Full Text
Introduction
Scrotal trauma, although relatively uncommon, represents a urological emergency that requires prompt evaluation and management to preserve testicular function and prevent long-term complications such as infertility, chronic orchialgia, testicular atrophy, or psychological distress [1]. The mechanism of injury is most often blunt force, resulting from road traffic accidents, falls, sports-related impacts, or interpersonal violence [2]. Due to the anatomical vulnerability of the scrotum and testes, even low-velocity trauma may cause significant internal injury, including vascular disruption, parenchymal laceration, and rupture of the tunica albuginea [3].
Clinical assessment of scrotal trauma is often challenging because signs such as swelling, tenderness, and ecchymosis are nonspecific and may obscure severe underlying injuries [4]. High-resolution ultrasonography (US) has therefore become the first-line diagnostic modality, offering rapid, non-invasive, real-time evaluation of scrotal contents with excellent soft-tissue resolution [5]. When combined with Colour Doppler imaging, ultrasonography can assess testicular perfusion and differentiate between haematocele, intratesticular hematoma, testicular rupture, testicular torsion, epididymal hematoma, and testicular avulsion [6].
Among the most serious complications of blunt scrotal trauma is testicular rupture, reported in nearly 50% of significant injuries [7]. Timely diagnosis and surgical repair ideally within 72 hours are critical for optimizing testicular salvage. Ultrasonographic signs suggestive of testicular rupture include heterogeneous echotexture, contour irregularity, and discontinuity of the tunica albuginea, while haematocele typically appears as a complex fluid collection within the tunica vaginalis [8]. Despite its high diagnostic performance, ultrasonography is not infallible; false positives and false negatives may lead to unnecessary exploration or missed injuries. Thus, correlating ultrasonographic findings with operative outcomes is essential to validate its reliability in acute trauma settings [9].
This study aimed to evaluate the diagnostic accuracy of ultrasonography in blunt scrotal trauma. A total of 30 patients presenting to the emergency department of a tertiary care teaching hospital in Maharashtra, India, over six months were included. All patients underwent clinical examination, scrotal ultrasonography, and subsequent surgical exploration, enabling direct comparison of imaging and intraoperative findings. Diagnostic performance was assessed by calculating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for key scrotal pathologies, including haematocele, testicular rupture, tunica albuginea breach, intratesticular hematoma, epididymal injury, and testicular avulsion.
The findings of this study aim to reinforce ultrasonography as an indispensable tool for timely diagnosis and surgical decision-making in acute scrotal trauma.
Materials and methods
This retrospective observational study was conducted in the Department of Radiodiagnosis at Government Medical College, Akola, a tertiary care teaching hospital in Maharashtra, India. The study included patients who presented with blunt scrotal trauma and received treatment between October 2023 to March 2024. Approval for the study protocol was obtained from the institutional departmental ethics committee. Patient confidentiality was strictly maintained, and all data were anonymized before analysis.
Male patients presenting with blunt scrotal trauma, confirmed clinically and by ultrasonographic evaluation, and who subsequently underwent surgical exploration, were included in the study. Patients with penetrating scrotal injuries, pre-existing scrotal pathology, or incomplete medical records were excluded. A total of 30 consecutive patients who met the inclusion criteria were identified from emergency department admission logs and surgical records. All eligible patients were evaluated and managed during the defined study period.
The primary exposure variable was blunt scrotal trauma, resulting from mechanisms such as motor vehicle accidents, physical assault, accidental falls, or sports-related injuries. Ultrasonography (US) served as the principal diagnostic modality and was used to identify the type and extent of scrotal injury. Surgical exploration was performed in all cases and served as the reference standard for diagnosis. Ultrasonographic findings were categorized into six major types of injury: haematocele, testicular rupture, tunica albuginea breach, intratesticular hematoma, epididymal injury, and testicular avulsion.
