly syndrome and Hiatal hernia [5].
Stomach cancer is the second most common cancer among men, third-most among females in Asia and worldwide. The 5 year survival rate is less than 20% in developing countries. Gastric carcinomas are usually diagnosed at advanced stages and lead to 20 % of deaths within 5 year after diagnosis [6]. Stomach cancer is the second most common cancer among men and third most common among females in Asia and worldwide [7]. There is decreased incidence in United States and England, whereas high in Japan, Chile and Italy [8]. Differences in some dietary pattern and use of tobacco and alcohol have been considered as potential risk factors. Mizoram has the highest number of gastric cancer cases in India. Dietary habits among the residants of Kashmir such as smoking of hukka, smoked fish and mixed spice cake, consuming dried and pickled vegetables is probably the reason for the increased incidence of gastric carcinoma in that area [9]. Risk factors for gastric carcinoma [8, 10] include age 60-70 years, male gender, helicobacter pylori bacteria, family history/genetics, blacks, hispanic and Asian race, diet, previous surgery or health condition, tobacco and alcohol, obesity and epstein barr virus infection [7].
Small bowel adenocarcinoma (SBA) are rare tumors, but their incidence is increasing. Adenocarcinoma of small bowel is 40-60 times less common than large bowel adenocarcinoma [8]. Duodenum is the most common site of small bowel adenocarcinomas. Despite the fact that the small intestine makes up to 75% of the length of the digestive tract and 90% of its mucosal surface area, small bowel cancer is rare, accounting for less than 5% of gastrointestinal cancers [8].
In India, colorectal cancer is the fourth most common cause of cancer in males, third most common cause of cancer in females. Colorectal cancer is the cancer of old age; mostly occurs after fifth decade of life. However, the incidence of colorectal cancer is increasing in young age, mainly due to change in lifestyle and food habits [11]. First degree relatives of colorectal cancer patients are at increased risk. Familial adenomatous polyposis (FAP) has the highest predisposition for colorectal adenocarcinoma. Having a family member with FAP also contributes to the malignancy. Hereditary non-polyposis colorectal cancer (HNPCC), Peutz-jeghers syndrome and MYH- associated polyposis (MAP) doubles the risk of colon cancer. High salt diet increases the risk. Also preserved foods, smoked foods, pickled foods, beef consumption, increased fat and animal product consumption, processed foods increase the risk. Eating fresh fruits and vegetables lowers the risk of developing colorectal cancer [12].
Types of intestinal carcinomas include adenocarcinoma, neuroendocrine tumors, gastrointestinal stromal tumors and lymphomas. Squamous cell carcinoma occurs at the gastroesophageal junction and at the anal verge. Mesenchymal tumors such as leiomyoma, schwannoma, solitary fibrous tumor are also not uncommon [12]. The prognosis of gastrointestinal carcinoma depends on patient’s age, tumor grade and location of the tumor. pTNM staging is the single most important factor for prognosis prediction. Histological pattern also determines prognosis. Old age, high tumor stage and grade and also certain locations are associated with poor prognosis [7, 8].
Gastrointestinal tract is a fertile soil for various neoplasms, with varied morphology and prognosis. Thus, this study aimed to study the morphological spectrum of gastrointestinal malignancies by histopathological examination.
Materials and methods
This is a prospective study done in Department of Pathology, Mysore Medical College and Research Institute, Mysuru during the period of December 2019 – May 2021 (18 months). The ethical approval was obtained from the Institutional ethics committee. The biopsies and resected specimens were collected from the Department of Pathology. All types of esophageo-gastrointestinal carcinomas were included in the study. Cases where there is extensive tumor necrosis without viable tumor cells for accurate evaluation and those who underwent adjuvant chemotherapy were excluded from the study. The detailed clinical history including the age, gender and results of relevant investigation done, was collected from the patient’s case records. In every case the standard protocol for surgical grossing of specimens was followed. After conventional processing, paraffin sections of 5µm thickness were stained by haematoxylin and eosin for histopathological study.
The tumors were categorized according to the WHO 2019 classification. Staging was done according to TNM staging. Histological types and grade of the tumors were also determined. The data was collected, statistically evaluated and represented in terms of frequency distribution tables. The categorical and counting variables were presented by frequencies and percentages. The proportion of subjects according to the various subgroups such as age, gender, type of cancer, grade and stage was estimated.
