Orginal Research
2024
June
Volume : 12
Issue : 2
Evaluation of ligament and meniscal injuries following knee trauma by MRI and its correlation with arthroscopy
Bhavani HG, Furtado R, Linyu V, Akami K, Naik S
Pdf Page Numbers :- 148-152
Bhavani HG1, Renny Furtado1, Visar Linyu1,*, Kewecho Akami2, and Shweta Naik1
1Department of Radiology, Goa Medical College and Hospital, Bambolim-403202, Goa, India
2Department of General Surgery, Dr. Ram Manohar Lohia Hospital, New Delhi-110001, India
*Corresponding author: Dr. Visar Linyu, Department of Radiology, Goa Medical College and Hospital, Bambolim-403202, Goa, India. Email: visarlinyu566@gmail.com
Received 20 January 2024; Revised 29 February 2024; Accepted 14 March 2024; Published 20 March 2024
Citation: Bhavani HG, Furtado R, Linyu V, Akami K, Naik S. Evaluation of ligament and meniscal injuries following knee trauma by MRI and its correlation with arthroscopy. J Med Sci Res. 2024; 12(2):148-152. DOI: http://dx.doi.org/10.17727/JMSR.2024/12-28
Copyright: © 2024 Bhavani HG et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Magnetic resonance imaging (MRI) is a non-invasive, quick and convenient investigation for evaluation of ligament and meniscal pathologies of the knee joint. Although arthroscopy is an invasive procedure it is considered the gold standard for evaluating injuries to menisci and ligaments and can be used for both diagnostic and therapeutic purpose. The purpose of this study was to evaluate cruciate ligament and meniscal injuries following knee trauma by MRI and correlate the findings with arthroscopy.
Materials and methods: This was a prospective study conducted at our institution including 61 patients with clinically suspected ligament and meniscal injury of knee. All the patients initially underwent MRI and subsequent arthroscopy. The location, type and grade of meniscal and ligament tears on MRI were recorded and later correlated with arthroscopic findings.
Results: The right knee joint was involved in 65.6 % and the left knee in 34.4 % of cases. The anterior cruciate ligament was the most commonly injured structure. The sensitivity, specificity and accuracy of MRI in detecting anterior cruciate ligament injury were 100%, 71.4% and 96.72 % respectively, posterior cruciate ligament injury (100%, 100% and 100% respectively), medial meniscus injury (100%, 78.8% and 88.5% respectively) and lateral meniscus injury (100%, 90.5% and 93.44% respectively).
Conclusion: MRI is highly sensitive and accurate in detection of cruciate ligament and meniscal tears. A good correlation was obtained between MRI and arthroscopic findings in this study. MRI used as a screening tool prior to arthroscopy helps in avoiding negative diagnostic arthroscopy.
Keywords: anterior cruciate ligament; posterior cruciate ligament; medial meniscus; lateral meniscus; arthroscopy
Full Text
Introduction
The knee joint is one of the most important weight bearing joints of the body, capable of performing complex and extensive movements. Injury to the knee joint is commonly seen due to repetitive activities, trauma and sports activities. Injury to the ligaments and menisci of the knee can lead to impairment of the patient’s daily activities making it paramount importance to treat these injuries. Magnetic resonance imaging (MRI) allows multiplanar imaging of knee joint and is the non-invasive modality of choice in evaluation of ligament and meniscal pathologies of knee joint. Lack of ionizing radiation, excellent soft tissue contrast, multiplanar imaging capabilities, absence of beam hardening artefacts and non-invasive nature are some of the advantages of MRI over other modalities. It provides detailed information about the bony cortex, cartilage, bone marrow, menisci, ligaments, tendons and synovium [1, 2]. Pulse sequences used in MRI have advantage in terms of speed and spatial resolution. Arthroscopy is an operative technique that allows the visualisation and treatment of internal structures of the knee joint. Although arthroscopy is considered the gold standard for evaluating injuries to menisci and ligaments, it is an invasive procedure. MRI reduces the number of negative arthroscopies and helps in selecting patients for therapeutic oriented arthroscopy [2].