Data were retrospectively extracted from patient medical records, operative notes, and radiology reports. Scrotal ultrasonography was performed using a Samsung RS80 EVO ultrasonography system equipped with a 7.5–10 MHz high-frequency linear transducer with Colour Doppler capability. All ultrasonographic examinations were performed by experienced radiologists in the Department of Radiodiagnosis. Due to the retrospective nature of the study and emergency setting, formal assessment of interobserver variability was not performed. Surgical exploration was performed under anaesthesia through a transverse scrotal incision, and all intraoperative findings were documented in detail. To minimize classification bias, only patients who underwent both ultrasonography and surgical exploration were included. Radiological and operative findings were matched and compared using a standardized reporting template.
All eligible cases (n = 30) during the study period were included, representing a complete sample of scrotal trauma admissions. Due to the descriptive nature of the study, no formal sample size calculation was performed.
Statistical analysis
The diagnostic performance of ultrasonography was assessed by calculating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for each category of scrotal injury. Ultrasonography findings were compared with operative findings, which served as the diagnostic gold standard. All data analysis was descriptive, and diagnostic accuracy metrics were calculated manually based on concordance and discrepancies between ultrasonographic and intraoperative results.
Results
Among the 30 patients included in this study, motor vehicle accidents were the most frequent cause of blunt scrotal trauma, accounting for 11 cases (36.6%). This was followed by assault-related injuries in 9 patients (30%). Falls from height were observed in 6 patients (20%), while sports-related injuries were the least common, occurring in 4 patients (13.3%) (Table 1).
Table 1: Causes of blunt scrotal injuries (n=30).
|
Injuries
|
Frequency (N)
|
Percentage (%)
|
|
Assault
|
9
|
30.0%
|
|
Motor vehicle accident
|
11
|
36.6%
|
|
Sport related
|
4
|
13.3%
|
|
Fall from a height
|
6
|
20.0%
|
A total of 30 patients with blunt scrotal trauma were assessed clinically, followed by ultrasonographic evaluation and surgical exploration. Haematocele was the most frequently identified lesion on ultrasonography, detected in 18 patients (60%) and surgically confirmed in 20 patients (66.7%), with two false-negative cases. Clinically, haematocele was suspected in only 5 patients (16.7%), indicating that a substantial number of cases would have been missed without imaging. Testicular rupture was detected in 17 patients (56.7%) on ultrasonography, while surgical exploration confirmed rupture in 12 patients (40%), resulting in five false positives and no false negatives. These findings suggest that ultrasonography may overestimate testicular rupture in certain cases (Table 2).
Tunica albuginea breach was suspected on ultrasonography in 9 patients (30%), whereas surgical exploration confirmed 11 cases (36.7%), indicating two false negatives and demonstrating the limited sensitivity of ultrasonography in detecting subtle breaches. Testicular hematoma was identified sonographically in 8 patients (26.7%) but confirmed intraoperatively in only 5 patients (16.7%), resulting in three false-positive interpretations, likely due to overlapping sonographic features with haematocele or parenchymal heterogeneity. Epididymal injury was suspected on ultrasonography in 5 patients (16.7%) and confirmed during surgery in 4 patients (13.3%), yielding one false positive. Testicular avulsion was suggested by ultrasonography in 2 cases (6.7%), but only 1 case (3.3%) was confirmed surgically, resulting in one false-positive finding (Table 2).
Table 2: Clinical, ultrasonographic, and surgical findings of scrotal injuries (n = 30).