Results
A total of 40 cases of esophageo-gastrointestinal carcinomas were taken for the study. Standard protocol for grossing and histopathological techniques were followed. In the present study, more number of cases were in the age group 61-70 years and least were in <40 years age group and majority of the cases were males, that is 24 out of 40 cases. The major site of carcinoma was left colon and stomach. Least number of cases were from small intestine, right colon and esophagus (Figure 1) (Table 1).

Figure 1: Gross photo of esophageal carcinoma, showing growth at lower end of esophagus.
Table 1: Number of cases from different sites and average age according to sites.
|
Location of the lesion
|
No of cases
|
% of cases
|
Average age
|
|
Esophagus
|
7
|
17.50
|
51.71
|
|
Stomach
|
9
|
22.5
|
60.33
|
|
Small intestine
|
0
|
0
|
0
|
|
Right colon
|
6
|
15
|
57.83
|
|
Left colon/colo-rectum
|
18
|
45
|
58.16
|
Majority of the cases were left colonic (Figure 2) and stomach carcinomas (Figure 3). The average age for left colon carcinoma was 58 years, average age for stomach carcinoma was 60 years and for esophageal carcinoma it was 52 years. Hence from this observation, it was found that the average age group affected was 50-60 years. Majority of the cases of esophageal carcinoma were diagnosed as Squamous cell carcinoma. Only 1/7 esophageal carcinomas was diagnosed as adenocarcinoma. Gastrointestinal carcinoma cases were all diagnosed as adenocarcinoma (Table 2).
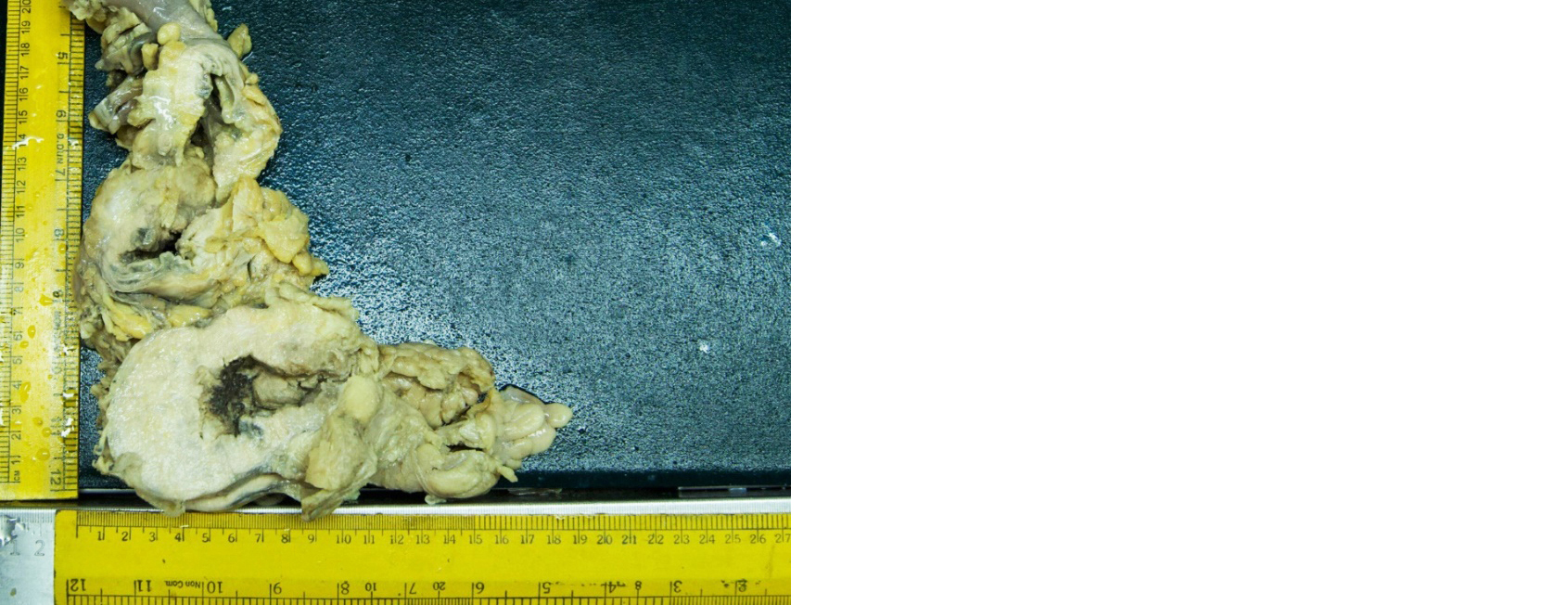
Figure 2: Gross photograph of descending colon showing large infiltrative growth with areas of necrosis and ulceration over the mucosal surface.