Aims of the study were to compare the diagnostic efficacy of MRI with arthroscopy in cruciate ligament and meniscal injuries of knee, and to evaluate the types and incidence of ligament and meniscal injuries following knee trauma.
Materials and methods
This was a prospective study including 61 patients conducted at Goa Medical College and Hospital over a period of 18 months from January 2021 to July 2022. The subjects included in this study consist of patients with clinically suspected ligament and meniscal injury of knee. The age group of patients in our study was 20–40 years. Patients with age less than 20 years and more than 40 years were excluded from the study. Patients who had previously undergone arthroscopy with repair of menisci and ligaments were also excluded. Ethical approval was taken from the Institutional Ethics Committee of our institution before commencement of the study.
Imaging technique
MRI of knee joint was performed using 1.5 Tesla Siemens Magnetom Avanto machine. A slice thickness of 3 to 4 mm in sagittal, coronal and axial planes was chosen for the scan. The field of view was between 14-16 cms. The sequences included were axial and sagittal T2 weighted (T2W) images (TR-3580 and TE-85) without fat saturation, sagittal proton density (PD) image (TR-3580 and TE-15) without fat saturation, coronal T2W fat saturated image (TR-5480 and TE-31) and 3-D gradient echo sequence (for cartilage). Oblique sagittal sections were performed in some cases of suspected anterior cruciate ligament (ACL) injury for better delineation of ACL tears.
Interpretation of images
MR images were reviewed by senior radiologists in our department. Meniscal tears were evaluated for their plane (outer 2/3rd or inner 1/3rd), site, grade and configuration. ACL and PCL tears were evaluated for type and site. The MRI findings were reported to the orthopedic surgeons. Prior knowledge of complete description of the tear helped the surgeons in optimal visualization and probing of the area with abnormal signal. Cases were discussed with the treating orthopedic surgeons for follow up of all cases. Arthroscopy was used as the gold standard and MRI findings were compared with it to know the sensitivity, specificity and accuracy of MRI for detection of cruciate ligament and meniscal tears.
Statistical analysis
Statistical data analysis was done using SPSS 21.0 version. The arthroscopic findings were taken as standard reference for comparison to MRI findings. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy were calculated by kappa statistics. This data was analyzed for correlation between MRI results and arthroscopic findings by kappa statistics.
Results
Our study included 61 patients of which 46 were men and 15 were women. The right knee joint was involved in 65.6 % and the left knee was involved in 34.4 % of cases. Table 1 shows the validity of MRI in correlation with arthroscopy. Graph showing various tears detected in our study is depicted in Figure 1.
Table 1: Validity of MRI in comparison to arthroscopy.
|
|
Sensitivity
|
Specificity
|
PPV
|
NPV
|
Accuracy
|
|
ACL
|
100%
|
71.4%
|
96.4%
|
100%
|
96.72%
|
|
PCL
|
100%
|
100%
|
100%
|
100%
|
100%
|
|
Medial meniscus
|
100%
|
78.8%
|
80%
|
100%
|
88.5%
|
|
Lateral meniscus
|
100%
|
90.5%
|
82.6%
|
100%
|
93.44%
|
Abbreviations: PPV: Positive predictive value, NPV: Negative predictive value, ACL: Anterior cruciate ligament, PCL: Posterior cruciate ligament.
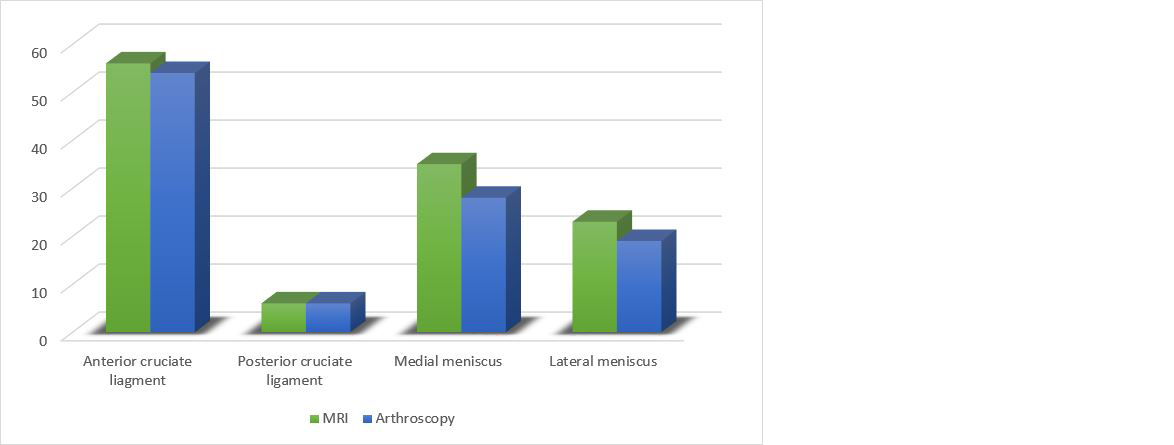
Figure 1: Graph showing number of various tears found on MRI and arthroscopy.
