Full Text
Introduction
Anaesthesia in parturient is unique and requires highest degree of care [1]. In the recent decades there has been worldwide shift in obstetric anaesthesia practice in favor of the regional anaesthesia, among which spinal anaesthesia being most popular [2].
Spinal anaesthesia was introduced by German Surgeon Karl August Bier in 1893 into clinical practice. Its popularity is due to advantages like –relative simplicity, rapidity, certainty, duration, low failure rates, minimal side effects, easy to perform, an awake mother, least exposure of mother and fetus to anaesthetic complications like aspiration, failed intubation and bradycardia, acidosis in neonate [2]. In fact, spinal block has been found to provide faster recovery, superior analgesia and less nausea and vomiting in the immediate postoperative period as compared to general anesthesia [3].
But, like any other anaesthetic technique, it is not devoid of complications, among which most common being hypotension [2]. Maternal hypotension is detrimental to both mother and fetus [4]. The incidence of hypotension has been reported to be as high as 85% in patients undergoing caesarean section under spinal anesthesia [5]. The hypotension following spinal block is primarily due to preganglionic sympathetic blockade resulting in vasodilation and pooling of blood in the affected areas. This reduces the cardiac preload and hence the cardiac output. Patient leg elevation, head down tilt and use of pressure stockings augment venous return and cardiac output [5].
Manual uterine displacement and pelvic tilt have been used in maternal hypotension during spinal anesthesia [6]. However all these methods have only limited role in treating hypotension. Preloading with I.V crystalloids or colloid solution is a standard practice for prevention of hypotension after spinal anesthesia, but this practice has been found to be ineffective when used alone, without concomitant use of vasopressor drugs. So use of vasopressor agents in conjugation with fluid preloading appears to be more logical approach to correct it [5]. Hypotension can lead to decreased utero placental blood flow, impaired fetal oxygenation with asphyxial stress and fetal acidosis and maternal symptoms of low cardiac output such as nausea, vomiting, dizziness and decreased consciousness [7]. Prompt treatment of hypotension with intravenous fluids or vasopressor is necessary to avoid these detrimental maternal and neonatal effects.
Phenylephrine is a pure α agonist which stimulates α1- adrenergic receptors by direct effect [8]. Ephedrine and mephentermine, both are mixed sympathomimetic amines that act both directly and indirectly on α and β adrenergic receptors. Phenylephrine is has quicker peak effect, less of fetal acidosis than ephedrine and mephentermine. But the drawback with this drug is the reduction in heart rate. The role of ephedrine has been challenged because of potential complications like tachycardia, tachyphylaxis and fetal acidosis [9]. Thus it is clear that the absolute supremacy of one vasopressor over the others has not yet been established unieqivocally, though arguments have been extended in favour of each vasopressor from time to time. Current study aimed to compare the efficacy of IV bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial blood pressure following anaesthesia for caesarean section.
The objectives of study was to compare the effect of phenylephrine, ephedrine and mephentermine, and for maintenance of arterial pressure during spinal anaesthesia for caesarean section. APGAR score in neonates at 1min and 5min, and to compare incidence of bradycardia, nausea, vomiting and shivering in mother.
Methodology
This is a randomized double blinded comparative clinical study done on Obstetric patients admitted in Cheluvambha hospital attached to Mysore medical college posted for Elective and emergency LSCS under spinal anesthesia, during the period of February 2021 to February 2023. This study was done on 30 patients in each group.
This study included the parturients scheduled for elective and emergency lower segment caesarean section aged between 20-35 years, height >150cm, with ASA class II. Parturients with baseline systolic blood pressure between 100-140 mmHg and diastolic blood pressure between 70-89 mmHg were included in the study.
We excluded from the study, the parturients with medical complications like diabetes mellitus, cardiovascular diseases, severe anemia, and cerebrovascular diseases; weight more than 70 kg, parturients with obstetrical complications like antepartum haemorrhage, pregnancy induced hypertension, cord complications (nuchal cord or cord prolapse), fetal malformations or malpresentations, and parturients with autonomic neuropathy, spinal deformities, other neurological diseases, infections in the lumbar area, signs of fetal distress, coagulation abnormalities and hypovolemia due to any cause . After thorough pre-anesthesia checkup all the patients sufficing the inclusion criteria were selected, procedure of spinal anesthesia and purpose of the study was explained and informed written consent was taken.