Figure 3: Gross photograph of gastric carcinoma showing solid grey white growth in the lumen.
Table 2: Histological type wise distribution of esophageo-gastrointestinal carcinoma.
|
Histological type
|
Total
|
% of cases
|
|
Squamous cell carcinoma
|
6
|
15
|
|
Adenocarcinoma
|
34
|
85
|
|
Neuroendocrine carcinoma
|
0
|
0
|
Grading was done according to WHO 2010 guidelines. Out of 40 cases, 15 cases were Grade 1/well differentiated carcinoma, 18 cases were grade 2/moderately differentiated and only 7 cases were grade 3/poorly differentiated carcinoma. Hence majority of the cases were moderately differentiated/grade 2 carcinoma (Table 3).
Table 3: Grade wise distribution of esophageo-gastro-intestinal carcinomas.
|
Grade
|
No of cases
|
Percentage (%)
|
|
Grade 1/Well differentiated carcinoma
|
15
|
37.5
|
|
Grade 2/Moderately differentiated carcinoma
|
18
|
45
|
|
Grade 3/poorly differentiated carcinoma
|
7
|
17.5
|
In the present study, 11/40 cases were biopsy specimens. Majority of the cases (29/40) were resected specimens. Hence staging was done to the resected specimens. Staging was done according to the WHO (2010) guidelines. Out of 29, 8 cases were in stage I, 12 cases were in stage II,9 cases were in stage III and none in stage IV. Hence from this observation it was found that the majority of the cases were in stage II in the present study (Table 4).
Table 4: Stage wise distribution of esophageo-gastrointestinal carcinomas.
|
Stage of the carcinoma
|
No. of cases
|
% of cases
|
|
Stage 1
|
8
|
27.58
|
|
Stage 2
|
12
|
41.37
|
|
Stage 3
|
9
|
31.03
|
|
Stage 4
|
0
|
0
|
Out of 40 cases, 7 cases were esophageal carcinoma and 6/7 were diagnosed as squamous cell carcinoma and 1/7 was diagnosed as adenocarcinoma. Among 6 cases of esophageal squamous cell carcinoma, 1 (14.28%) was well differentiated carcinoma, 4 (57.14%) were moderately differentiated carcinoma (Figure 4) and 1(14.28%) was poorly differentiated carcinoma (Figure 5). Adenocarcinoma was diagnosed to be well differentiated carcinoma. Out of 40 cases, 9 cases were from the stomach and all were adenocarcinoma (Figure 6). Grading of the tumor was done as per the WHO 2010 guidelines. Majority were moderately differentiated adenocarcinoma (Figure 7) and 2 cases were diagnosed as poorly differentiated carcinoma. Out of 40 cases, 24 cases were colorectal carcinoma. All the cases of colon were diagnosed as adenocarcinoma. Among 24 cases of colorectal adenocarcinoma, 12(50%) were well differentiated, 9(37.5%) were moderately differentiated and 3(12.5%) were poorly differentiated adenocarcinoma. One case of mucinous adenocarcinoma was identified (Figure 8).
