Full Text
Introduction
The term soft tissue tumors (STT) encompass a wide range of tumors arising from the mesenchymal tissues. These tumors are usually classified into three categories based on their differentiation and resemblance to the tissue of origin as benign, intermediate (including the locally aggressive and rarely metastazising variants) and malignant categories [1]. STTs are also associated with a wide range of recurring cytogenetic abnormalities which now have become the molecular markers for diagnosis of these tumors [1, 2]. In this study, we have retrospectively analysed the various STTs occurring in the Department of Pathology, in our institution over a period of 2 years.
Materials and methods
The present study was conducted in the Department of Pathology of our institute. We included all cases with a confirmed histopathological diagnosis of soft tissue lesions received during the study period of January 2018 – December 2019. These cases were further analysed for the site of the lesion, number of lesions, age and gender of the patients and the results tabulated. We excluded the skin tumors, adnexal tumors and bone tumors which also clinically mimic a soft tissue lesion. This study was approved by the institutional ethical committee.
Results
A total of 207 cases of soft tissue tumors with confirmed histopathological diagnosis were included in this study. The male: female ratio is 1.1:1. Figure 1 shows the gender distribution of the soft tissue tumors.
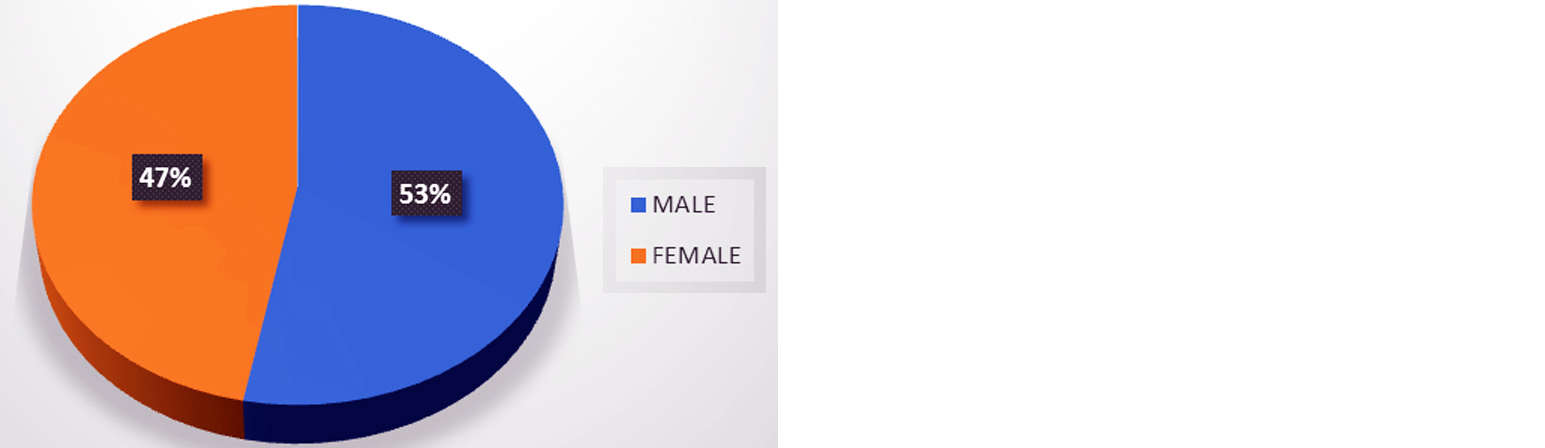
Figure 1: Gender distribution of soft tissue tumors.
The STTs were classified according to the WHO classification. Figure 2 shows the types of tumors observed in this study with the percentage of incidence.

Figure 2: Percentage distribution of soft tissue tumors.
The age wise distribution and occurrence of soft tissue tumors is shown in Figure 3.