|
Lesion
|
Clinical Finding
|
US Finding
|
Surgical Finding
|
False Positives (FP)
|
False Negatives (FN)
|
|
Haematocele
|
5 (16.7%)
|
18 (60.0%)
|
20 (66.7%)
|
0
|
2
|
|
Testicular rupture
|
0 (0%)
|
17 (56.7%)
|
12 (40.0%)
|
5
|
0
|
|
Tunica albuginea breach
|
0 (0%)
|
9 (30.0%)
|
11 (36.7%)
|
0
|
2
|
|
Testicular hematoma
|
0 (0%)
|
8 (26.7%)
|
5 (16.7%)
|
3
|
0
|
|
Epididymal injury
|
0 (0%)
|
5 (16.7%)
|
4 (13.3%)
|
1
|
0
|
|
Testicular avulsion
|
0 (0%)
|
2 (6.7%)
|
1 (3.3%)
|
1
|
0
|
The diagnostic accuracy of ultrasonography was assessed by comparing sonographic findings with surgical exploration, which served as the gold standard. Ultrasonography demonstrated high sensitivity across all categories of scrotal injury, achieving 100% sensitivity for testicular rupture, intratesticular hematoma (Figure 1), epididymal injury, and testicular avulsion. Haematocele and tunica albuginea breach showed slightly lower sensitivities of 90.0% and 81.8%, respectively. Specificity values were also consistently high, with ultrasonography demonstrating 100.0% specificity for both haematocele (Figure 2) and tunica albuginea breach, while specificity was moderately lower for testicular rupture (72.2%) and intratesticular hematoma (88.0%). Epididymal injury and testicular avulsion demonstrated specificities of 96.2% and 96.6%, respectively, indicating excellent ability to correctly identify patients without the condition.
Regarding predictive performance, the positive predictive value (PPV) was highest for haematocele, tunica albuginea breach, and epididymal injury, ranging from 80.0% to 100.0%. In contrast, the PPV for testicular avulsion was lower at 50.0%, likely reflecting its rare occurrence and the increased potential for overdiagnosis. Negative predictive value (NPV) was uniformly high, reaching 100% for all injuries except haematocele (83.3%) and tunica albuginea breach (90.5%) (Table 3).
Table 3: Diagnostic accuracy of ultrasonography compared with surgical findings (n = 30).
|
US finding
|
Sensitivity
|
Specificity
|
PPV
|
NPV
|
|
Haematocele
|
90.0%
|
100.0%
|
100.0%
|
83.3%
|
|
Testicular rupture
|
100.0%
|
72.2%
|
70.6%
|
100.0%
|
|
Tunica albuginea breach
|
81.8%
|
100.0%
|
100.0%
|
90.5%
|
|
Testicular hematoma
|
100.0%
|
88.0%
|
62.5%
|
100.0%
|
|
Epididymal injury
|
100.0%
|
96.2%
|
80.0%
|
100.0%
|
|
Testicular avulsion
|
100.0%
|
96.6%
|
50.0%
|
100.0%
|
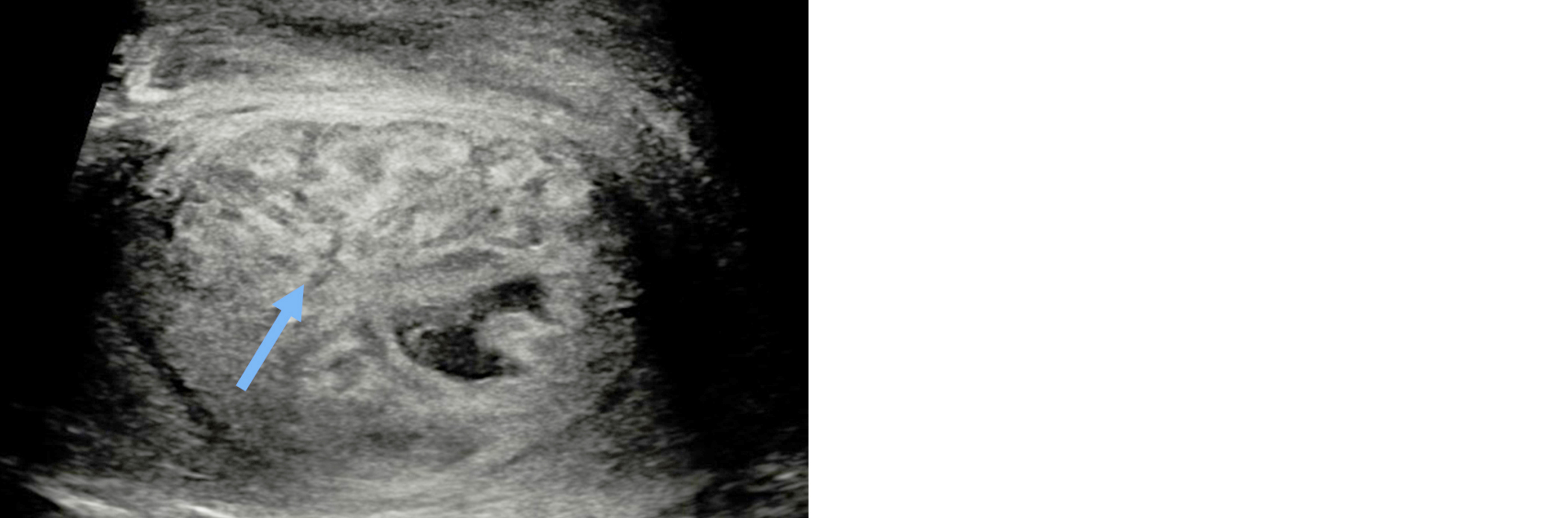
Figure 1: Transverse image in a patient with blunt trauma to the scrotum showing ill-defined heterogeneous area in right testis representing intratesticular hematoma.