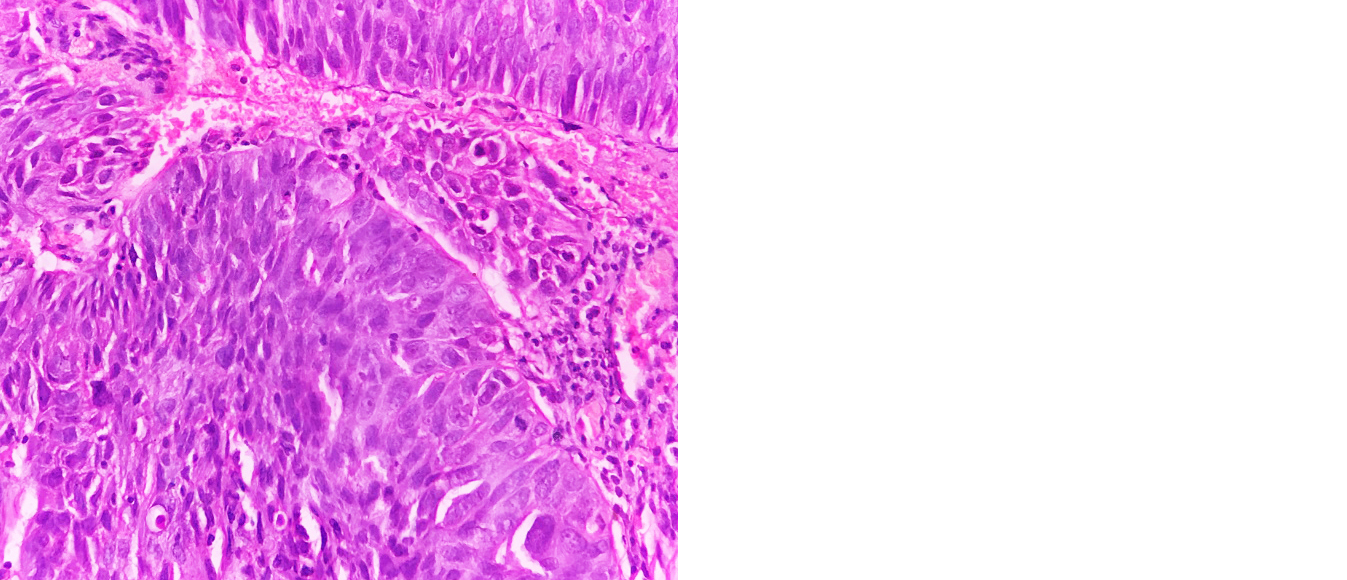
Figure 4: Photomicrograph of moderately differentiated esophageal squamous cell carcinoma (H&E; 40x).
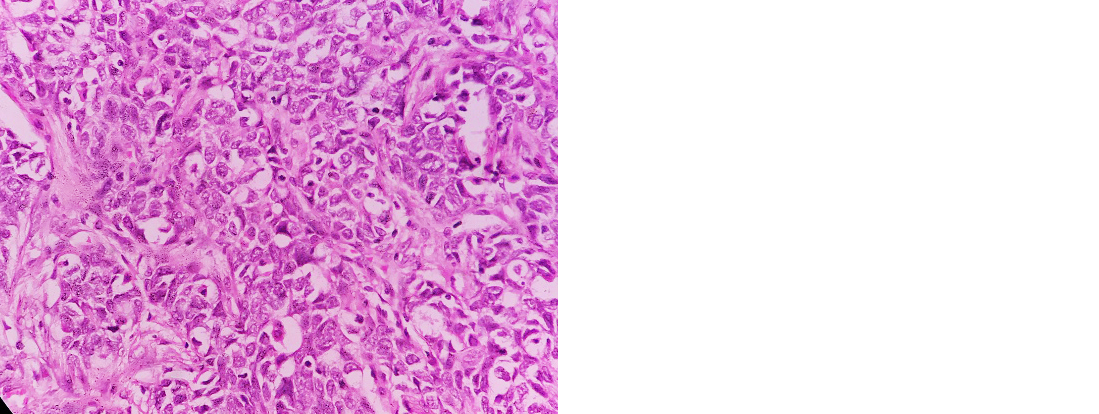
Figure 5: Photomicrograph of poorly differentiated squamous cell carcinoma (H&E; 40x).
