Full Text
Introduction
Pulmonary nocardiosis is caused by Nocardia species, which are gram positive aerobic bacteria belonging to actinomycetes group. There are almost 100 species of genus Nocardia. Most human infections are due to Nocardia asteroids complex. Pulmonary nocardiosis is common due to inhalational route of transmission. They can also cause cutaneous, central nervous system (CNS), ocular, skeletal or disseminated infection. They usually affects immunocompromised individual.
Pulmonary nocardiosis is a rising bacterial infection, with a high chance of misdiagnosis. Pulmonary nocardiosis is a major cause of morbidity and mortality in immunocompromised patients. Lack of suspicion, non-specific clinic-radiological presentation (often mimicking tuberculosis and fungal infections), diagnostic intricacies, and lack of systematic reporting are the probable reasons that have hindered the true estimation of its incidence, worldwide. Pulmonary nocardiosis and disseminated forms of the infection are opportunistic diseases occurring mainly in patients deficient in T cell-mediated immunity.
We report here a case of pulmonary nocardiosis in an immunocompetent individual which is quite rare.
Case Report
35 years-old female with no known co morbidities presented to outpatient Department of Respiratory Medicine, Velammal Medical College & RI, Madurai with symptoms of productive cough, shortness of breath and chest pain for the past 3 months. Patient was started on empirical ATT (RHEZ) outside 3 months ago for the above mentioned complaints, based on chest skiagram. On examination, there was reduced intensity of breath sounds in left mammary, interscapular region with no added sounds. Lab investigations revealed leucocytosis with microcytic hypochromic anemia. Chest X ray showed heterogenous opacity left upper lobe (Figure 1). Computed tomography (CT) of Thorax done showed Consolidation with air broncogram in left upper lobe posterior segment with heterogenous enhancement (Figure 2). CT brain and ultrasound abdomen done were normal study. Bronchoscopy was done which showed Mucoid secretions in left upper lobe from which Bronchial wash taken (Figure 3). Transbronchial lung biopsy was taken from left upper lobe posterior segments. Bronchial wash analysis showed Filamentous Acid fast bacilli in modified AFB stain (1 % H2SO4) and culture grew Nocardia species (Figure 4).
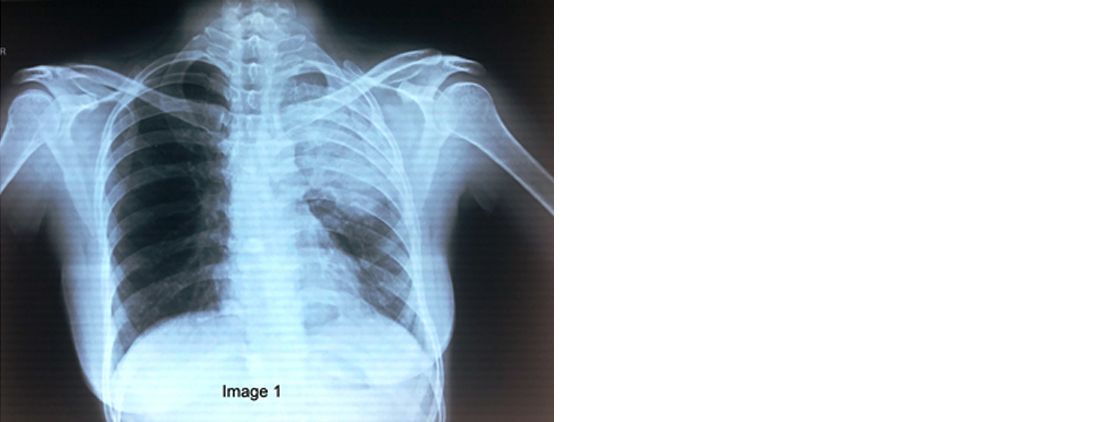
Figure 1: Chest X ray showed heterogenous opacity left upper lobe.