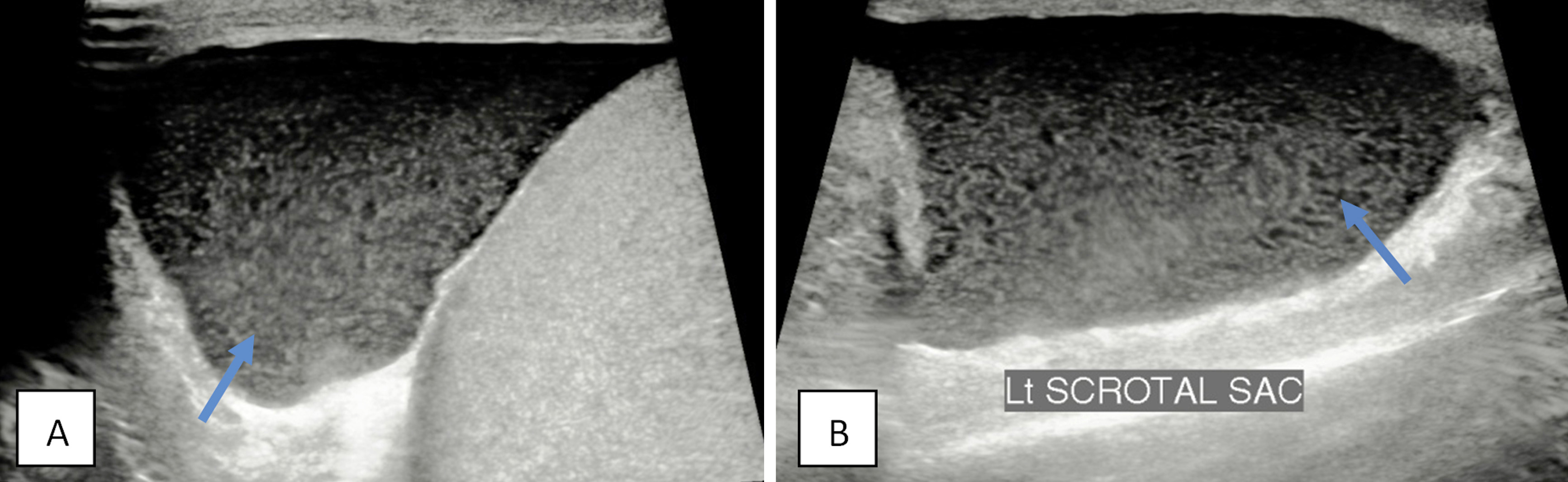
Figure 2: (a) Transverse, (b) Sagittal images in a patient with history of scrotal trauma a 2 days ago: Note echoic collection in left scrotal sac (arrow), representing a hematocoele.
Discussion
Scrotal trauma, particularly from blunt injury, presents a significant diagnostic and therapeutic challenge in emergency care. Although relatively uncommon, such injuries pose a substantial risk of complications including infertility, chronic pain, and psychological distress if not identified and managed promptly. In this study of 30 patients, we evaluated the diagnostic accuracy of ultrasonography in detecting various scrotal pathologies by comparing sonographic findings with definitive surgical exploration.