Anterior cruciate ligament injury
There were 56 ACL tears detected on MRI and 54 were seen on arthroscopy (Figures 2a-c). Femoral site tears were the most common site of ACL injury on MRI as well as arthroscopy. There were 46 acute tears of ACL and 10 were of chronic type.
Posterior cruciate ligament injury
There were 6 tears of PCL on MRI and all six were seen on arthroscopy. The mid-segment tear of PCL was the most common type (Figure 2d).
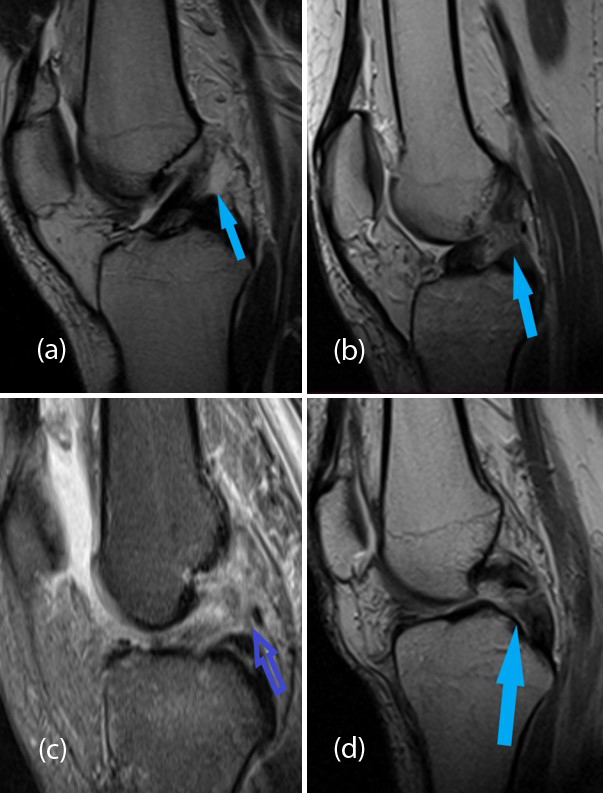
Figure 2: Proton density images show partial tear of ACL at its femoral attachment (a), Complete tear of ACL at its mid substance (b), Complete tear of ACL involving entire length (c), Complete tear of PCL at its mid-segment (d).
Medial meniscus injury
In our study, we found 35 medial meniscus tears on MRI and on arthroscopy 28 tears were seen (Figures 3a-c, 4c, d). Longitudinal tears were the most common type of tears seen on MRI in the medial meniscus and was seen in 17 patients on MRI. Other types of medial meniscus tears seen on MRI were complex tear (6 patients), bucket handle tear (5 patients), horizontal tear (4 patients) and radial tear (3 patients). Subsequently performed arthroscopy could identify 11 longitudinal tears and 5 complex tears. All other types of tears seen on MRI were also identified on arthroscopy. The posterior horn of medial meniscus was the most common involved site of injury.
Lateral meniscus injury
There were 23 lateral meniscus tears detected on MRI out of which 19 cases were seen on arthroscopy (Figures 3d, 4a, b). Radial tears were the most common type of tear seen on MRI in the lateral meniscus and was seen in 11 patients on MRI. Other types of lateral meniscus tears seen on MRI were horizontal tear (4 patients), longitudinal tear (3 patients), complex tear (3 patients) and bucket handle tear (2 patients). Subsequently performed arthroscopy could identify 7 radial tears. All other types of tears seen on MRI were also identified on arthroscopy. The body was found to be the most common site of lateral meniscus injury in our study.