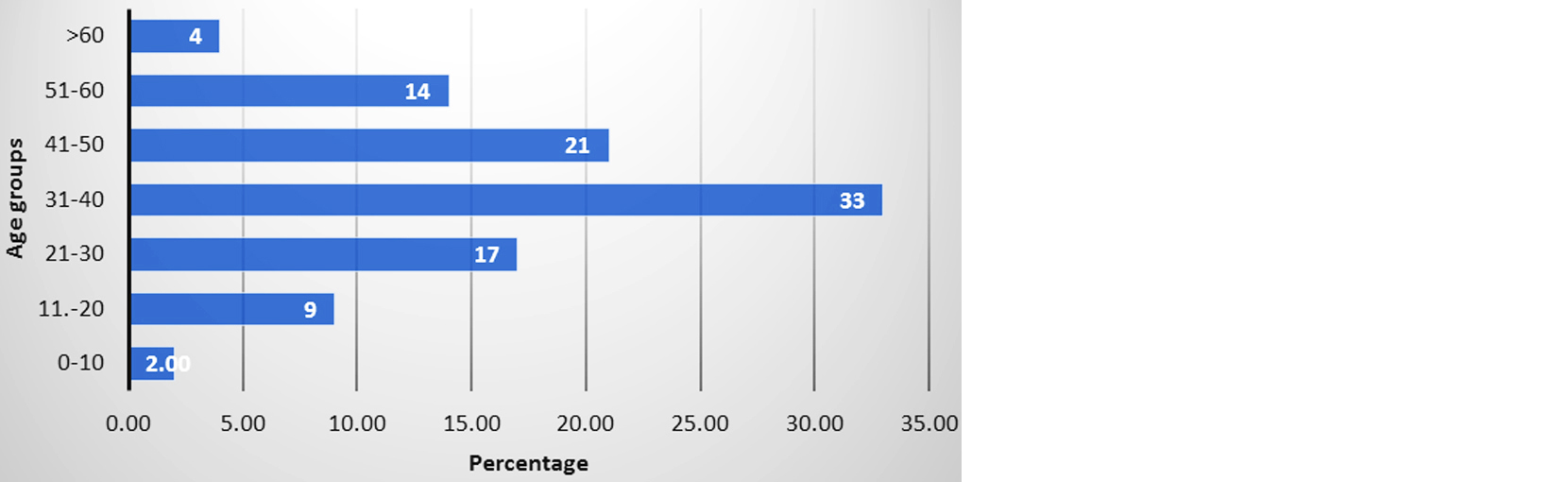
Figure 3: Age distribution of soft tissue tumors.
Table 1: Showed the sub-categorisation of adipocytic tumors based on differentiation.
|
Adipocytic tumors
|
No. of cases
|
%
|
|
Benign
|
126
|
100
|
|
Intermediate
|
0
|
0
|
|
Malignant
|
0
|
0
|
|
Total
|
126
|
100
|
Showed the sub-classification of benign adipocytic tumors in the Figure 4.
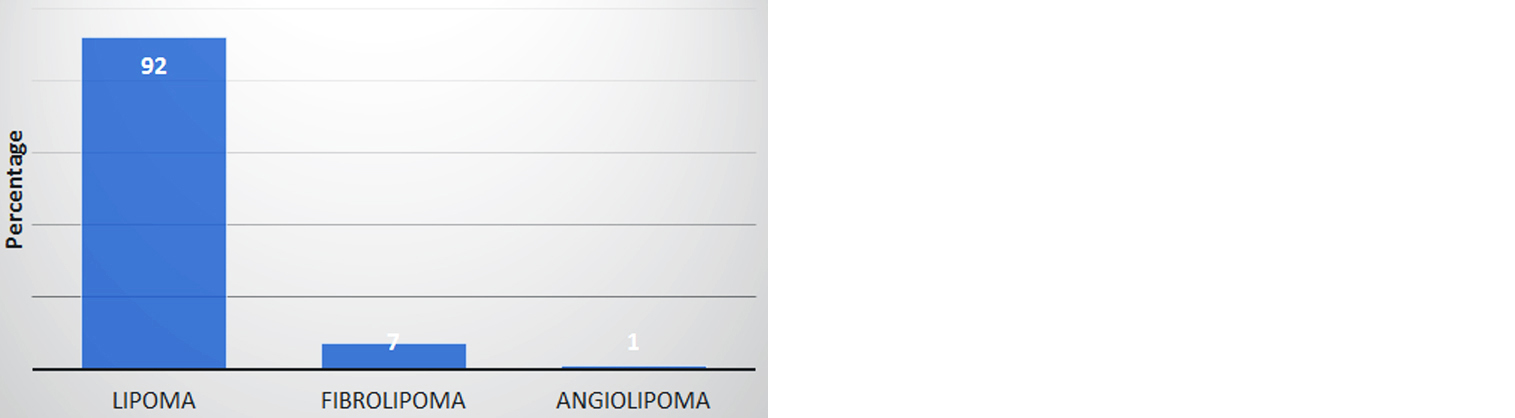
Figure 4: Subtypes of benign adipocytic tumors.