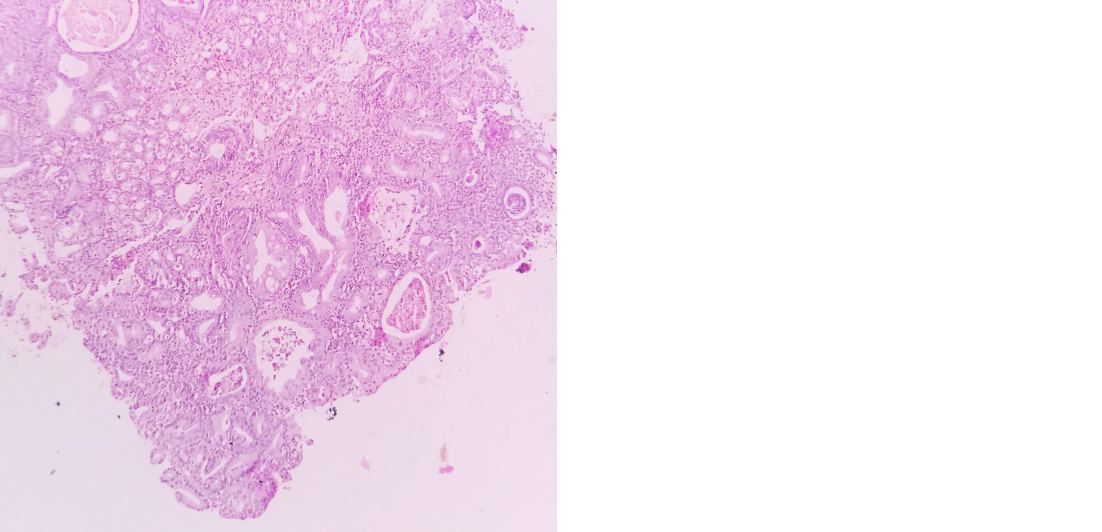
Figure 6: Photomicrograph of well differentiated adenocarcinoma of stomach (H&E, 10x).
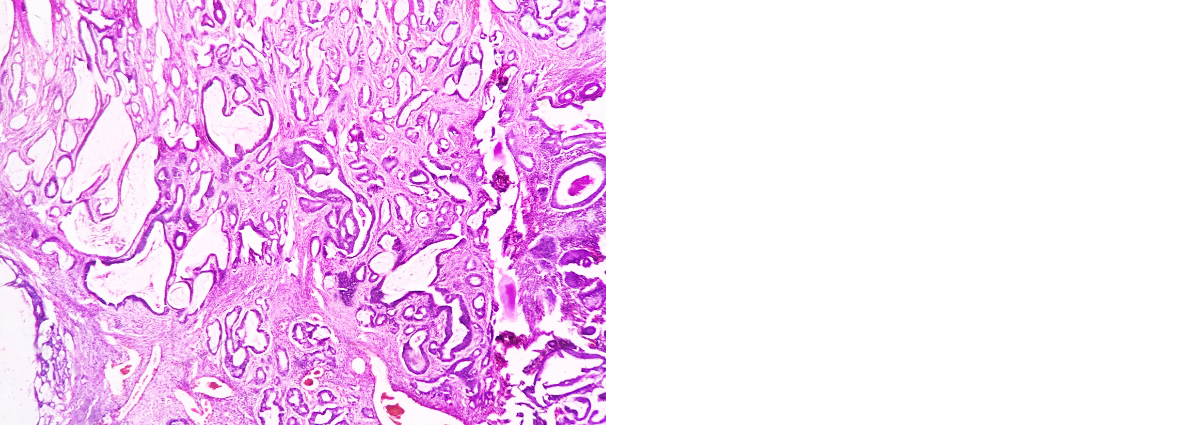
Figure 7: Photomicrograph of moderately differentiated rectal adenocarcinoma (H&E; 10x).
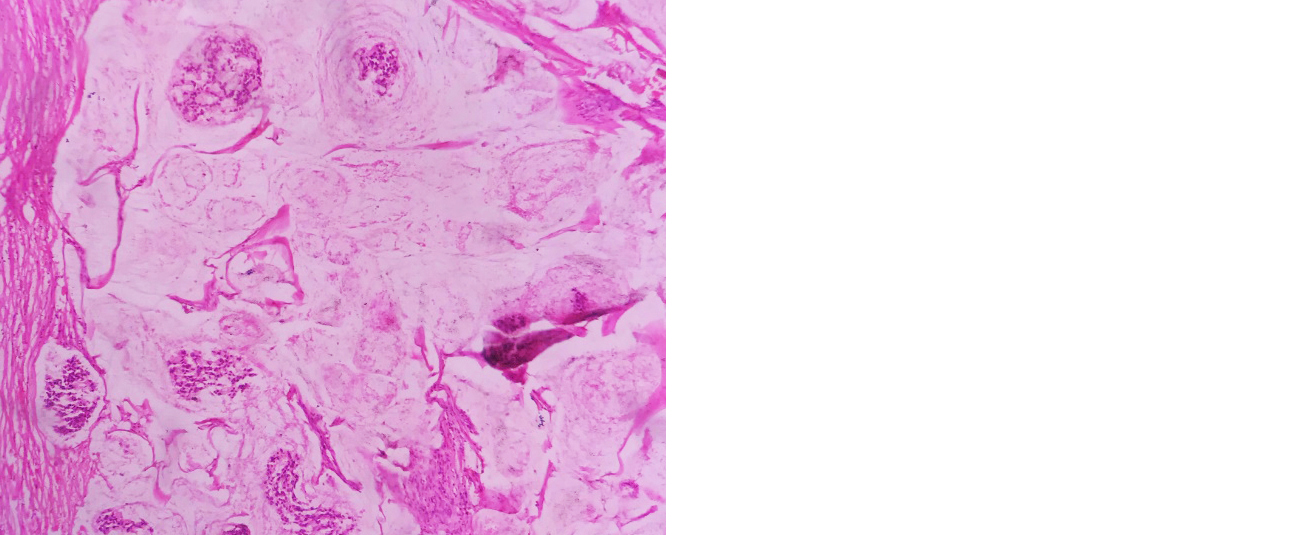
Figure 8: Photomicrograph of mucinous adenocarcinoma of colon (H&E; 10x).