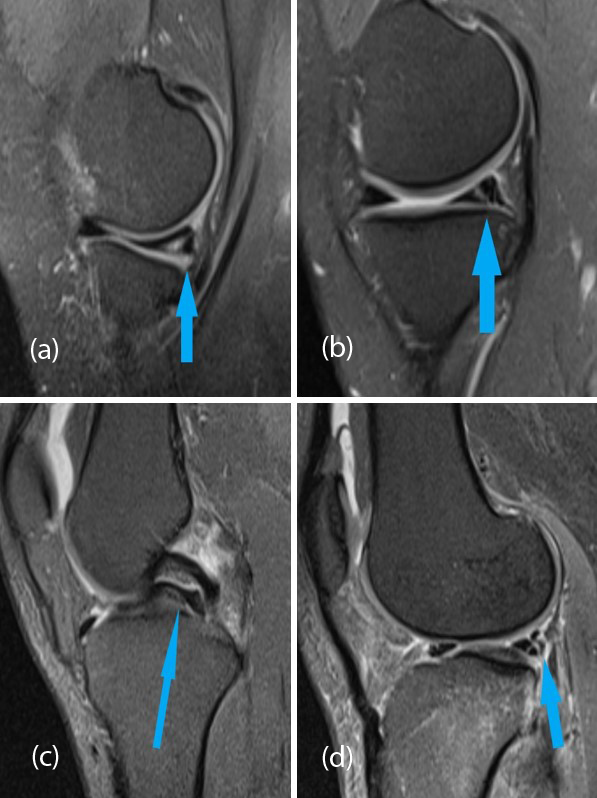
Figure 3: Proton density images show longitudinal horizontal (a) and vertical tear (b) of posterior horn of medial meniscus, Double PCL sign formed by flipped inner fragment of torn meniscus in bucket handle tear (c), Complex tear of posterior horn of lateral meniscus (d).
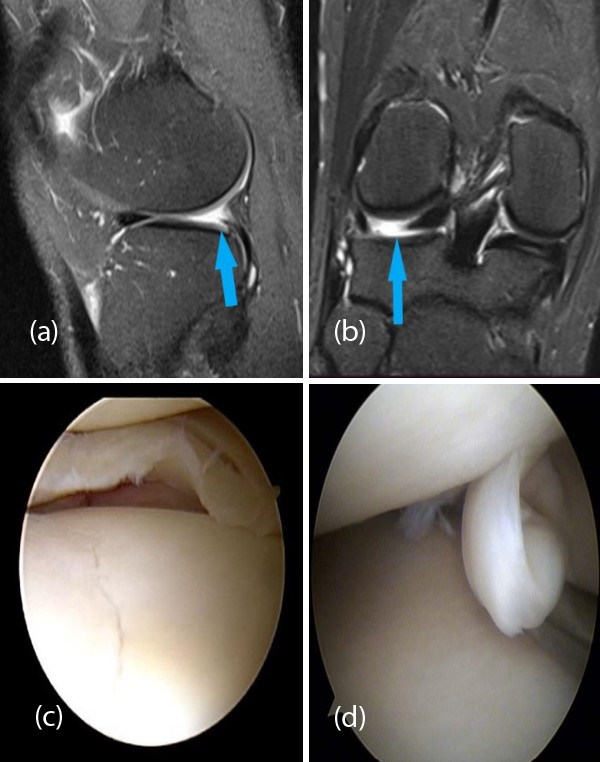
Figure 4: Proton density sagittal (a) and coronal (b) images shows radial tear of posterior horn of lateral meniscus. Arthroscopic images show longitudinal tear (c) and bucket handle tear (d).
Collateral ligament injury
There were 17 medial collateral ligament injuries in our study out of which 6 were grade I injury, 10 were grade II injury and 1 was grade III injury. There were 12 lateral collateral ligament injuries out of which 4 were grade I injury, 6 were grade II injury and 2 were grade III injury.