Our results demonstrate that ultrasonography is highly effective in identifying scrotal injuries, particularly haematocele, testicular rupture, and epididymal injuries. Haematocele was the most common lesion, with ultrasonography detecting 18 of the 20 surgically confirmed cases, yielding a sensitivity of 90%. This is consistent with the observations of Guichard et al. [10], who reported a sensitivity of 87% for haematocele, reinforcing the reliability of ultrasonography in identifying complex fluid collections within the tunica vaginalis. Testicular rupture, a critical consequence of blunt trauma, was identified sonographically in 17 patients and confirmed surgically in 12. While ultrasonography demonstrated excellent sensitivity (100%), specificity was lower (72.2%) due to five false-positive cases. Similar findings have been described by Guichard et al. [10], who noted that severe contusions may mimic rupture on imaging. Bhatt and Dogra [11] likewise highlighted the difficulty in distinguishing rupture from marked contusion, particularly in the acute setting.
Ultrasonography also performed well in identifying testicular hematomas and epididymal injuries, achieving 100% sensitivity for both. However, testicular hematoma exhibited a moderate positive predictive value (62.5%) due to false-positive interpretations, which may reflect overlap with haematocele or heterogeneous echotexture caused by contusions or infarction. Deurdulian et al. [12] noted that small intratesticular hematomas can be difficult to differentiate from parenchymal disruption without contrast-enhanced imaging. For tunica albuginea breach, the sensitivity in our study was 81.8%, with a specificity of 100%, indicating that while small or subtle tears may be missed, positive findings are highly reliable. These results align with the observations of Guichard et al. [10], who emphasized the difficulty of directly visualizing the tunica albuginea in the absence of associated findings.
Testicular avulsion, though rare, is a severe form of scrotal injury. Ultrasonography suggested avulsion in two cases, while surgical confirmation was obtained in only one, resulting in a PPV of 50%. Nonetheless, sensitivity and negative predictive value remained high, supporting the utility of ultrasonography in ruling out avulsion. Yusuf et al. [13] have suggested that contrast-enhanced ultrasonography (CEUS) may offer superior assessment of tissue viability in equivocal cases. Overall, the diagnostic performance of ultrasonography in our study reinforces its role as the first-line imaging modality for scrotal trauma, particularly in emergency settings where rapid surgical decision-making is required. The uniformly high negative predictive values across most injuries underscore ultrasonography’s value in excluding significant pathology and avoiding unnecessary surgical interventions. As noted by Churukanti et al. [14] and Yagil et al. [15], operator expertise and imaging equipment quality significantly influence diagnostic accuracy; in our study, this limitation was minimized by ensuring all scans were performed or reviewed by experienced radiologists, with surgical correlation serving as the reference standard.
One of the major strengths of this study is the direct comparison of ultrasonographic findings with surgical exploration in all cases, allowing precise assessment of diagnostic accuracy. Standardized scanning protocols and interpretation by experienced radiologists further strengthen the reliability of our results. However, the study also has limitations. The sample size was relatively small (n = 30), potentially affecting generalizability. Additionally, the study was conducted at a single tertiary care centre, and outcomes may differ in settings with variable operator experience or imaging resources. Advanced modalities such as CEUS were not utilized, despite their reported value in improving diagnostic accuracy in borderline cases. Overlap of multiple injuries in some patients may also have influenced accuracy metrics. Future research involving larger, multicentric cohorts and the integration of advanced ultrasonographic techniques may further validate and enhance the role of ultrasonography in the assessment of scrotal trauma.
Limitations: This study has certain limitations. First, the sample size was relatively small (n = 30), which may limit the generalizability of the results. However, blunt scrotal trauma requiring surgical exploration is an infrequent emergency presentation. Our study included all consecutive eligible patients (n = 30) presenting during the defined study period, representing a complete sample rather than a selective cohort. Similar diagnostic accuracy studies in acute scrotal trauma have reported comparable sample sizes due to the rarity of the condition. Second, Interobserver variability was not formally assessed, which may have influenced diagnostic accuracy estimates; however, all examinations were performed or reviewed by experienced radiologists. Third, the study was conducted at a single tertiary care center, and the results may not reflect outcomes in settings with variable operator expertise or imaging resources. Future studies with larger, multicentric cohorts and the inclusion of advanced sonographic techniques could further validate and refine the role of ultrasonography in the evaluation of scrotal trauma.