Intravenous access was secured with 18G IV cannula in non-dominant hand, Parturients were pre-loaded with Ringers lactate 15ml/kg. Multipara monitor was attached and baseline vital parameters (Pulse, SBP, DBP, MAP) and SpO2 was noted. Patients were put into the left lateral position and under all aseptic precautions spinal anaesthesia was performed at L2-3 or L3-4 interspace. The skin was infiltrated with 2ml of 2 percent local anaesthesia (lignocaine) and then using a 25 gauge Quincke needle pointing cephalad all patients in the study received 2cc (10mg) of 0.5% inj. bupivacaine Heavy(Preservative free) after free flow of CSF. After giving Spinal Anaesthesia, patient will be positioned supine, and 15 degree wedge will be placed under right hip to produce left uterine displacement oxygen @5litre/min was administered by using face mask. After induction, patients were divided into 3 groups of 30 subjects each with the help of randomization (by using shuffled closed opaque envelope technique). Reduction in systolic blood pressure (SBP) of more than 20% below the base line or fall in SBP less than 90mm of Hg and it is treated with:
Group P – Phenylephrine 100mcg
Group E –Ephedrine 6mg
Group M –Mephentermine 6mg
Spinal anesthesia was given and hypotension was treated with the respective drugs in each group. The hemodynamic parameters like SBP, DBP, MAP, HR, respiratory parameters like SpO2 were recorded as primary outcome. APGAR score at 1 and 5 min were recorded. (Figure 1) Adverse events like hypotension, bradycardia, nausea, vomiting, shivering were recorded as secondary outcome.
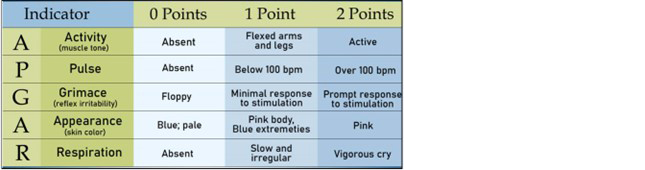
Figure 1: Showing APGAR score.
Statistical analysis
Data was analyzed using SPSS 22 software. Any p-value less than 0.05 was considered to be significant.
Results
The study was on the comparison of intravenous bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anesthesia in caesarian section, showed the following hemodynamic changes, APGAR score results and adverse events in each group. In our study, majority (56.7%) of females were in the age group of 21-25 years, followed by 43.3% of females in 26-29 group. Distribution of SBP after giving vasopressor till 10min was compared among three groups (Table 1). There was a significant fall in systolic blood pressure at onset of hypotension (p<0.05), on intergroup comparison rise of systolic blood pressure at 1,2 and 4 min after administration of the vasopressor is highly significant (p<0.01) and significant (p<0.05) at 6min in phenylephrine group compared to ephedrine and mephentermine group. The intergroup comparison showed that there was a rise of diastolic blood pressure at 1,2, 4 and 6min after administration of the vasopressor and the results were highly significant(p<0.01) in phenylephrine group compared to ephedrine and mephentermine group (Table 2).
Table 1: Showing distribution of systolic blood pressure after giving vasopressor till 10 min.
|
Baseline
(onset of hypotension)
mm Hg
|
Group P Mean &
standard
deviation
|
Group E
|
Group M
|
P/E
p value
|
P/M
p value
|
M/E
p value
|
|
81.4 (9.9)
|
83.7 (9.9)
|
82.1 (9.6)
|
0.03
|
0.02
|
0.04
|
|
1
|
121.3 (13.5)
|
119 (15.6)
|
118.6 (14.3)
|
0.003
|
0.005
|
0.78
|
|
2
|
122.2 (17.5)
|
120.5 (17.7)
|
114.5 (20.3)
|
0.019
|
0.013
|
0.89
|
|
4
|
122.8 (14.4)
|
120.7 (14.3)
|
111.2 (14.1)
|
0.001
|
0.004
|
0.91
|
|
6
|
123.4 (13.6)
|
121.3 (15.1)
|
113 (13.5)
|
0.03
|
0.05
|
0.91
|
|
8
|
122.4 (13.3)
|
119.4 (14.2)
|
113.2 (13.7)
|
0.8
|
0.7
|
0.9
|
|
10
|
118.2 (12.8)
|
118.7 (14.2)
|
112.9 (13.5)
|
0.9
|
0.9
|
0.77
|
Table 2: Showing distribution of DBP after giving vasopressor till 10min.