Table 2: Distribution of fibrohistiocytic tumors according to histologic differentiation.
|
Fibrohistiocytic tumors
|
No. of cases
|
%
|
|
Benign (No. of cases)
|
5
|
30
|
|
|
Keloid (1)
|
|
|
Fibroma (3)
|
|
|
Dermatofibroma (1)
|
|
Intermediate
|
8
|
47
|
|
|
Benign fibrous histiocytoma (5)
|
|
|
Fibromatosis (2)
|
|
|
Dermatofibrosarcoma protuberans (1)
|
|
Malignant
|
4
|
23
|
|
|
Low grade fibromyxoid sarcoma(1)
|
|
|
Spindle cell sarcoma (1)
|
|
|
Adult type fibrosarcoma (1)
|
|
|
Fibromyxoid sarcoma (1)
|
|
Total
|
17
|
100
|
Table 3: Distribution of vascular tumors based on differentiation.
|
Vascular tumors
|
No. of cases
|
%
|
|
Benign (Hemangioma)
|
32
|
100
|
|
Intermediate
|
0
|
0
|
|
Malignant
|
0
|
0
|
|
Total
|
32
|
100
|
Table 4: Distribution of peripheral nerve sheath tumors based on differentiation.
|
Peripheral nerve sheath tumors
|
No. of cases
|
%
|
|
Benign
|
25
|
96
|
|
|
Schwannoma (12)
|
|
|
Neurofibroma (12)
|
|
|
Neuroma (1)
|
|
|
Malignant
|
1
|
4
|
|
|
Olfactory neuroblastoma (1)
|
|
Total
|
26
|
100
|
Table 5: Distribution of tumors of uncertain differentiation.
|
Tumors of uncertain differentiation
|
No. of cases
|
%
|
|
GCT of tendon sheath
|
1
|
17
|
|
Granular cell tumor
|
3
|
50
|
|
Hamartoma
|
2
|
33
|
|
Total
|
6
|
100
|
Table 6: Distribution of soft tissue tumors according to the site of presentation.
|
Sites
|
Histopathological diagnosis
|
|
Adipocytic
|
Fibro-histiocytic
|
Vascular
|
Peripheral nerve sheath tumors
|
Miscellan-eous
|
|
No. of cases
(%)
|
No. of cases (%)
|
No. of cases (%)
|
No. of cases (%)
|
No. of cases
(%)
|
|
Head and neck
|
45 (37)
|
5 (30)
|
15 (47)
|
11 (42)
|
3 (50)
|
|
Upper limb
|
23 (18)
|
5 (30)
|
7 (22)
|
9 (35)
|
2 (33)
|
|
Lower limb
|
28 (22)
|
7 (40)
|
5 (16)
|
4 (15)
|
0
|
|
Back
|
9 (7)
|
0
|
2 (6)
|
1 (4)
|
0
|
|
Abdomen
|
11 (9)
|
0
|
2 (6)
|
0
|
0
|
|
Axilla
|
7 (5)
|
0
|
0
|
0
|
0
|
|
Chest and breast tissue
|
3 (2)
|
0
|
1 (3)
|
1 (4)
|
0
|
|
Vulva
|
0
|
0
|
0
|
0
|
1 (17)
|
|
Total
|
126 (100)
|
17 (100)
|
32 (100)
|
26 (100)
|
6 (100)
|
Discussion
Soft tissue tumors are a group of mesenchymal neoplasms encompassing all tumors originating from the adipose tissue, neural tissue, vascular tissue and fibroblasts [1]. Reporting of soft tissue tumors based on histological features alone is a diagnostic difficulty for a general pathologist. Ancillary studies like immunohistochemistry and molecular mutational studies should be employed for an accurate diagnosis and subtyping of soft tissue tumors [1, 2].
Demography
Gender distribution
In the present study, male: female ratio was found to be 1.1:1 with a slight male preponderance. Other studies were Konkani et al - 1.56:1; Solanki et al - 1.18:1; Anitha et al - 1.1:1; Bharti et al - 1.55:1; and Janaki et al - 1.2:1 [3-7]. From these observation, it is seen that the incidence of soft tissue tumors in this study, is slightly higher in males compared to females similar to other studies.