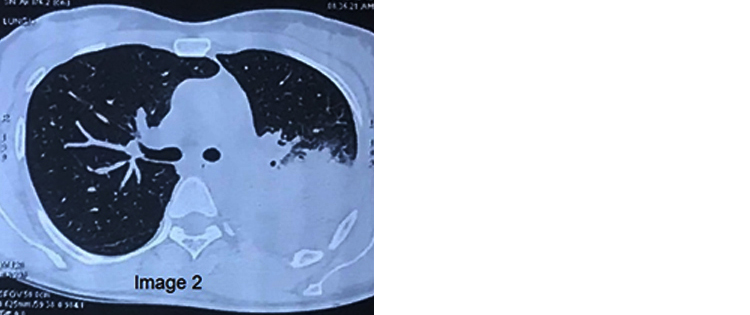
Figure 2: Computed tomography of thorax done showed consolidation with air broncogram in left upper lobe posterior segment with heterogenous enhancement.
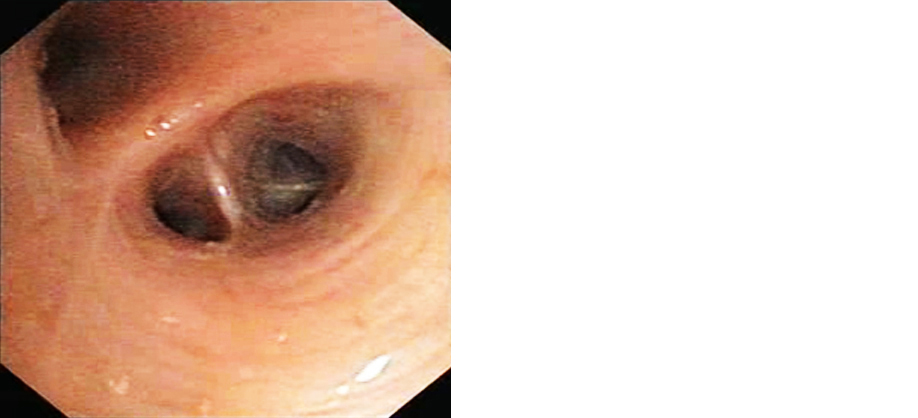
Figure 3: Bronchoscopy showed mucoid secretions in left upper lobe from which bronchial wash taken.
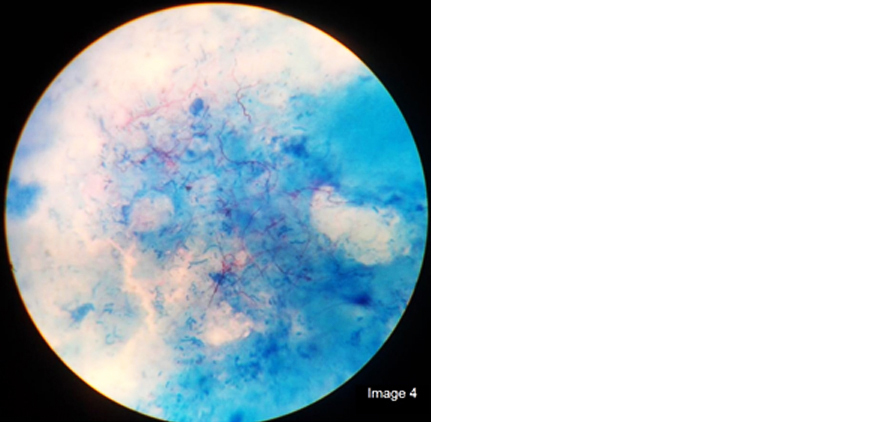
Figure 4: Modified AFB Stain (1% H2SO4)- Bronchial wash analysis showed filamentous acid fast bacilli.