|
Baseline
(onset of hypotension)
mm Hg
|
Group P Mean &
standard
deviation
|
Group E
|
Group M
|
P/E
p value
|
P/M
p value
|
M/E
p value
|
|
54.7 (5.9)
|
53.1 (5.9)
|
52.7 (5.9)
|
0.05
|
0.01
|
0.03
|
|
1
|
76.5 (12.2)
|
75.1 (10.5)
|
73.3 (11.2)
|
0.003
|
0.005
|
0.78
|
|
2
|
77.3 (13.8)
|
75.9 (12.4)
|
72.8 (14.0)
|
0.019
|
0.013
|
0.89
|
|
4
|
78.6 (12.5)
|
76.3 (13.4)
|
73.1 (14.0)
|
0.001
|
0.004
|
0.91
|
|
6
|
79.4 (10.6)
|
77.1 (10.3)
|
72.7 (10.1)
|
0.03
|
0.05
|
0.91
|
|
8
|
79.7 (9.7)
|
77.9 (9.2)
|
70.2 (8.5)
|
0.8
|
0.7
|
0.9
|
|
10
|
79.2 (10.7)
|
77.4 (10.4)
|
70.7 (11.5)
|
0.9
|
0.9
|
0.77
|
Mean heart rate was raised in all three groups at the onset of hypotension. But after administration of the study drug there was a significant (p<0.05) drop of heart rate at 1, 2, 4 min and highly significant (p<0.001) drop in the HR at 6, 8 and 10min in phenylephrine group compared Ephedrine and mephentermine group (Figure 2). MAP showed a significant increase (p<0.05) at 1,2,4,6 and 8min in phenylephrine group compared to Ephedrine and mephentermine group. All the three groups had APGAR score ≥7 at 1min which was statistically in significant (p>0.05). Two patients in Group P had bradycardia and treated with Inj. atropine 0.6 mg and none in Group E and Group M. Four patients in Group E and three patients in Group M had vomiting and were treated with Inj ondensetron 4mg. One patient in Group P, two patients in Group E and one patient in Group M had shivering (Figure 3).
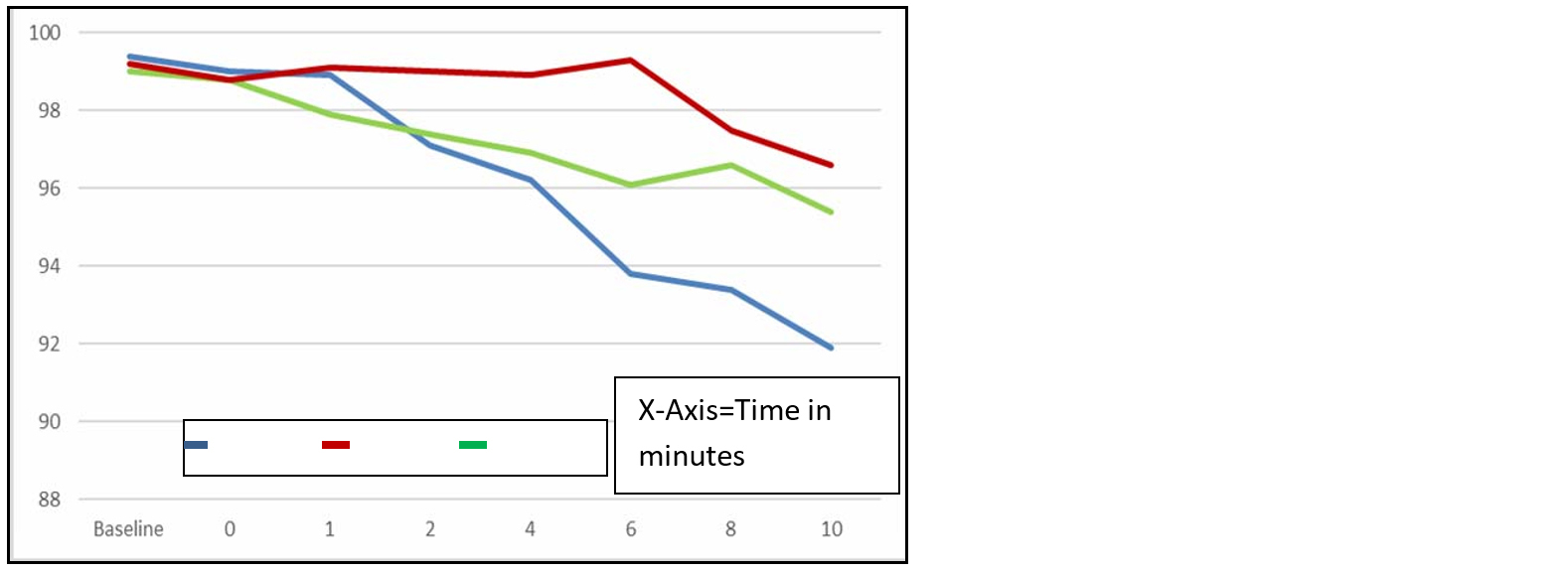
Figure 2: Showing distribution of heart rate after giving vasopressor till 10min.