Age distribution
In the present study, it was observed that 33% of the tumors occurred in the 31-40 years age group. The second common age group affected was 41-50 years with 21% of cases (Table 8).
Table 8: Comparison of age distribution.
|
Study group
|
31-40 Years (% of cases)
|
41-50 Years (% of cases)
|
|
Konkani et al [3]
|
20
|
28
|
|
Solanki et al [4]
|
15
|
28
|
|
Kumari et al [5]
|
47
|
14
|
|
Ramnani et al [6]
|
28
|
15
|
|
Janaki et al [7]
|
23
|
20
|
|
Present study
|
33
|
21
|
From the above comparison with different studies, it is observed that soft tissue tumors occur frequently in the 30-50 years age group.
Adipocytic tumors
In the present study, it was observed that benign soft tissue tumors outnumbered the intermediate and malignant categories. Among adipocytic tumors, 100% of the cases were classical lipomas. Similar observations were made by Chakrabati et al who in their study have stated that 83.7% of tumors were benign classical lipomas. Fibrolipomas (7%) and angiolipomas (1%) were the other subtypes of lipomas observed in this study. Chakrabati et al in their study, have observed that fibrolipomas were the second common type of benign lipomas constituting 16.3% of the cases [8].
100% of these cases of lipoma occurred in the subcutaneous site (classical lipomas). Other variants of benign lipomas described in literature, include intramuscular lipomas, intermuscular lipomas, parosteal/periosteal lipomas, synovial lipomatosis (Lipoma arborescens), chondroid lipomas, myolipomas, lipoblastomas and intracranial lipomas [9]. In the present study, the most common site of subcutaneous lipomas were observed in the head and neck region which contributed to 37% of the total cases of benign lipomas. In the present study, we have not reported any tumor in intermediate and malignant categories during the study period.
Rarely, lipomas can be seen associated with certain syndromes namely Gardner syndrome, Madelung disease and adiposis dolorosa [1, 10, 11]. Most common chromosomal rearrangements seen in lipomas include structural abnormalities of 12q, 13p and 6p chromosomes [12]. MDM2 mutational studies are employed for differentiating between well differentiated lipomatous tumors and benign lipomas in addition to the histomorphological findings [12].
Fibrohistiocytic tumors
In the present study, it is observed that intermediate category of tumors (47%) were frequently reported compared to the benign (30%) and malignant (23%) categories. Solanki et al [4] in their study of 170 cases of soft tissue tumors observed that in the fibrohistiocytic category of tumors, malignant tumors were commonly seen compared to benign and intermediate categories. Konkani et al [3] in their study on 105 cases of soft tissue tumors have reported that, benign and intermediate categories were more common compared to the malignant category of fibrohistiocytic tumors.
Common fibrous histiocytoma or simply dermatofibroma is the most common benign fibrohistiocytic type of tumors. Several morphological variants described in the literature include, lipidized, hemosiderotic, keloidal, granular cell, palisading, atrophic, clear cell, myxoid, lichenoid, balloon cell and signet ring cell variants among others [13]. Few case reports of metastasizing variant of fibrous histiocytoma have been documented in the literature [14].
The tumors of fibrohistiocytic origin which belong to the intermediate category includes, dermatofibrosarcoma protuberans, giant cell fibroblastoma, plexiform fibrous histiocytoma, soft tissue giant cell tumor of low malignant potential [1]. In the present study, we have reported 5 cases of benign fibrous histiocytoma and one case of dermatofibrosarcoma protuberans. One of the morphologic variants of dermatofibrosarcoma protuberans (DFSP) is that of a pigmented tumor known as Bednar tumor. The Bednar tumor varies from the classical DFSP in the amount of pigmented dendritic cells with the classical morphology of DFSP [1].
Majority of the DFSPs will have a specific translocation t [17, 22] involving a supernumerary ring chromosome and translocation of genes PDGFβ with COL1A1. Because of this gene translocation, certain tyrosine kinase inhibitors like Imatinib Mesylate are being therapeutically implicated in the chemotherapy of DFSPs [1].