Discussion
Gastrointestinal malignancies are one of the common malignancies affecting individuals with poor dietary habits, family history and genetic mutations. Metastasis from the primary digestive tract carcinomas are commonly encountered during the clinical practice. The determination of primary site in ‘tumors of unknown origin’ is crucial because it affects the treatment and prognosis of the patient [13, 14].
The mean age of esophageal malignancies in the present study was 52 years. This was in concordance with the study done by Singh et al [15]. The studies done by Driessen et al [16] and Yamada et al [17] showed mean ages of 65 years and 62 years, respectively, which was higher than our study. In the present study, the mean age of gastric malignancies was 60 years which was similar to the study done by Yu et al [18]. In the present study, colorectal malignancies presented at a mean age of 58 years. Similar age incidence was noted in the study done by Gheini et al [19]. However, the mean age in the present study was lower compared to the studies done by Ljuslinder et al [20] and Spano et al [21].
The incidence of esophageal and gastric malignancies was higher in malescompared to females. This was in correlation with the studies done by Driessen et al [16], Yamada A et al [17], Singh et al [15], Yu et al [18]. Increased alcohol consumption and smoking habits which are the risk factors for upper gastrointestinal tract malignancies might be the cause forthe increased incidence among males. No significant gender predominance was found in the incidence of colorectal malignancies. The studies done by Gheini et al [19], Ljuslinder et al [19] and Spano et al [20] also showed similar results.
In the present study, colorectum was the predominant site of malignancy in the esophageo-gastrointestinal tract with 60% of cases. This correlates with the studies of Sharma et al [1], Chu et al [22] and Kende et al [23] (Table 5).
Table 5: Comparison of site of esophageo-gastrointestinal malignancies with other studies.
|
Author
|
Total cases
|
Esophagus
n(%)
|
Stomach
n(%)
|
Small intestine n(%)
|
Colorectum
n(%)
|
|
Sharma et al [1]
|
40
|
9(22.5)
|
4(10)
|
3(7.5)
|
24(60)
|
|
Chu et al [22]
|
42
|
14(33.3)
|
8(19.0)
|
0(0)
|
20(47.6)
|
|
Kende et al [23]
|
78
|
11 (14.1)
|
38(49.3)
|
0(0)
|
29(37.17)
|
|
Present study
|
40
|
7(17.5)
|
9(22.5)
|
0(0)
|
24(60)
|
In our study, we did not find any case of small intestinal malignancies similar to the studies done by Chu et al [22] and Kende et al [23]. Similarly, the study done by Sharma et al [1] also had least incidence of small intestinal malignancies compared to colorectal, esophageal and gastric malignancies. The incidence of malignancies in small intestine are extremely rare compared to large intestine. Several mechanisms have been hypothesised to explain this difference. Quicker transit time of chyme and lower bacterial load in small intestine compared to large intestine are known to reduce the exposure of its mucosa to carcinogens and thus the reduced incidence of cancer. Increased levels of IgA and reduced reactive oxygen species in small intestine are also known to have a protective role in small intestine against malignancies. The distinction in the frequency of esophageal carcinoma and gastric carcinoma was not statistically significant. This correlates with the studies done by Sharma et al [1] and Chu et al [22]. The histopathological spectrum of esophageal, gastric and colorectal malignancies was comparable with studies done by Chu et al [22)], Kende et al [23], Bayrak et al [13], Wang et al [24] and Kummar et al [25], respectively (Table 6).