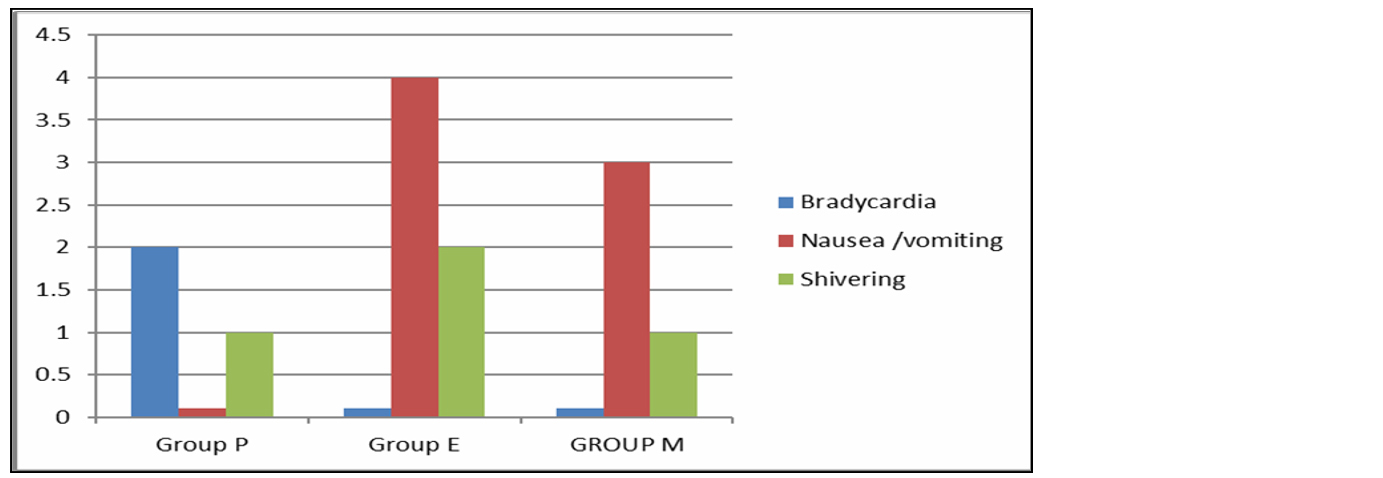
Figure 3: Showing distribution of adverse effects among the three groups.
Discussion
Obstetric anesthesia is faced with challenges of providing anesthesia for caesarean section and care for both mother and the unborn baby. In spite of numerous advantages of spinal anesthesia, it has few complications. Among which most common is hypotension which can severely affect both mother and fetus. Sympathetic blockage resulting in vasodilation is the primary cause of fall in arterial blood pressure and decreased venous return, exacerbated by aorta caval compression leading to hemodynamic sequelae especially hypotension in up to 85% of parturient which is major concern. So use of vasopressor agents in conjugation with fluid preloading appears to be more logical approach to correct it [1-3].
Vasopressors are nowadays becoming one of the mainstays of management of spinal hypotension. Prophylactic use of vasopressors, intramuscular and subcutaneous routes rule out the possibility of dose titration and may result in either inadequate treatment or more seriously hypertension. Intravenous infusion and bolus of vasopressors has advantage of side to side monitoring of patient response, better flexibility and greater margin of safety. However infusions have been associated with large amount of drug used, increasing the possibility of side effects and toxicity. Various vasopressors are available for counteracting spinal hypotension, each with different pharmacological profile [3, 4]. The current study was undertaken to compare the efficacy of IV bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure following spinal anesthesia in caesarean section. We chose equipotent dose of phenylephrine 100mcg, ephedrine 6mg and mephentermine 6mg in our study.