Bronchial wash AFB and cytology were negative. Histopathological examination revealed chronic suppurative inflammation with presence of organisms morphologically suggestive of Nocardia (Figure 5). Patient was initiated on trimethoprim-sulphamethoxazole double strength twice daily and inj. Amikacin 15 mg/kg once daily. Renal and liver parameters were monitored weekly for 3 months and were within normal limits. Chest X ray after 4 months of treatment showed clearance of left upper lobe lesion with symptomatic improvement (Figure 6).
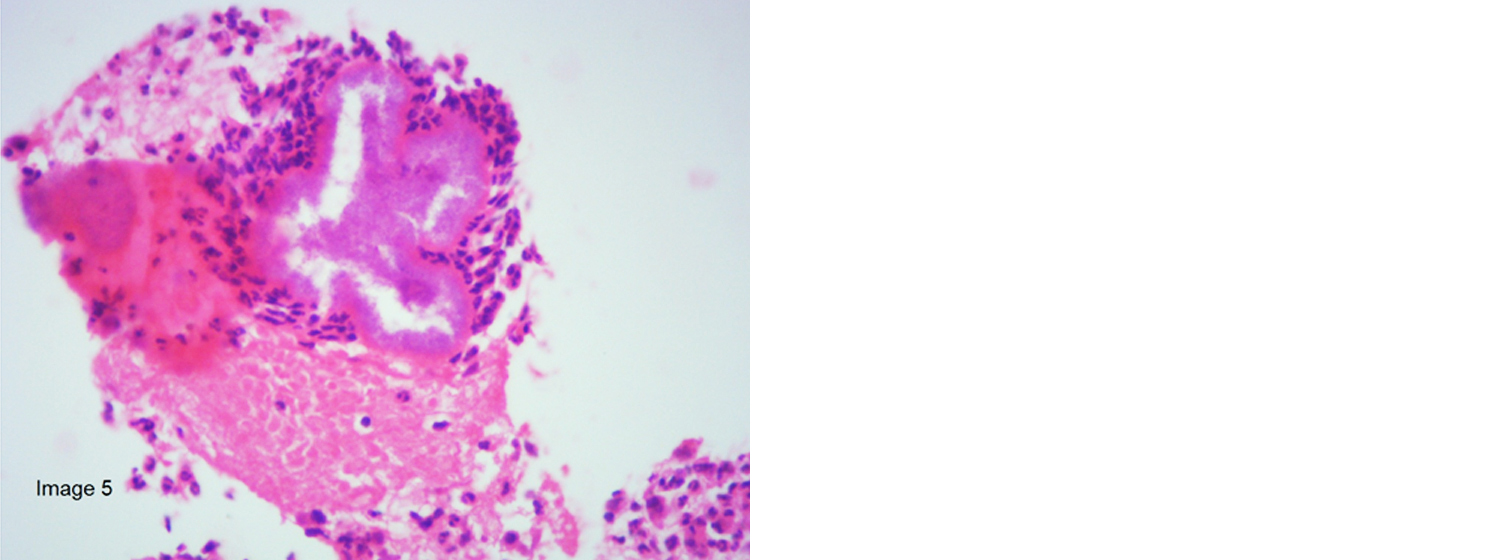
Figure 5: Histopathological examination revealed chronic suppurative inflammation with presence of organisms morphologically suggestive of Nocardia.

Figure 6: Chest X ray after 4 months of treatment showed clearance of left upper lobe lesion.
Discussion
Nocardia asteroids complex usually affects middle aged males [1]. Pulmonary nocardiosis presents as an acute, subacute, or chronic disease in patients with and without predisposing chronic conditions. Predisposing factors include patients with malignancies, human immunodeficiency virus infection and solid-organ or hematopoietic stem cell transplant and those on steroids or other immunosuppressive medications [2, 3]. The genus Nocardia are branching gram-positive, variably acid-fast, aerobic bacteria and they can fragment into rod-shaped or coccoid elements [4]. A modified Ziehl-Neelsen technique (1% sulphuric acid) is used to demonstrate Nocardia [5].