Discussion
Anterior cruciate ligament injury
ACL injury was seen in 56 patients on MRI and 54 were identified on arthroscopy making it the most common structure involved in knee trauma. Sahni et al. also reported ACL tear as the most common finding in knee injury [3]. Tears at the femoral attachment was the most common site and acute tears were more common than chronic tears. We found that MRI sensitivity, specificity and accuracy in detecting ACL tears was 100%, 71.4% and 96.72% respectively, when compared to arthroscopy. These findings correlate well with previous studies in literature [4-6, 18].
Posterior cruciate ligament injury
In our study, we found 6 patients with PCL injury. All injuries were seen on arthroscopy. Tears at the midsubstance was the most common site. We obtained sensitivity, specificity and accuracy of MRI in detecting PCL tears of 100%, 100% and 100% respectively, when compared to arthroscopy. Dhall et al. [5] and Sanjay et al. [18] also reported similar sensitivity of 100 % and specificity of 100% of MRI in diagnosing PCL tears. According to Singh et al. [7] MR imaging has a pooled sensitivity, specificity, and accuracy of 98.72%, 98.94%, and 98.84% respectively for tears of PCL. Roberts et al. [8] found that the midsegment of the PCL was the most common site involved in PCL injury. Sonin et al. [9] also found that midsubstance tear is the most common site of injury of the PCL. These findings were similar to the findings in our study. Grover et al. [10] found that MRI is most reliable in the diagnosis of PCL tears. On sagittal images, PCL tears were better seen because anatomical disruption of the ligament or detachment of the ligament from the insertion site is visualised better on sagittal image.
Medial meniscus injury
Medial meniscus injury was found in 35 patients on MRI in our study and 28 cases were confirmed on arthroscopy. The posterior horn was the most common involved site involved in medial meniscus injury. The sensitivity, specificity and accuracy of MRI in detection of medial meniscal injury with respect to arthroscopy were 100 %, 78.8% and 88.5% respectively. These findings correlate well with previous studies in literature [4,11,12,18]. In our study, we found that longitudinal tears were the most common type of tear involving the medial meniscus. De Smet et al. [13] also detected that longitudinal tears were more common than other types of tears because of a higher rate of false positive diagnosis and lower PPV while diagnosing a longitudinal tear of the medial meniscus. They hypothesised that the longitudinal tear of the medial meniscus which was identified on MRI, was actually healed. Therefore, these tears were not confirmed by arthroscopy. Weiss et al. [14] supported De Smet's hypothesis by stating that majority of the longitudinal tears were present in the outer one-third of the meniscus, which has a rich vascular supply.
Lateral meniscus injury
In our study, 23 cases of lateral meniscus tears were detected on MRI and 19 cases were confirmed on arthroscopy. The body was found to be the most common site of lateral meniscus injury in our study. The sensitivity, specificity and accuracy of MRI in detection of lateral meniscus injury when compared to arthroscopy were 100 %, 90.5% and 93.44% respectively. Similar findings were seen in previous studies [12,15,16,18]. We found that overall, MRI had a higher sensitivity but not specificity in the detection of meniscal tears. This discrepancy was explained by some studies previously. Carrino et al. [17] discovered in arthroscopy that the posterior horn in medial meniscus tear was a hidden area especially the area between the medial collateral ligament and the intercondylar attachment of the posterior horn. For this reason, a tear in these areas was missed during arthroscopy. Mink et al. [4] explained the possible reasons for the discrepancy between the sensitivity and specificity of MRI in the detection of meniscal injury. These include: i) Misconceived normal anatomical structures like meniscofemoral ligaments. ii) Meniscal tears may be mimicked by osteochondral flap avulsion lesions. iii) Presence of loose bodies iv) Difficulty in visualizing radial meniscal tears on MRI.
Limitations: The sample size of the study could have been more, thereby giving more precise results. In this study arthroscopy was used as the gold standard; however, arthroscopy is not 100 % accurate and is operator dependent.