Group P (n=30) received inj. phenylephrine 100mcg intravenous whenever hypotension occurred. This was comparable to study by Dokania et al [5] and Tridib et al [10] wherein they considered dose of 100mcg of phenylephrine. Group E (n=30) received inj. ephedrine 6mg intravenously at onset of hypotension. This was comparable to study by Sinha et al [11] and Das et al [12] they used same dose 6 mg ephedrine. The dose 6mg mephentermine was comparable to study conducted by Tridib et al [10].
Based on previously published work, we chose the dosages of vasopressors in our study approximately equipotent. Thomas et al [13] in their similar randomized trial study reported that bolus phenylephrine 100mcg is as effective as ephedrine 5mg in restoring maternal blood pressure above 100 mm Hg. Sahu et al [14], Ganeshanavar et al [2] and Dokania et al [5] carried out studies with phenylephrine (100 mcg), ephedrine(6 mg) and mephentermine (6mg) and Thomas et al [13] studied phenylephrine (100mcg) and ephedrine (6mg) boluses with similar dosages as our study which is comparable.
The mean SBP at onset of hypotension was 81.4, 83.7 and 82.1 in Groups P, E and M respectively. We found that in our study all the three vasopressor effectively maintained arterial pressure within baseline value after administration. Though when inj. phenylephrine hydrochloride was used there was a statistically highly significant (p<0.003) rise in systolic blood pressure, within 1min, 2, 4min and significant (p<0.05) at 6min compared to ephedrine and mephentermine which is comparable to the study of Devender Dua et al [1] (p<0.05). This quicker control of hypotension in phenylephrine group attributed to the peak effect of drug, which is within one minute whereas ephedrine has 2-5 min and mephentermine has 5min.
The mean DBP at onset of hypotension was 54.5, 53.1 and 52.7 in Groups P, E and M respectively. The rise in DBP in phenylephrine group is highly significant (p<0.001) 1,2 and 4min and significant (p<0.05) at 6min. No significant changes observed in ephedrine and mephentermine group. Our study was comparable to study conducted by Sahu et al, [14] where there was significant (p<0.05) rise in DBP at 6min. Ganeshanavar et al [2] drawn similar results of significant rise in DBP (p<0.05) at 2, 4 and 6 in their study which is comparable to our study.
Mean arterial pressure in our study was found to be higher in phenylephrine group as compared to other two group up to time interval of 6- 8 min (p<0.01). With respect to blood pressure, the observation in the present study were in agreement with the findings reported by Sahu et al. [14] The results obtained in our study can be explained on the cardiovascular effects of the three vasopressors used to maintain the blood pressure during spinal anesthesia. Phenylephrine is pure α agonist, whereas ephedrine and mephentermine have got mixed action directly and indirectly on α and β receptors. Our study results are in good correlation with similar studies conducted by Thomas et al [13], Ngan Kee et al [15] using IV boluses of either phenylephrine or ephedrine and observed that phenylephrine is as effective as ephedrine in treating hypotension in partureints following SAB.
Heart rate raised in all three study groups at onset of hypotension. The mean heart rate was 99.4, 99.0 and 99.2 in Group P, E and M respectively. But, after the administration of study drug, there was highly significant (p<0.001) reduction in Heart rate at 6,8 and 10 min interval in Group P as compared to both Group M and E. At rest of intervals, it was statistically non – significant. Dokania et al [5] reported significant drop in HR at 4 min interval in Group P compared to other group E and M.
The results of our study are in accordance with the pharmacological actions of the vasopressor agents used. Phenylephrine is a pure α adrenergic agonist. It causes reflex bradycardia by baroreceptor stimulation due to an increase in the pressure resulting in inhibition of the tonic discharge of the vasoconstrictor nerves and excitation of the vagal innervation (Mary’s law). Ephedrine stimulates the α and β. Receptors directly as well as indirectly by causing release of endogenous catecholamines. This dual action greatly results in increase in force of contraction and heart rate [4].
In our study APGAR score at 1 and 5 min interval showed no statistical differences among the groups. The APGAR score at 1 and 5min after delivery of baby were ≥7 and similar among the three study groups. Thomas et al [13], Sahu et al [14] and Ngan Kee et al [15] observed clinical neonatal outcome APGAR score ≥7 in all neonates which is comparable to our study. The incidence of bradycardia in Group P is 6%, i.e., 2 patients at 6 and 8 min. It was not seen in any other group. This was comparable with study conducted by Dokania [5] in which they had bradycardia in group P at 4 min and 6 min. Four patients in Group E (13%), two patients (10%) in Group M and none Group P developed intraoperative nausea and vomiting during hypotension. The absence of nausea and vomiting in Group P and reduced incidence in Group M and E in our patients was probably result of treating hypotension, immediately and effectively which is comparable with study conducted by Fauzia Shifaat et al [4] reported absence of nausea and vomiting.