Table 6: Comparing of distribution of histopathological spectrum of esophageo-gastrointestinal malignancies.
|
Author
|
Histological type
|
Total cases
|
|
Esophageal carcinoma
|
|
Driessen et al [16]
|
Adenocarcinoma
|
66
|
|
Squamous cell carcinoma
|
0
|
|
Chu et al [22]
|
Adenocarcinoma
|
0
|
|
Squamous cell carcinoma
|
14
|
|
Present study
|
Adenocarcinoma
|
1
|
|
Squamous cell carcinoma
|
6
|
|
Gastric carcinoma
|
|
Kende et al [23]
|
Adenocarcinoma
|
38
|
|
Bayrak et al [13]
|
Adenocarcinoma
|
59
|
|
Present study
|
Adenocarcinoma
|
9
|
|
Colorectal malignancies
|
|
Chu et al [22]
|
Adenocarcinoma
|
20
|
|
Wang et al [24]
|
Adenocarcinoma
|
40
|
|
Kummar et al [25]
|
Adenocarcinoma
|
26
|
|
Present study
|
Adenocarcinoma
|
24
|
The grade of the tumor indicates the likelihood of tumor to spread and grow and hence indirectly determines the prognosis of the carcinoma. Therefore, it is essential to grade the tumor. In the present study, the tumors were graded according to WHO 2010 guidelines. Some of the authors have followed two-tier system of grading which groups well differentiated and moderately differentiated tumors under low grade and poorly differentiated under high grade tumors. In the present study, 45% of the esophageo-gastrointestinal carcinoma were in grade 2 and 37.5% were in grade 1. This predominance of well and moderately differentiated carcinomas was in concordance with the studies done by Yamada et al [18], Oue et al [26], Bayrak et al [13] and Gheini et al [19].
In the present study, out of 40 specimen, 29 were resected specimens, rest all were biopsy specimens. Hence staging was possible only on resected specimens. Staging was done according to WHO 2010 guidelines. Majority of the cases were in stage II in the present study. Similarly, the studies conducted by Yamada et al [18] and Takami et al [27] also showed similar comparison with the stage of the tumor.
Limitations of the study include that this is a single institute study done on a small number of population. Thus, we recommend multicentric study on a larger group of study population.
Conclusion
The present study highlights the crucial role of histopathological examination in diagnosing the esophageo-gastrointestinal carcinomas. Grading and staging plays an essential role in prognostification and risk assessment of these cancers, which further significantly affects the disease management and patient survival.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Sharma R, Baghla A, ChahalKS, Girdhar M. Immunohistochemical expression of cytokeratin 20 in various malignant conditions of gastrointestinal tract. Int J Sci Res. 2017; 6:4–7.
[2] Sinha. Cancer risk and diet in India. J Postgrade Med. 2003; 49:222–228.
[3] Samarasam I. Esophageal cancer in India: Current status and future perspectives. Int J Adv Med Health Res. 2017; 4:5–10.
[4] Ali I, Wani WA, Saleem K. Cancer scenario in India with future perspectives. Cancer Therapy. 2011; 8:56–70.
[5] DomperArnal MJ, Arenas AF, Arbeloa L. Esophageal cancer: Risk factors, screening and endoscopic treatment. World J Gasteroenterol. 2015; 21:7933–7943.
[6] Dikshit RP, Mathur G, Mhatre S, Yeole BB. Epidemiological review of gastric cancer in India. Indian J Med Paed Oncol. 2011; 32:3–11.
[7] Bosman FT, Carneiro F, Hruban RH, Thesie ND. Tumours of the stomach; WHO classification of tumours of the digestive system. 4th ed. International Agency for Research on Cancer. 2010; pp.45–79.
[8] Rosai J. Rosai and Ackerman’s Surgical Pathology. 11th ed. Philadelphia, PA; Elsevier, 2018; pp.541–688.
[9] Sharma A, Radhakrishnan V. Gastric cancer in India. Indian J Med Paediatr Oncol. 2011; 32:12–26.