Vascular tumors
In the present study, only benign vascular tumors were reported during the study period. Janaki et al in their study on 204 cases of soft tissue tumors over a period of 4 years have reported that among vascular tumors, benign category of tumors were reported frequently with an incidence percentage of 100 [7]. Solanki et al in their study on 170 cases, have observed that among vascular lesions, benign tumors account for 100% of the cases similar to this study [4].
Molecular mutations have minimal role in the diagnosis of vascular tumors. Few of the intermediate grade tumors like epithelioid hemangioendotheliomas have been shown to be associated with a signature chromosomal rearrangements like WWTR1-CAMTA1 and YAP1-TFE3 [1-3].
Peripheral nerve sheath tumors
In the present study, it was observed that 96% of the peripheral nerve sheath tumors were of the benign category. Solanki et al have reported similar incidence of benign tumors accounting for 92% of the peripheral nerve sheath tumors [4]. Konkani et al in their study have reported only benign tumors (100%) [3]. The most common benign tumors of peripheral nerve sheath origin include schwannomas, ancient schwannomas, cellular schwannomas, neurofibromas, plexiform neurofibromas, neuromas and perineuriomas [1]. The malignant category of tumors includes malignant peripheral nerve sheath tumor (MPNST) and malignant Triton tumor which is a heterologous tumor composed of MPNST admixed with tumor cells showing skeletal muscle differentiation [1].
Conclusion
Soft tissue tumors are not uncommon tumors and account for 5.2% of cases among the routine histopathological specimens. Most common soft tissue tumors observed are adipocytic tumors, vascular tumors, fibrohistiocytic and peripheral nerve sheath tumors. Among these category of tumors, benign lesions outnumber the intermediate and malignant categories. Soft tissue tumors are most common among the 30-50years age group with a slight male preponderance. This study is presented here to understand the demography and the spectrum of soft tissue tumors observed in a tertiary care centre.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] WHO classification of tumours editorial board. Soft tissue and bone tumours. 5th ed., Lyon (France): International agency for research on cancer; 2020.
[2] Anderson WJ, Jo VY. Diagnostic immunohistochemistry of soft tissue and bone tumors: An update on biomarkers that correlate with molecular alterations. Diagnostics. 2021; 11:690.
[3] Konkani MJ, Menapara CB. Morphological spectrum of soft tissue tumors in a tertiary care hospital affliated with a teaching institute: A 4 years retrospective study. Indian J Pathol Oncol. 2019; 6:471–475.
[4] Solanki D, Mangar D. Study of histopathological pattern of soft tissue tumors in a tertiary care centre of Gandhi Nagar, Gujarat. Tropical J Pathol Microbiol. 2018; 4:604–609.
[5] Kumari MKSA. Spectrum of soft tissue tumors based on histomorphology. Medpulse Int J Pathol. 2017; 3:36–39.
[6] Ramnani B. Clinicopathological profile of benign soft tissue tumors; Study in a tertiary care hospital in Western India. 2014; 8:1–4.
[7] Janaki M, Arora KVS, Rani S, Kumar MP, Krupal S. Morphological study of soft tissue tumors. Int J Res Health Sci. 2015; 3:364–368.
[8] Chakrabati PR, Chakravarti S, Pandit A, Agarwal P, Dosi S, et al. Histopathological study of soft tissue tumors; A three year experience in tertiary care centre. Indian J Pathol Oncol. 2015; 2:141–149.
[9] Johnson CN, Ha AS, Chen E, Davidson D. Lipomatous soft-tissue tumors. J Am Acad Orthop Surg. 2020; 26:779–788.
[10] Nandakumar G, Morgan JA, Silverberg D, Steinhagen RM. Familial polyposis coli: clinical manifestations, evaluation, management and treatment. Mt Sinai J Med. 2004; 71:384–391.
[11] Wortham NC, Tomlinson IP. Dercum's disease. Skinmed. 2005; 4:157–162.
[12] Chrisinger JSA. Update on lipomatous tumors with emphasis on emerging entities, unusual anatomic sites, and variant histologic patterns. Surg Pathol Clin. 2009; 12:21–33.
[13] Alves JVP, Matos DM, Barreiros HF, Bartolo EAFLF. Variants of dermatofibroma - a histopathological study. An Bras Dermatol. 2014; 89:472–477.
[14] Doyle LA, Fletcher CDM. Metastasizing “benign” cutaneous fibrous histiocytoma- a clinicopathologic analysis of 16 cases. Am J Surg Pathol. 2013; 37:484–495.