Conclusion
Accurate evaluation of knee joint injury is crucial for management and outcome. Any delay in treatment can lead to chronic debility, especially in the younger age group. MRI is a non-invasive, quick and convenient investigation for diagnosing internal derangement of knee joint. It is highly sensitive and accurate in detection of cruciate ligament and meniscal tears. A good correlation was obtained between MRI and arthroscopic findings in this study. MRI used as a screening tool prior to arthroscopy helps in avoiding negative diagnostic arthroscopy.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Reicher MA, Bassett LW, Gold RH. High-resolution magnetic resonance imaging of the knee joint: pathologic correlations. AJR Am J Roentgenol. 1985; 145:903–909.
[2] Beltran J, Noto AM, Mosure JC, Weiss KL, Zuelzer W, et al. The knee: surface-coil MR imaging at 1.5 T1. Radiology. 1986; 159:747–751.
[3] Sahni G, Kumar S, Rehncy JS, Aggarwal S. Diagnostic arthroscopy compared to magnetic resonance imaging in evaluation of meniscal and ligament tears of knee. Natl J Physiol Pharm Pharmacol. 2022; 12:166–169.
[4] Mink JH, Levy T, Crues JV. Tears of the anterior cruciate ligament and menisci of the knee: MR imaging evaluation. Radiology. 1988; 167:769–74.
[5] Dhall A, Agrawal S, Thukral BB, Swarup A. MRI evaluation of knee trauma and its correlation with clinical examination and arthroscopic findings. Int J Radiol Diagn Imaging. 2021; 4:84–87.
[6] Gupta RK, Sagar S, Swarup A, Dube AS, Kumar A, et al. Arthroscopic correlation of ligamentous injury in adult knee with magnetic resonance imaging. J Orthop Dis Traumatol. 2020; 3:109–111.
[7] Singh J, Garg L, Shrimali R, Setia V, Gupta V. MR imaging of knee with arthroscopic correlation in twisting injuries. Indian J Radiol Imaging. 2004; 14:33–40.
[8] Roberts CC, Towers JD, Spangehl MJ, Carino JA, Morrison WB. Advanced MR imaging of the cruciate ligaments. Radiol Clin North Am. 2007; 45:1003–1016.
[9] Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, et al. Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology. 1994; 190:455–458.
[10] Grover JS, Bassett LW, Gross ML, Seeger LL, Finerman GA. Posterior cruciate ligament: MR imaging. Radiology. 1990; 174:527–530.
[11] Elvenes J, Jerome CP, Reikeras O, Johansen O. Magnetic resonance imaging as a screening procedure to avoid arthroscopy for meniscal tears. Arch Orthop Trauma Surg. 2000; 120:14–16.
[12] Polly DW, Callaghan JJ, Sikes RA, McCabe JM, McMahon K, et al. The accuracy of selective magnetic resonance imaging compared with the findings of arthroscopy of the knee. J Bone Joint Surg Am. 1988; 70:192–198.
[13] De Smet AA, Graf BK. Meniscal tears missed on MR imaging: relationship to meniscal tear patterns and anterior cruciate ligament tears. AJR Am J Roentgenol. 1994; 162:905–911.
[14] Weiss KL, Morehouse HT, Levy IM. Sagittal MR images of the knee: a low-signal band parallel to the posterior cruciate ligament caused by a displaced bucket-handle tear. AJR Am J Roentgenol. 1991; 156:177–179.
[15] Cheung LP, Li KC, Hollett MD, Bergman AG, Herfkens RJ. Meniscal tears of the knee: accuracy of detection with fast spin-echo MR imaging and arthroscopic correlation in 293 Patients. Radiology. 1997; 203:508–512.
[16] Saseendran R, Ahamed MS, Mohanan K, Verghese JP. MRI with arthroscopic correlation in meniscal injuries of knee. Int J Contemp Med Surg Radiol. 2018; 3:70–73.
[17] Carrino JA, Schweitzer ME. Imaging of sports-related knee injuries. Radiol Clin North Am. 2002; 40:181–202.
[18] Sanjay N, Shanthappa AH, Kurahatti A, Kumaar A. Comparison of clinical, magnetic resonance imaging (MRI) and arthroscopic findings in assessment of cartilage defects and internal derangement of knee. Cureus. 2023; 15:e40110.