[10] Yusefi AR, Lankarani KB, Bastani P, Radinmanesh M, Kavosi Z. Risk factors for gastric cancer: a systemic review. Asian Pacific J Cancer Prevention. 2018; 19:591–603.
[11] Sharma D, Singh G. Clinico-pathological profile of colorectal cancer in first two decades of life: A retrospective analysis from tertiary health center. Indian J Cancer. 2017; 54:397–400.
[12] Bosman FT, Carneiro F, Hruban RH, Thesie ND. Tumours of the small intestine; WHO classification of Tumours of the Digestive System. 4th ed. International Agency for Research on Cancer, 2010; pp.95–117.
[13] Bayrak R, Haltas H, Yenidunya S. The value of CDX2 and Cytokeatins 7 and 20 expression in differentiating colorectal adenocarcinomas from extraintestinal gastrointestinal adenocarcinomas: cytokeratin7-/20+ phenotype is more specific than CDX2 antibody. Diagn Pathol. 2012; 7:9.
[14] Wong HH, Chu P. Immunohistochemical features of the gastrointestinal tract tumors. J Gastrointest Oncol. 2012; 3:262–284.
[15] Singh A, Kapur S, Chattopadhyay I, Purkayastha J, Sharma J, Mishra A et al. Cytokeratin immunoexpression in esophageal squamous cell carcinoma of high-risk population in Northeast India. Appl Immunohistochem Mol Morphol. 2009; 17:419–424.
[16] Driessen A, Nafteux P, Lerut T, Raemdonck DV, Leyn PD, et al. Identical cytokeratin expression pattern CK7+/CK20- in esophageal and cardiac cancer: Etiopathological and clinical implications. Modern Pathology. 2004; 17:49–55.
[17] Yamada A, Sasaki H, Aoyagi K, Sano M, Fujii S, et al. Expression of cytokeratin 7 predicts survival in stage I/IIA/IIB squamous cell carcinoma of the esophagus. Oncology Reports. 2008; 20:1021–1027.
[18] Yu J, He Y, Guo Z. Age trend of the male to female sex ratio in surgical gastric cancer patients at a single institution. World J Surg Oncol. 2014; 12:269.
[19] Gheini MH, Jalayernaderi N. The relationship between Cytokeratins 7 and 20 Expression, and Prognostic factors in Colon Adenocarcinoma: An Immunohistochemical Study. Iranian J Pathol. 2017; 12:94–98.
[20] Juslinder I, Melin B, Henriksson ML, Oberg A, Palmquist R. Increased epidermal growth factor receptor expression at the invasive margin is a negative prognostic factor in colorectal cancer. Int J Cancer. 2011; 128:2031–2037.
[21] Spano JP, Lagorce C, Atlan D, Milano G, Domont J, et al. Impact of EGFR expression on colorectal cancer patient prognosis and survival. Ann Oncol. 2005; 16:102–108.
[22] Chu P, Wu E, Weiss LM. Cytokeratin 7 and Cytokertain 20 Expression in Epithelial Neoplasms: A survey of 435 cases. The United States and Canadian Academy of Pathology 2000; 13:962–972.
[23] Kende AI, Carr NJ, SobinLH. Expression of cytokeratins 7 and 20 in carcinomas of the gastrointestinal tract. Histopathology. 2003; 42:137–140.
[24] Wang NP, Zee S, Zarbo RJ, Bacchi CE, Gown AM. Coordinate expression of cytokeratins 7 and 20 defines unique subsets of carcinomas. Appl Immunohistochem. 1995; 3:99–107.
[25] Kummar S, Forgarsi M, Canova A, Mota A, Ciesielski T. Cytokeratin 7 and 20 staining for diagnosis of lung and colorectal adenocarcinoma. British J Cancer. 2002; 86:1884–1887.
[26] Oue N, Noguchi T, Anami K, Kitano S, Sakamoto N, et al. Cytokeratin 7 is a predictive Marker for Survival in Patients with Esophageal Squamous Cell Carcinoma. Am Surg Oncol. 2012; 19:1902–1910.
[27] Takami H, Sentani K, Matsuda M, Oue N, Sakamoto N, et al. Cytokeratin expression profiling in gastric carcinoma: Clinicopathologic significance and comparison with tumor-associated molecules. Pathobiology. 2012; 79:154–161.