Most common symptoms in pulmonary nocardiosis include fever, weight loss, dry cough, anorexia, night sweats, dyspnea and hemoptysis. Acute presentation can be in the form of pneumonia, abscess formation, bronchopneumonia, pleural involvement and empyema. Involvement in preexisting lung cavities can produce "fungus ball" appearance in chest skiagram. Skin manifestations include superficial abscess, cellulitis, pustules, pyoderma and ulcerations. CNS involvement include cerebral nocardiosis and meningitis. Other systemic involvement includes peritonitis, epididymo-orchitis, iliopsoas, ischiorectal and perirectal abscess, endophthalmitis, retinitis, pericarditis, endocarditis, aortitis, septic arthritis and bursitis, osteomyelitis, and diffuse organ abscesses. Our patient had only pulmonary involvement in the form of left upper lobe consolidation.
Diagnosis is established by analyzing respiratory secretion and aspirate from abscess to be subjected to Modified Acid fast stain, grocott staining for demonstrating bacteria. Culture is the gold standard method of diagnosis and the culture should be observed for 2 weeks before discarding [6]. Bronchoscopy was done for our patient and bronchial wash showed Nocardia in modified Ziehl-Neelsen staining and culture grew Nocardia species.
Management of nocardial infection includes antibiotic therapy and surgery. Medical management includes Trimethoprim-sulfamethoxazole as monotherapy in mild localized infections. In case of severe pulmonary infection, CNS involvement, or disseminated infection 2 agents (such as trimethoprim-sulpamethoxazole or imepenem plus amikacin) should be used.In case of life threatening disease, 3 drugs should be considered [7]. Our patient was managed with dual antibiotic therapy. Immunocompetent patients with pulmonary or systemic nocardiosis, without CNS involvement should be treated for a minimum of 6-12 months extending to 12 months in those with CNS infection. Other agents used in nocardiosis include amikacin, imipenem, meropenem, ceftriaxone, cefotaxime, minocycline, moxifloxacin, levofloxacin, linezolid, tigecycline, and amoxicillin -clavulanic acid [8, 9].
Conclusion
Even Immunocompetent patients with atypical clinical and radiological features needs to be evaluated for Nocardia species as the virulence is high with multisystem involvement and increased mortality and morbidity.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Reed RC. Nocardiosis and actinomycosis. Medicine. 2005; 33:114–115.
[2] Young LS, Rubin RH. Mycobacterial and nocardial diseases in the compromised host. In: Rubin RH, Young LS, eds. A clinical approach to infection in the compromised host. 4th ed. New York, Kluwer Academic, 2002; pp.257–261.
[3] Long PF. A retrospective study of Nocardia infections associated with the acquired immune deficiency syndrome (AIDS). Infection. 1994; 22:362–364.
[4] McNeil MM, Brown JM. The medically important aerobic actinomycetes: Epidemiology and microbiology. Clin Microbiol Rev. 1994; 7:357–417.
[5] Lerner PI. Nocardia species, in Manedll GL, Douglas RG Jr., Bennett GE, editors: Principles and practice of infectious diseases, New York, John Wiley & Sons Inc. 1985; pp.1423–1427.
[6] Curry WA. Human nocardiosis .A clinical review with selected case reports. Arch Intern Med. 1980; 140:818–826.
[7] Restrepo A, Clark NM. Nocardia infections in solid organ transplantation: guidelines from the infectious diseases community of practice of the American society of transplantation.
[8] Garlando F, Bodmer T, Lee C, Zimmerli W, Pirovino M. Successful treatment of disseminated nocardiosis complicated by cerebral abscess with ceftriaxone and amikacin: Case report. Clin Infect Dis. 1992; 15:1039–1040.
[9] Yew WW, Wong PC, Kwan SY, Chan CY, Li MS. Two cases of Nocardia asteroids sternotomy infection treated with ofloxacin and a review of other active antimicrobial lagents. J Infect. 1991; 23:297–302.