Conclusion
All the three vasopressors in the present study, phenylephrine, ephedrine and mephentermine effectively maintained arterial blood pressure in IV bolus form during subarachnoid block for caesarean section and can be safely used to treat hypotension. Phenylephrine has fast acting but short lived normotensive in comparison to ephedrine and mephentermine. Phenylephrine caused significant reduction in heart rate compared to ephedrine and mephentermine which may be advantageous in cardiac patients in whom tachycardia is undesirable. All drugs did not have any significant adverse effects clinically on mother and fetus.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Devender D, Rashida J, Deepa G, Parmar VS, Ankit J. Comparison of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section. Int J Pharma Sci Res. 2014; 5:2412–2417.
[2] Ganeshanavar A, Ambi US, Shettar AE, Koppal R, Ravi R. Comparison of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section. J Clin Diagn Res. 2011; 5:948–952.
[3] Cooper DW, Carpenter M, Mowbray P, Desira WR, Ryall DM, et al. Fetal and maternal effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. J Am Soc Anesthesiol. 2002; 97:1582–1590.
[4] Shifaat F, Syed SI, Gupta S, Danish Q, Wani HA. Comparison of ephedrine, mephentermine and phenylephrine for maintenance of blood pressure during spinal anaesthesia. Int J Med Res. 2016; 2:51–58.
[5] Dokania S, Gurung R, Jain A. Comparison of IV bolus phenylephrine, ephedrine and mephentermine for maintenance of hemodynamic status and its effect on fetal outcome during spinal anesthesia in cesarean section. Artificial Intell Med. 2019; 6:28–36.
[6] Greene NM, Brull SJ. The cardiovascular system. In: Butterworth J (ed.), Physiology of spinal anaesthesia. 4th ed. Baltimore: Williams and Wilkins. 1993; 85:85–199.
[7] Bhardwaj N, Jain K, Arora S, Bharti N. A comparison of three vasopressors for tight control of maternal blood pressure during cesarean section under spinal anesthesia: Effect on maternal and fetal outcome. J Anaesth Clin Pharmacol. 2013; 29:26.
[8] Puthenveettil N, Sivachalam SN, Rajan S, Paul J, Kumar L. Comparison of norepinephrine and phenylephrine boluses for the treatment of hypotension during spinal anaesthesia for caesarean section – A randomised controlled trial. Indian J Anaesth. 2019; 63:995.
[9] Mahajan L, Anand LK, Gombar KK. A randomized double-blinded comparison of ephedrine, phenylephrine and mephentermine infusions to maintain blood pressure during spinal anaesthesia for cesarean delivery: The effects on fetal acid-base status and haemodynamic control. J Anaesth Clin Pharmacol. 2009; 25:427.
[10] Saravanan S, Kocarev M, Wilson RC, Watkins E, Columb MO, et al. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in caesarean section. Br J Anaesth. 2006; 96:95–99.
[11] Thomas DG, Robson SC, Redfern N, Hughes D, Boys RJ. Randomized trial of bolus phenylephrine or ephedrine for maintenance of arterial pressure during spinal anaesthesia for Caesarean section. Br J Anaesth. 1996; 76:61–65.
[12] Choudry T, Mitra M, Shailendra K, Basu M. A comparative study on the role of phenylephrine and mephentermine in the treatment of hypotension during spinal anaesthesia for caesarean section. J Res Med Dent Sci. 2020; 8:56–66.
[13] Bhattarai B, Bhat SY, Upadya M. Comparison of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anesthesia in cesarean section. J Nepal Med Assoc. 2010; 49:23–28.
[14] Das S, Potli S, Madhusudhana R, Krishnamurthy D. A comparative study of phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section. IOSR-J Dent Med Sci. 2015; 14:80–85.
[15] Ngan WDK. Phenylephrine Vs ephedrine for maintaining blood pressure during spinal anaesthesia for non-elective caesarean section. J Assoc Anaesth Great Br Irel. 2008; 63:1319–1326.