Conclusion
Ultrasonography is a highly effective, rapid, and non-invasive imaging modality for the assessment of blunt scrotal trauma. It demonstrates excellent diagnostic accuracy, particularly in detecting haematocele, testicular rupture, intratesticular hematoma, and epididymal injuries, and provides critical information that guides timely surgical decision-making. Although certain injuries may yield false-positive findings, the consistently high negative predictive value underscores the reliability of ultrasonography in ruling out significant pathology and preventing unnecessary surgical exploration. Based on its accessibility, diagnostic performance, and real-time capability, ultrasonography should remain the first-line imaging modality in the evaluation and management of acute scrotal trauma.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Bourke MM, Silverberg JZ. Acute scrotal emergencies. Emerg Med Clin North Am. 2019; 37:593–610.
[2] Kendall M, Oeur A, Brien SE, Cusimano M, Marshall S, et al. Accident reconstructions of falls, collisions, and punches in sports. J Concussion. 2020; 4:205970022093695.
[3] Nicola R, Carson N, Dogra VS. Imaging of traumatic injuries to the scrotum and penis. AJR Am J Roentgenol. 2014; 202:1–8.
[4] Gridley CM, Nguyen HT. The acute scrotum. In: Urological Emergencies: A Practical Approach. 2nd ed. New York: Springer, 2013; p:207–217.
[5] Mathur M, Mills I, Spektor M. Magnetic resonance imaging of the scrotum: pictorial review with ultrasonography correlation. Abdom Radiol (NY). 2017; 42:1929–1935.
[6] Paparella MT, Eusebi L, Pagliara MP, Palladino N, Sortino G, et al. Multiparametric ultrasonography in testicular emergencies: state of the art. Curr Radiol Rep. 2023; 11:109–119.
[7] Randhawa H, Blankstein U, Davies T. Scrotal trauma: a case report and review of the literature. Can Urol Assoc J. 2019; 13:67–69.
[8] Garriga V, Serrano A, Marin A, Medrano S, Roson N, et al . US of the tunica vaginalis testis: anatomic relationships and pathologic conditions. Radiographics. 2009; 29:2017–2032.
[9] Arnold MJ, Jonas CE, Carter RE. Point-of-care ultrasonography. Am Fam Physician. 2020; 101:275–285.
[10] Guichard G, El Ammari J, Del Coro C, Cellarier D, Loock PY, et al. Accuracy of ultrasonography in diagnosis of testicular rupture after blunt scrotal trauma. Urology. 2008; 71:52–56.
[11] Bhatt S, Dogra VS. Role of ultrasonography in testicular and scrotal trauma. Radiographics. 2008; 28:1617–1629.
[12] Deurdulian C, Mittelstaedt CA, Chong WK, Fielding JR. US of acute scrotal trauma: optimal technique, imaging findings, and management. Radiographics. 2007; 27:357–369.
[13] Yusuf GT, Rafailidis V, Moore S, Hawthorn B, Fang C, et al. The role of contrast-enhanced ultrasonography (CEUS) in the evaluation of scrotal trauma: a review. Insights Imaging. 2020; 11:46.
[14] Churukanti GR, Kim A, Rich DD, Schuyler KG, Lavien GD, et al. Role of ultrasonography for testicular injuries in penetrating scrotal trauma. Urology. 2016; 95:208–212.
[15] Yagil Y, Naroditsky I, Milhem J, Leiba R, Leiderman M, et al. Role of Doppler ultrasonography in the evaluation of scrotal pathology. J Ultrasonography Med. 2010; 29:11–21.
|
Author Designations:
Pankaj Asaram Badarkhe (Associate Professor); Sahebrao Bhumanna Kaslod (Assistant Professor); Payal Mahagaonkar-Badarkhe (Assistant Professor); Venkat Narsingrao Bhosle (Radiology Resident).
|